You might also like
- Personality DisordersDocument125 pagesPersonality DisordersDevendra Singh Baryah100% (2)
- Graves Disease: An Autoimmune Disorder Causing HyperthyroidismDocument35 pagesGraves Disease: An Autoimmune Disorder Causing HyperthyroidismMarianGadugdug75% (4)
- AAOS Foot & Ankle 2015Document114 pagesAAOS Foot & Ankle 2015Fasa Roshada100% (3)
- Dermatitis and HomoeopathyDocument18 pagesDermatitis and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- The Perfect Thyroid Diet Cookbook; The Complete Nutrition Guide To Managing And Healing Thyroid Symptoms For General Wellness With Delectable And Nourishing RecipesFrom EverandThe Perfect Thyroid Diet Cookbook; The Complete Nutrition Guide To Managing And Healing Thyroid Symptoms For General Wellness With Delectable And Nourishing RecipesNo ratings yet
- Thyroid DisordersDocument29 pagesThyroid DisordersEMPINo ratings yet
- Thyroid Storm: An Acute Life-Threatening Hypermetabolic StateDocument11 pagesThyroid Storm: An Acute Life-Threatening Hypermetabolic StateAndrew UtamaNo ratings yet
- 00 Obs&Gyn Clerkship-1-1Document9 pages00 Obs&Gyn Clerkship-1-1samwel daniel100% (1)
- Therapeutics: Thyroid DisordersDocument24 pagesTherapeutics: Thyroid DisordersSharas FarhadNo ratings yet
- NEURO VITAL SIGNS ASSESSMENT Procedure and ChecklistDocument12 pagesNEURO VITAL SIGNS ASSESSMENT Procedure and ChecklistMemer-alasadNo ratings yet
- Hypothyroidism: Madhuri Devdhar, MD, Yasser H. Ousman, MD, Kenneth D. Burman, MDDocument21 pagesHypothyroidism: Madhuri Devdhar, MD, Yasser H. Ousman, MD, Kenneth D. Burman, MDTatiana RamírezNo ratings yet
- Thyroid StormDocument16 pagesThyroid StormRaquid MariaNo ratings yet
- PDF document-CD8968C1BAE7-1Document22 pagesPDF document-CD8968C1BAE7-1Sean SialanaNo ratings yet
- Thyroid StormDocument36 pagesThyroid StormSabrina ShalhoutNo ratings yet
- Hyperthyroidism and ThyrotoxicosisDocument33 pagesHyperthyroidism and Thyrotoxicosiseze033No ratings yet
- Hyperthyroidism and Thyrotoxicosis - Practice Essentials, Background, PathophysiologyDocument13 pagesHyperthyroidism and Thyrotoxicosis - Practice Essentials, Background, Pathophysiologyabenezer g/kirstosNo ratings yet
- Thyroid Storm: July 2020Document9 pagesThyroid Storm: July 2020mirzaNo ratings yet
- Hyperthyroidism and Thyrotoxicosis: Practice EssentialsDocument39 pagesHyperthyroidism and Thyrotoxicosis: Practice Essentialssyl viNo ratings yet
- 2005 H Diagnostic Si TratamentDocument9 pages2005 H Diagnostic Si TratamentCaulfield DariaNo ratings yet
- Thyroid+Storm+ +StatPearls+ +NCBI+Bookshelf 1666577389538Document9 pagesThyroid+Storm+ +StatPearls+ +NCBI+Bookshelf 1666577389538Novita Sri MulyatiNo ratings yet
- Atow 496 00 01Document9 pagesAtow 496 00 01Nguyen Ngoc ChungNo ratings yet
- Research Paper On Thyroid DiseaseDocument4 pagesResearch Paper On Thyroid Diseasecwzobjbkf100% (1)
- Tyroid StormDocument10 pagesTyroid StormAfdhalia Khairunnisa SyammarhanNo ratings yet
- American Thyroid Association Guidelines For Detection of Thyroid DysfunctionDocument5 pagesAmerican Thyroid Association Guidelines For Detection of Thyroid DysfunctionUdsanee SukpimonphanNo ratings yet
- Thyroid Storm Diagnosis and Treatment ChallengesDocument7 pagesThyroid Storm Diagnosis and Treatment ChallengesKarl Angelo MontanoNo ratings yet
- Nonthyroid Surgery in The Patient With Thyroid Disease - UpToDateDocument25 pagesNonthyroid Surgery in The Patient With Thyroid Disease - UpToDateDanya BarbozaNo ratings yet
- Thyroid Surgery UpToDateDocument24 pagesThyroid Surgery UpToDatepck846737No ratings yet
- Diagnosis of HyperthyroidismDocument25 pagesDiagnosis of HyperthyroidismGuardito PequeñoNo ratings yet
- Hyperthyroidism Causes, Symptoms, Diagnosis and TreatmentDocument40 pagesHyperthyroidism Causes, Symptoms, Diagnosis and TreatmentEmmanuelNo ratings yet
