W
SKIN
ECZEMA
Eczema is a non contagious inflammatory disease fo the skin in
response to endogenous or exogenous stimuli, characterized by
erythema, edema, vesiculation, oozing, weeping and crusting.
Microscopically, characterized by intraepidermal vesiculation. It
is due to an antigen-antibody reaction.
Etiology
There are two groups of eczema — exogenous (or contact) and
endogenous (or constitutional) :
Exogenous eczemas
« Primary irritant dermatitis.
* Allergic contact dermatitis.
+ Infective dermatitis.
Endogenous eczemas
+ Atopic dermatitis.
+ Seborrhoeic dermatitis.
+ Neurodermatitis
+ Discoid
* Gravitational.
* Pompholyx.
Exogenous eczemas
Irritant contact dermatitis : Detergents, alkalis, acids,
pec abrasive dusts are common causes. Irritant contact
¢memas account for the majority of industrial cases and work
hf.
+ and is due to irritant
loss. Napkin eczema in babies is common
ammoniacal urine and feces.
: It is due to a delayed
Allergic contact eczem™ © ace with an antigen.
hypersensitivity reaction following con
Some common allergens
shes Present In
Nickel “Joweltery, Bra clips, Jean studs
pews Cement, tetera
Rubber cherleats Clothing, Shoas, Tyres
Hair dye, Clothing
Paraphenylee diamine
Perfumes, Citrus fruits
Balsam of Peru
Neomycin Topical applications
Parabens Preservatives in cosmetics
Epoxy resin Resin adhesives
Endogenous eczemas
Atopic eczema : Atopy is a genetically determined disorder
in which there is an increased liability to form IgE antibodes
and increased susceptibility to cetain diseases like asthma,
hay fever and dermatitis.
Seborrheic dermatitis : [s a constitutional diathesis
which affects ceratain areas of greatest sebacious activity.
Sometimes becoming generalised.
Pathology (eczema)
The histological changes in eczema reflects the dynamic changes
resulting from inflammation of the epidermis and dermis.
Histology of the classical eczema passes through the following
stages :
Spongiosis : Epidermal edema, separation of malpigian cells
stretching and rupture of prickles.
Rupture of vesicles.
Parakeratosis : In which horny cells retain their nuclei.
Lichenification : Thickening and increased pigmentation
of cells layers.
-_
ALIST OF COMMON REGIONAL CONTACTANTS
tose directly applied like
a cosmetics — face powder, cream, bindi, varmilion (sindhur), eyebrow
pave ume, $02, 0! (Brahmi, Lom: 1 ecto, Crest a
ee tume, Loma Cr
pert Ee ‘and Cantharadine etc.), shampoos, dyes (Inecta, Crest and Para
pe actacle frames. ‘dS, The distibution is typical in all these contactants.
ec]
csovedst poets, fumes, paints.
by the patient’
rose eee nen ee ‘almost any iritant or sensitizer may get on to the face, since it
i oa face with fingers from time to time. Nail vamish is a common
exe .
Ups: Lipstick. toothpaste, cigarette holders, pipes and balloons.
- ecart, dyed fur, collar, ing i i
Neck! scarf, dyed fur, collar, buttons, marking ink, jewellery (particulatly chrone or nickel), hat strap,
sume. , ,
pody: Clothing, buttons, marking ink (dhobi’s mark) .
agiae : DeSS armpit pads, dyes, depilatories, deodorants, astringens.
Genitals and a oe i Cortcentves (rubber, quinine and other chemicals), toilet paper,
medicaments used DY louches , antiprurtus (particularly cocaine derivatives), feminine hygiene
gprs. avlonsiplastic underwear,
puttock : Tolet paper, lavatory seat (vamish), jute and straw mattresses, toy horses.
+ Occupational - primary irritants and sensitisers. Hobbies - gardening, photography, painting etc.
onions, tomatoes, ladies fingers: drivers steering wheel, ignition key;
Wrists : Waterand its strap, bracelet and bangles.
Thighs : Clothing, things in pockets particularly matchboxes, ‘and suspenders (rubber or nickel).