- Hyperthyoidism: Anaesthetic ManagementDocument11 pagesHyperthyoidism: Anaesthetic ManagementerzaraptorNo ratings yet
- Hyperthyroidism Article PubmedDocument12 pagesHyperthyroidism Article PubmedSandu AlexandraNo ratings yet
- Endocrinology L8: Introduction To Thyroid Disease and HyperthyroidismDocument30 pagesEndocrinology L8: Introduction To Thyroid Disease and HyperthyroidismSecret ManNo ratings yet
- Medical Diagnosis (Hyperthyroidism)Document4 pagesMedical Diagnosis (Hyperthyroidism)Kenneth Smith IINo ratings yet
- Thyroid Storm May Be The Initial Presentation Of: Thyrotoxicosis in Undiagnosed Children, Particularly in NeonatesDocument8 pagesThyroid Storm May Be The Initial Presentation Of: Thyrotoxicosis in Undiagnosed Children, Particularly in NeonatesLolla MorsiNo ratings yet
- Thyroid DisorderDocument60 pagesThyroid DisorderThe AbyssinicansNo ratings yet
- Background: Excessive Release of Thyroid Hormones (THS) Hypertension Congestive Heart FailureDocument8 pagesBackground: Excessive Release of Thyroid Hormones (THS) Hypertension Congestive Heart FailureIkmal HazliNo ratings yet
- Toxic Multinodular GoiterDocument25 pagesToxic Multinodular GoiterGamer MadaNo ratings yet
- Causes, Symptoms, Diagnosis and Treatment of HyperthyroidismDocument11 pagesCauses, Symptoms, Diagnosis and Treatment of HyperthyroidismtiwiNo ratings yet
- Treatment and Guidelines Patient HyperthyroidDocument2 pagesTreatment and Guidelines Patient Hyperthyroidshana_anwarNo ratings yet
- Tiroiditis Subakut PDFDocument8 pagesTiroiditis Subakut PDFAdeh MahardikaNo ratings yet
- ThyroidDocument12 pagesThyroidrpjaymaNo ratings yet
- Fendo 05 00102Document11 pagesFendo 05 00102nita mellyniumNo ratings yet
- Hypo & HyperthyroidismDocument13 pagesHypo & Hyperthyroidismgolden fleeceNo ratings yet
- Nonthyroid Surgery in The Patient With Thyroid Disease - UpToDateDocument13 pagesNonthyroid Surgery in The Patient With Thyroid Disease - UpToDateJavier GlezqNo ratings yet
- Hyperthyroidism UpToDateDocument19 pagesHyperthyroidism UpToDatepck846737No ratings yet
- Background: Excessive Release of Thyroid Hormones (THS) Hypertension Congestive Heart FailureDocument13 pagesBackground: Excessive Release of Thyroid Hormones (THS) Hypertension Congestive Heart FailureFebria ArmaNo ratings yet
- THYROTOXICOSISDocument20 pagesTHYROTOXICOSISfig8fashion1No ratings yet
- Euthyroid Sick Syndrome - Endocrine and Metabolic Disorders - Merck Manuals Professional EditionDocument2 pagesEuthyroid Sick Syndrome - Endocrine and Metabolic Disorders - Merck Manuals Professional Editionram7676No ratings yet
- Morning ReportDocument31 pagesMorning Reports1882No ratings yet
- Endocrinology Metabolism: Management of Subclinical HyperthyroidismDocument7 pagesEndocrinology Metabolism: Management of Subclinical HyperthyroidismagungNo ratings yet
- LO&WO - Endokrin.week4 (Michael G)Document6 pagesLO&WO - Endokrin.week4 (Michael G)Michael GNo ratings yet
- Ann Int Med 2020 - HyperthiroidismDocument19 pagesAnn Int Med 2020 - HyperthiroidismKarla WevarNo ratings yet
- Thyroid Storm: An Unusual Presentation: Case ReportDocument2 pagesThyroid Storm: An Unusual Presentation: Case Reportplay_wright2084No ratings yet
- ThyrotoxicosisDocument16 pagesThyrotoxicosisFiorella Peña MoraNo ratings yet
- Management of Subclinical Hyperthyroidism: A 6-Step ApproachDocument1 pageManagement of Subclinical Hyperthyroidism: A 6-Step ApproachRovelyn CalinawaganNo ratings yet
- Thyroid Disorders GuideDocument31 pagesThyroid Disorders GuideAmmar HattemNo ratings yet
- By Talha Anwar: HyperthyroidismDocument8 pagesBy Talha Anwar: HyperthyroidismFalah NadeemNo ratings yet
- Perioperative Management of The Thyrotoxic PatientsDocument16 pagesPerioperative Management of The Thyrotoxic PatientsHub storeNo ratings yet
- Wo Week 4 (Hyperthyroidism)Document12 pagesWo Week 4 (Hyperthyroidism)Theddyon BhenlieNo ratings yet
- Hyperthyroidism, Thyroid Storm, and Graves Disease: BackgroundDocument22 pagesHyperthyroidism, Thyroid Storm, and Graves Disease: BackgroundAnonymous 3OoumAUytNo ratings yet
- ThyrotoxicosisDocument15 pagesThyrotoxicosischrysandre100% (1)
- Thyroid Disorder MGT July 2020-3Document89 pagesThyroid Disorder MGT July 2020-3robelNo ratings yet
- Ipertiroidismo SubclinicoDocument9 pagesIpertiroidismo SubclinicoMr. LNo ratings yet
- Hyperthyroidism: ThyrotoxicosisDocument17 pagesHyperthyroidism: ThyrotoxicosisDerly Barino HasdiNo ratings yet
- Bta Patient Hyperthyroidism PDFDocument4 pagesBta Patient Hyperthyroidism PDFWILLIAMNo ratings yet
- Oscillococcinum for InfluenzaDocument5 pagesOscillococcinum for InfluenzaDeepak KumarNo ratings yet
- Session 6 - Performing Abdominal ExaminationDocument33 pagesSession 6 - Performing Abdominal ExaminationOtsward OwdenNo ratings yet
- 5 Tips for Preventing Diabetes with Lifestyle ChangesDocument2 pages5 Tips for Preventing Diabetes with Lifestyle Changesmatindi galawanNo ratings yet
- Bovine Ephemeral Fever: ImportanceDocument4 pagesBovine Ephemeral Fever: ImportanceAamir AliNo ratings yet
- Chronic Pyelonephritis: Causes, Symptoms and TreatmentDocument70 pagesChronic Pyelonephritis: Causes, Symptoms and TreatmentSravani Peddagangannagari100% (1)
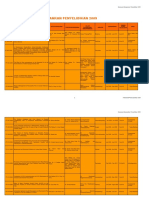
- Data Penyelidikan 2009Document86 pagesData Penyelidikan 2009Alex Phang Kean ChangNo ratings yet
- SBTP Annual Report 2018Document111 pagesSBTP Annual Report 2018RMCNo ratings yet
- Death and Its CauseDocument22 pagesDeath and Its Causeअनूप ठाकुर100% (1)
- GASTRO - GastritisDocument9 pagesGASTRO - GastritisOsyd Friss BlackNo ratings yet
- Biology Notes CHPTR 12Document14 pagesBiology Notes CHPTR 12Wan HasliraNo ratings yet
- Anesthesia For Patients With Diabetes Mellitus - UpToDateDocument31 pagesAnesthesia For Patients With Diabetes Mellitus - UpToDateEduardoNo ratings yet
- Sanofi Annual Report 2014Document85 pagesSanofi Annual Report 2014MirzaNo ratings yet
- Dolo 650 MG (Paracetamol) : Uses, Side Effects, DosageDocument3 pagesDolo 650 MG (Paracetamol) : Uses, Side Effects, DosageRaluca Elena Raluca ElenaNo ratings yet
- Physiological-Changes-in-Aging - RESPIRATORY-SYSTEM (Autosaved)Document70 pagesPhysiological-Changes-in-Aging - RESPIRATORY-SYSTEM (Autosaved)Patric Aaron de VillaNo ratings yet
- 19mbm003 Aiswarya Lakshmi Thakka Ravunni Y - 12798 - Assignsubmission - File - Mip-19mbm003, Aiswarya Lakshmi Thakka Ravunniy-SignedDocument21 pages19mbm003 Aiswarya Lakshmi Thakka Ravunni Y - 12798 - Assignsubmission - File - Mip-19mbm003, Aiswarya Lakshmi Thakka Ravunniy-SignedVadivelNo ratings yet
- 1 PBDocument8 pages1 PBRobas BasathaNo ratings yet
- Philippines HIV/AIDS Registry For September 2019Document8 pagesPhilippines HIV/AIDS Registry For September 2019Michael DavidNo ratings yet
- Micro-Chem Plus TDS English GHSDocument1 pageMicro-Chem Plus TDS English GHSFrank AlvaradoNo ratings yet
- Introduction To Maternity Pediatric Nursing 6th Edition Leifer Solutions ManualDocument6 pagesIntroduction To Maternity Pediatric Nursing 6th Edition Leifer Solutions Manuallioneldatfcc12100% (28)
- Joint Syndrome. Osteoarthritis. Solodenkova K.S.Document40 pagesJoint Syndrome. Osteoarthritis. Solodenkova K.S.Abdullah KhanNo ratings yet
- TOPIC 3.A Bag TechniqueDocument38 pagesTOPIC 3.A Bag TechniqueJayrelle D. Safran100% (1)
- Disturbed Sensory PerceptionDocument3 pagesDisturbed Sensory PerceptionJashtine JingcoNo ratings yet
- 2023 Complications and Treatment Errors in Peri-Implant Hard Tissue ManagementDocument22 pages2023 Complications and Treatment Errors in Peri-Implant Hard Tissue Managementmatias cofreNo ratings yet
- Clinical Guidelines PDFDocument19 pagesClinical Guidelines PDFEmilio AcostaNo ratings yet
- What Causes CancerDocument2 pagesWhat Causes CancerSilla, KyshiaNo ratings yet