Feet : Footwear, shoes (chrome dyes and rubber). The dorsum and sides of the feet are selectively
| scaces ate spared (comparison : tinea pec), Colored sacks (dyes and nyion), elastic
shoe strap
Symptems / signs
Acute eczema
Redness and swelling, usually with ill defined margins.
+ Papules, vesicles and more rarely big blisters.
+ Exudation and cracking.
+ Scaling.
Chronic eczema
* Many show all of above fe:
vesicular and exudative.
+ Thickening : Lichenification, a dry leathery thickening
with increased skin markings is secondary to rubbing
dis most often seen in atopic eczema.
atures though it is usually less
and scratching an
+ Fissures and scratch marks.
* Pigmentation.
662 extbook of practice of medicine
seborrheic eczema
sealp, ears, [c€
i
presternal an P
of axillae, umblicus:
Fissure
id eczema gq seen most often in elderly males,
those of other type of eczema
vesicular and crusted.
Disco!
common form ©)
is
This eejons are more di
The lesion:
and are usually mu
Gravitational eczema
Occurs on the lower leg an
tig insufficiency !
d is often assosiated with signs of
veno’
» Edema. ;
«Red or bluish discoloration.
OCCUPATIONAL DERMATITIS
Occupation Causative Agents and Type of Dermatitis
sw ngrcuturats and gadeners Plants, waeds, Pe rides, fertlizers and oils - mechanical injures
a and contact dermaiis.
Automobile workers is, poral, slvents, greases, paints, thinner —2cne ane demettis.
Cement lime, insecticides, fungicides, wood, pains, Kerosene ol,
© Building workers
turer!
Chemical and Phawraceuticel Different ay6
ils, disinfectants,
als, pha s, explosives, solvents,
ens eto. — contact dermatits
industries
© Coal miners Mechanical injures.
« Dentists
Engineering Industries Cutting oils, solvents, 4
© Housewives ‘and detergents, vegtanles and fruits, nickel, polishes, pare-
pherlyene diamene, reys, Kerosene ol, wooden cutlery, lowes,
adsed to foods !ke socium bisulphide
tuber gloves, and sensit ser
in salads, artifical favors, para!
ageris in laundry products.
fodine, streptomycin, chlorpromazine, s
conaine denvatives contact dermatitis
Turpentine, pains, detergents ~ contact dermatitis.
Mel, bichromate ~ contact dermatitis
Resins, hardeness, solvents, alues, cellulose, esters ete. — contact
dermatiis,
© Printers Dyes, acrylic plales and inks causing dermatitis and
Rubber workers MB.EH., T.M.T., M.B.T,, dyes, glues, oll etc. ~ con
and depiginentation
Chromate, formaldehyde, dyes, arsenic, alkel
derraitis and depigmertation,
Dermatitis and tar acne.
Formaldehyde, solvents, dyes, bleaches e
_ dyes, fuorescent whitening
iphonarnide, tinct, benzoin,
2 Nurses and Doctors
e = Painters
© Photographers
Plastic factory
tact detmatitis
e Tanney workers ies, acids etc.
e Tar workers:
«Textile workers tc. — contact dermatitis.
* Loss of hair.
* — Induration.
. Ulceration,
Pompholyx (Dyshidro
This type of eczema h,
formation and affects th
Investigations
Patch testing to
allergic contact eczema.
Prick testing : 1
atopic eczema if food
exacerbating factors,
Hemosiderin pigmentation,
tic eczema)
‘as bouts of recurrent vesicle or bulla
¢ palm, fingers and sole.
allergen : Used in suspected cases of
It is Used for few patients with stubborn
or inhalant allergens are suspected as
Culture : This is for bacterial yeast and fungal pathogens.
DISTINGUISHING FEATURES OF TRUE INFANTILE AND
SEBORRHEIC ECZMEA
Seborrheic
Infantile
« Diseases develop af 3-6 months after birth,
somatimes earlier.
« Child is irritable and weak,
Starts from cheeks and extends to forearms
and legs.
Oozing mare. Areas look clean
« Family history of atopic disorders except
in simple variety
+ lching is severe and spasmodic
+ Recurrences frequent and usually independent
of season,
‘Cradile cap’ at the time of birth, seborthoeic
dermatitis efterwerds.
Child is usually healthy and happy olhernise.
Stans from scalp, posterior auricular folds, and
involves neck and trunk, On the trunk fiat
macular erythematous or hypopigmented and
scaly rash. in some cases, it manifests as
diaper dermatitis.
Crusting more and the areas hav 2 diny
appearance.
Family history of seborthoeic disorders.
Itching, mild to moderate.
Recurrences mostly seasonal ie. summer
and monsoon; at times in winter also.
Complications
* Superinfection, with bacterias or yeasts and viruses.
Reaction to local medicaments.
Psychological affects - anxiety neuroses.
cea _Textdook of practice of m
pifferential diagnosis
seborrheic dermatitis.
. Contact dermatitis.
Impetigo:
Treatment
Explanation, reassurance and encouragement
Avoidance of contact with irritants.
Protection of affected part
Patient should be careful in their choice of soap; they shout
not be drying after bathing; rinsing skin should be patie’
dry not rubbed.
Homoeopathic medicines
i , with great burni
Arsenicum : Chronic forms of eczema, wi rning ang
itching. The skin is thickened. Chronic dry eczema (Lyco, in dy
scaly eczema.) /
Baryta carb : Ecema on the back of hands, skin rough, dry ang
chapped /
Berberis aquifolium : Scaly, pustular eruptions on the face,
: This remedy relieves the ithcing of eczema rapidly
Croton ti, ,
and permanently; small blisters.
Fluoric acid : A very valuable remedy in eczema with itching
red vesicles having a tendency to scale off.
Graphites : Moist, scabby eruptions on the scalp, sore to touch,
The skin is very sensitive to touch and suppurates easily. It is
also useful in eczema of the genital organs.
Eczema capitis and moist eczemas, when chron
Kali mur. :
and obstinate in character.
Mezereum : The best remedy when crusts form and there is
great itching, worse when warm and wrapped-up. Secretion dries
quickly producing crusts under which thick pus oozes.
Rhus tox.: Eczema with vesicular eruptions, which are numerous
with great itching. The skin is often swollen and edematous and
these vesicles have a red circumference at the base. Symptoms
worse at night, in damp weather and in winter,
Sulphur : Eczema erythematosum. Ageravation from washing
Scratching makes the part burn intensely; tendency to pustular
eruptions; eruptions of yellow crusts.
Rhus venenata : A single dose of this medicine in 30th poten
will sometimes suffice in a simple case. In case it aggravates, 7
skin 665
ae a
SI eo
Medicine should not be repeated but the results should P
watched for some time, until a higher dose becomes necessary.
° chive |
Alumina : Chapped or dry eczmea; intolerable itching in warm
bed.
Urtica urens : Eczema with burning, itching and stinging.
Mercurius cor. : Obstinate eczema including eczema capitis.
Note = Tuberculinum and Syphilinum are the most important
remedies in all skin affections.
Other remedies : Ars. iod., Bar, m., Calc., Calc. sulph., Cic.,
Dule., Hep., Jug. c., Jug., Led., Olnd., Petr., Psor., Sulph-iod.
(Beyond this regional involvement may be scen under relative
sections. Constitutinal treatment is the basic approach).
PSORIASIS
It is a chronic, non infectious skin disease characterized by well
defined, slightly, raised, dry erythematous macules with silvery
scales and typical extensor distribution. The main abnormality
in psoriasis is increased epidermal proliferation due to excessive
division of cells in the basal layer and a shorter life cycle time
The transit time of keratinocytes through the epidermis is
shortened and the epidermal turnover time falls from 28 days to
5 to 6 days.
Etiolegy
+» The exact etiology is
unknown. A genetic
predisposition is
evidenced by a
positive family history
in 25% patients and
association of HLA B&
and Al7.
THE HISTOLOGY OF PSORIASIS
Poiymorpnenuctear
leucocyte mecro-abscesses
Parshereioss
Prortasis
+ Biochemcial. — {
ee
* Immunopathological : : Ss)
Many immunological é
abnormalities have
been found but their
role is uncertain.
Ineguiar nekenng
ol epwarma:
Dlates ana tonuows
capillary oops
Upper tra Tine
Dermal : The in- anne
creased epidermal
cell proliferation of
Psoriasis is related to increased replication and meta
ers eats
olism
edicine
686 Textbook of practice of
re ups ~
Factors causing flare UPS sury or irriation of normal
“ Koebne? penomenon) | the site. This is called
«Trauma (Koel «of psoriasis .
jon!
skin induces }s!0
Koebner’s phenomenor '
«Infection : B-hae™ strep ese
» Sunlight : 10% becomes me.
Drugs ! Antimalarials, beta-t
« Emotion - Anxiety.
Pathology
Histology
. ratosis. igi
Parakerato of the stratum malpigii
Thinning of supra-paillary portion
Elongation of rete-pegs-
Edema and clubbing of papillae.
Micro abscess of ‘Munro’.
+ Dilated and tortuous capillary in
« Edema and round cell infilteration in
upper dermis.
Various variants
Plaque pattern : Most common type; individual lesions are
well demarcated; range from few mm. to several centimetres
in diameter. The lesions are red with dry, silvery white
scaling, which may be obvious only after scraping the surface,
‘The elbows, knee, lower back and scalp are most commonly
affected.
Guttate psoriasis : Usually seen in children and adolescents.
A shower of small sized (3-5 mm) erythematous papules
which are scaly initially; patient may develop the plaque
pattern later.
upper dermis.
the papillae and
Pustular psoriasis : Pustular lesions are sometimes localised
to palms and soles; in severe cases of generalised pustular
psoriasis, pustules of variable size appear all over the body.
Arthropathie psoriasis : Limb joints are commonly involved.
Distal arthritis, involving distal interphalangeal and other
small joints, is the commonest presentation.
pe rt cies psoriasis : It is a complication of psoriasis
ally occuring as a result of injudicious treatment.
Fi 5
vole psoriasis 3 Flexural areas are predominantly
. Psoriasis involving the natal cleft, submaxillary
ne
<7 ano
o&@
Skin 697
axillary folds ot scaly but req,
» Blisten
ny
eB
and n
symmetrical.
jasis : i and
mucosal psor! # It is the genital m
is which i 7 UCUS me;
glans penis which is more often involved thay TMM" esp
symptoms J signs ™Ucosa,
typical distribution is extensor type.
. Common areas affected are scalp, back of elt
+ sgnces, legs and lower part of the back, of the ae front of
runk.
t exhibitis itself as a dry, well defined mai
+ Sraque of erythema with layer upon layer or Papules and
when a psoriatic lesion is scratched with the wales
dissecting forceps, a candle greases like soa tt ofa
repeatedly produced even from non scaling lesi fe can be
called the ‘candle grease sign’ ions. This is
The complete removal of scale produces pinpoi
which is typical of psoriasis. Pinpoint bleeding
Normally characterised by absence of itching, but in topi
countries patient complain of slight or moderate praia
The lesions are slightly raised above the surface of ski
there is no induration. e of skin, but
psoriatic lesion may develop along the scratch lines in the
active phase; this is called Koebner’s phenomenon.
Nail show three type of lesions.
- Pitting.
- Separation of the distal portion of the nail from nail-bed
and wall.
- Thickening of nail
+ On scalp : thick, scaly papules discretely distributed all
over, with intervening areas of normal skin. The lesions are
ary; there is no matting of hair, never causes loss of hair and
baldness.
Investigations
' History is typical
‘ Biopsy is rarely required.
lifferential diagnosis
* Atopic dermatitis.
Impetigo.
Reiter’s syndrome.
jnstructions are vital ang
ent’s intelligence. ~
e and
t’s or par
tient shou
equent sun baths before
Iphur springs all are usefu
reassuranc
he patien
ld be maintained.
A moderate warm climate. fr
onset of winter and visits of SU
bringing down the relapse rate.
c¢ medicines
Homoeopathi
Hep., Lyco., Petrol.
Im : Graph..
Psoriasis of pa
puce, nails : Graph., Sep.
Psoriasis of pre
Psoriasis of tongue : Sep.
Other remedies : Ars. iod., Kali. ars., Lyco., Mez., Pi
yco., Mez., Petr.,
Pors., Sars., Sep.
ACNE VULGARIS
jis a common inflammatory disease of t!
geen i adolescents characterised by
ceoondarily infected, resulting in papules,
qones, nodules and scars. In the preadolesce: rt
gleosa and some comedones frequently epeen aa ners
the disease in the twenties; it gradually decreases and is am 7
seen especially in women after the age of 28, or so (post adolescent
gene). It occurs in both girls and boys; in the latter ma
somewhat severer form.
he pilosebaceous follicles
comedones which are
pustules, cysts, come.
» ina
Theories of
causation
« Increase in the | frdens|
quantity of androgens
secreted, or increased
sensitivity of the
sebaceous glands to _ | sebaceous on
Occlusion of
llosebaceous duct
-Beciovel colerisaton
of duct
Increased stu
androgens. comme
ee toi
Alteration in the com- ~_ psi ery
Position of sebaceous 4} medias mio Gee,
secretion (free fatty ‘THE PATHOGENESIS OF ACNE
acids are increased
and these are irritant
to the skin).
leading to formation of c
icine
672 Textbook of practice of me:
8.
Alteration in bacterial flora of the skin — acne bacillus pro-
piohibacterium acnes.
Acne is often familial. The inheritance pattern is probably
polygenic.
Pathology ; lidiyrot ecb ;
‘ is i ivity of sebaceous gland:
yuberty there is increase in acti : g :
eon Pow If the infundibulum of the follicles are plugged
of Skin Collection of sebum inside the follicle. These is growth of
a bacillus, which causes release of fatty acids. These fatty
se egi y ction to sebum occurs,
acids act as irritants and foregin body rea
acids act a omedones, papules etc. If pus
accumulates inside then pustules form.
Symptoms / signs
Onset and progress : Starting just after puberty the
comedones prgoress to papules and may completely involve
or progress to form pustules, and heal with resultant scars or
pits.
Sites :(Cheeks, chin, nose, forehead, chest, back, shoulder
and buttocks usually associated with an oily scalp. —
Types of acne
« | Comedones : Comedones are only on an oily skin.
White head : On the surface of skin, it appears as a slightly
elevated white dot.
Black head : Sulphur constituent of sebum soon get converted
into sulphide turning the white head into black dot, called
blackhead.
Acne papulosa : Large number of inflammatory papules.
Acne pustulosa : Papules often suppurate to from pustules,
resutling from the action of secondary invading micro-
organisms, chiefly staphylococci
Acne indurata : Characterised by firm, perifollicular nodules
of bluish rtd colour.
Acne cystica : Many of indurata eventually become
completely or partially absorbed, other transform into cysts,
acne cystica.
Acne atrophica : Where there are tiny residual atrophic pits
and Scars.
aoe ag
qreatment | Skin 673
Must be treated oa,, +f
ue sioid scarring. Early, condition be kept Under og
—— — Ntrol to
_-General : The ener, ——
“ 1
and hypothyroidism ae should be checkeg
Diet : Certain foods st ,
v “chocolate, Creams
etc.
- Cleansing : Wash thi
-, le face fr j 3
flora and removes the Seas ci with soap. This reduces
» Laser therapy can be used.
improvement,
> ANemia
fe ould be avoided like Pasteries, pj,
’ Wed foods, nuts, eggs, butter anit pa
Dermoabrasion helps in cosmetic
Homoeopathic medicines
Hydrocotyle : Great dryness and desquamation of epidermis,
|-Nux vom. : From liquor drinks,
Agaricus : With blueness and tendency to chilblains.
Ars: iodide or Sulph iodide : Severe obstinate cases.
Bellis p. : From cold drinks.
Carbo. an. : For recent cases, but if they are full of blood, give
Bell. and if they are pale, give Pulsatilla.
Carbo veg. : From gastric derangements.
Kali brom. : For eruption on face, chest and shoulders (Acne
vulgaris).
Antim sulph. 6x : (Acne with pus).
A mixture of Silicia 200 + Carbo veg. 200 for acne. .
jes 2 . crud., Aur., Calc. sili, Calc. s., Carbo.
mite, Capen. ee. Psor., Sep., Thuja, Tub. (see distribution
area also in repertory).
layer of the eipiaermis,
lives there for about two
months. In these burrows,
she lays her eggs which
develop into larvae. They
pierce the roofs of the
burrows, find shelter in the
pores of the skin, and
develop into adult mites.
The life cycle of the acarus,
from the ovum to the adult
Stage is from 13 to 21 days.
Symptoms / signs
* The lesions usually
Spares head and neck
History of exposure or
multiple cases in the
family,
Nocturnal pruritus.
Burrows; they
tebresent the path
Taversed by the
aiasite in the horny
oe of the skin. Their
ths vary from a
sasceri(5 SABO
ANIMAL PARASITES,
688 Textbook of practice of medicine
i ith
quarter of an inch to one inch. If the roof is I ate
Recdle, the mite can be demonstrated, The comune es Of
burrows are the fingers, the interdigital webs, f Ee ae
\srists, the points of elbows, the anterior axilaty 0 Manoa
the nipples, the abdomen, the buttocks, 8¢!
and the feet.
* Fine, pin-head sized, follicular papules.
. Excoriations and scratch markes.
Laboratory diagnosis
: ° : rganism)
+ Microscopic examination of specimen for org:
. @urrow ink test
Complications
+ _Impetigonization.
: “Eczematization,
* Secondary lymphadenitis.
Differential diagnosis
* Pediculosis,
. Other causes of pruritus.
Treatment
* . Personal hygiene and daily bath; separate clothes, bed linen
and towels; use of medicated scap containing 3 p.c. acid
Salicylic and 10 p.c. sulphur (Tetmosol). Hot bath and
thorough scrubbing followed by new clothes. Old clothes
should be disinfected.
° Treat all contacts - conjugal, family members, school friends
etc, whether they have symptoms or not. This is most
important to prevent ping-ponging of the disease. It must be
bered that pruritus may persist for a few weeks even
the acari have been got rid of by the specific treatment.
Half hearted, ineffective treatment of contacts and inadequate
infection of clothing are responsible for failure to cure
and eradicate scabies.
Homoecpathic medicines
Anthrok., Crot tig., Hep., Mez., Psor., Sep., Sul.
Arsenicum : Inveterate cases; eruptions on the bends of knees;
pustular eruptions; burning and itching : better from external
warmth.
Skin 689
ta : Baker’s and Grocer’s it erupti
serie ch, as cruptions on the back of
carbo Veg. ? Eruptions dry and fine; alm
worse OP the extremities; itching worse afte
symptoms, belching of wind and _passi:
mercurial ointments.
‘ost on the whole body
T undressing; dyspeptic
ng of flatus; abuse of
causticum : Abuse of mercury and sulphur; yellowish col
the face; warts on the face; involuntary discharge of uri re wh mn
coughing, sneezing or waking, sensitiveness to cold zie, “nen
Hepar sulph. : Fat, pustulous and crusty itch, also aft
mercurial ointments. sneeon
Sulphur : It is the main remedy, voluptuous tingling and itching
with burning and soreness after scratching.
Sulphuric acid : Indicated when itchiness of the skin and single
pustule appear every spring after a not perfectly cured itch. If all
the above remedies fail (in IX potency), Dr. Hering’s
recommendations be followed as laid down below :-
Begin with one dose of Mercurius 30, and give after a few days
Sulphur 30 in alternation for sometime. If improvement takes
place, stop further dosing. If there is, however, no relief, try the
following remedies :-
Carbo veg. : Every other day, if the vesicles are small and dry, or
ring and evening. But if the pustules are
give Hepar suiph 30 moi
then Sulphur and afterwards Causticum
large, give Mercurius,
night and morning in water.
Lachesis : If the pustules are large and become
repeat it whenever the pains get worse.
i is: f the pustules, take
Note. : On suppression or disappearance 0! t ;
Sulphur or Arsenicum 200 (one dose) fortnightly, until the rash
returns.
yellow and blue,
ee ““pusiled in the lymphatic vessels
and gland. The male is about 4 cm by 0.1 mm and the
female 6 cm by 0.2 mm. 1 hey copulate, the female becomes
gravid, discharging microfilariae (livin
lymphatics: these ente;
lymphatics have become o
the primary iriation and
are found in the
Stage of infection Mosqui
hosts in w
into infective larval filari
beings through bites by
enter the lymphatic
nto blood stream unless the
ccluded by inflammation due to
Secondary infection, Microfilariae
» sucked during bitings, mature
ae. They are transferred to human
infected Mosquitoes; larval filariae
system, maturing in about 3 months.
Symptoms / signs
Stage of invasion, the
symptoms are mainly
allergic taking the form
of painful swellings of
the scrotum, arms and
legs (like erythema
nodosum), urticarial
lesions, lymphadenitis,
lymphangitis and
filarial fever.
q
After the adult worms
have lodged them-
selves in lymphatic
vessels and glands, the
microfilariae are
liberated. Only at this
Stage can they be
demonstrated in the
peripheral blood. Filarial abscesses,
lymph scrotum, lymph hydrocele an
and hydrocoe!
Wuchereria ba
ZEND
ee
Epididymo-orchitis
Microttar,
=f ‘ae
in blood
us \d) Adu worm in
Yrph vessel
Lympanote
ncrott| and Brugia malayi, Life eyele
and pathogenesis of lymphatic filariasis,
be
» varicose groin glands,
d chyluria, arthritis etc,
are the usual symptoms at this stage. Inguinal and femoral
glands are hard and fibrous; when
microfilaria can be demonstrated
lymphatics are also seen. In lymph
enlarged, bulky and itchy. Surfac
which on rupture keep on disch
colored fluid
The most common infestation
elephantiasis of the legs and = scr
obstruction of the lymphati
There
pl
is tense solid ede
accompanied by repeated
eosinophilia, Elephantiasis js a very
often cripples the patient.
are often enlarged. Micro
this stage.
fil
Investigations
Eosinophilia,
Treatment
Pressure bandages and sg
elephantiasis.
urgery
The lymp!
Demonstration of microfilariae in thi
unctured with a syringe,
in the lymph. Indurated
scrotum the scrorum is
e shows lymph varices
arging continously straw-
one comes across is
otum produced by the
ic vessels and glands,
lymphangitis, and
distressing symptoms; it
hatic glands in the groin
ariae are absent from blood at
€ night blood.
complement fixation and skin tests.
help the bad case of
ii
mosqui
Homo
Arse
e reme
the fei
Elephantiasis
d skin, hardened and itching).
Hydrocele
is consists of mass treatment of all
‘an area and the eradication of
¢ prev" r
The Pid indivduals in en ane
f insecticides in the breeding places.
nfecte
toes by the usc
eopathic medicines
Mez., Staph.» Psor» Sulph-
dies given under ‘Malaria’ apply in this disease also, at
rbrile stage:
Elaeis (thickene
great thickening of epidermoid layer and
Hydrocotyle (
exfoliation of scales).
anacardium (skin sym
Myristica sebifers (inflammation 0
(epithelioma of skin).
ptoms similar to Rhus) .
{'skin, cellular tissue).
Arsenic alb.
Silicea (elephantiasis of scrotum).
Apis (serous inflammation of testes).
Aurum (chronic inflammation of testicles).
Cal. fluor. (induration of testes).
Conium (testicles hard and enlarged).
Fluoric acid (swollen scrotum).
Graphites (testicles swollen and indurated).
Rhododendron (induration and swelling of testicles after
gonorrhoea).
Spongia (swelling of spermatic cord and testicles with
pain and tenderness).
Inflammatory fever
* Aconite
+ Bell.
+ Bry.
Lymphangitis
* Apis
* Ars. iodide
* Mere. sol.
Lachesis
adenitis
- Apis
. Bell
« lodium
. Phyt
{LICHEN PLANUS
nate. 2 hronic_disorde;
«¢ an uncommon acute, subacute or chronic disorder of tp
okin and raucous: ancs characterized by purplish <
Golaccous, polyhedral, flat-topped, itchy, papules: occuring mostly
cn the flexor surfaces and in the_mouth. The name lichen jg
Sefived from the resemblance it has to the purplish lichens that
grow on trees in the hills.
ce main features of lichen planus are :
. i itic skin lesion:
oy ical pruritic skin lesions
+ Cmocosal lesions. )
ban tration 0
{ melanophages and lymphocytes in
Etiology
«It’s cause is unknown.
+ (Psychogenic stress.’)
«In tropical countries, a lichen-planus-like eruption is often
brought about by chloroquine and insect bites.
Pathology
It is characteristic and, in a typical lesion, it consists of
sis, a patchy increase in the stratum granulosum,
shortening of the inter-papillary processes, basal cell
degeneration, and a well-defined band of round-cell infiltration
in the upper corium.
Symptoms / signs
Typically, lichen planus consists of polyhedral, firm, purplish
or violaceous papules with shiny, {fat tops; very thin, firmly
attached scales may be evident on the surface.
Faint striations of grey streaks (Wickham’s stria) can be seen
on the surface of the papules through a magnifying lens
These are best demonstrated after applying oil to the lesion.
The papule is about the size of a _Split_pea_{sometimes
smaller) =
The papules may become confluent to form plaques if the
enlarge with cenira’ clearing; rin, -
papules anus annularie). Each ring hag cfs 2 forme
Leer with a reddish or purplish lichenoia Peripher emented
cengastant, being more 90 in dark-skinned peorae tian
tropical climates. ing in
Itching produces_lichen_planus_papules along the lin
ie of
seratching "Koebner’s phenomenon’ similar to one. att
a = 7 in
3 :
psoriasis. :
The (ash is bilateral and_symmetic
the front of wrists, the flexor surface
abdomen, the legs, genitalia and the
Lesions also occur in the mouth, buccal Mucosa, |,
commonly, on the lips, tongue and genitalias ~~” [°88
It is distributed
alon,
sof the forcarmens
Sek orcas, the
The disease is seldeom seen on the Scalp, the pal
ms
hands and the soles of the feet. The mucous tient?
lesions are usually a symptomatic, but sometimes valtge
little burning and irritation.
It is usually a chronic disease lasting for several months or
years.
Nails are affected only in a minority of cases.
Variations of lichen planus
Annular lichen planus : Ringed lesions with central clearing
and raised firm periphery.
Acute generalized lichen planus : The onset is sudden, the
course short, and the rash is generalised. In the early stages,
the eruption may not be typical, but characteristic lesions
soon become visible. It may merge into chronic lichen
planus.
Lichen planus verrucosus : It occurs as hyperkeratotic,
verrucous, violaceous nodules and patches on the legs. It
may occur as such, but is usually accompanied by typical
lesions on the legs, wrists, forearms, etc. Itching is severe.
Linear or herpes-zoster like lichen planus : The lincar
form, common in children, is seen on the extremities or the
face. The lesions rarely occur along the segmental
distribution of nerves; when they do, the condition may be
Confused with herpes-zoster or nervous unius lateralis.
Lichen plano-pilaris : It is usually seen as acuminate,
follicular papules with horny spines, accompanied by flat,
lichenoid lesions on the chest, back and upper arms.
Bullous and atrophic forms : These forms of lichen pl
ae rare,
anus
Textbook of practice of medicine
gations \
onst of typical lesion»): Polyhedral, firm, violaceou
(may be difficult to detect in dark skinned people) flat,
(imped papules with Wickham's stria and very thin adherent
scales.
(Di tribution on the flexors, genitalia and mouth.)
696
« Pruritus.
e«
You might also like
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Complete Repertory Notes?Document162 pagesComplete Repertory Notes?AbhishekNo ratings yet
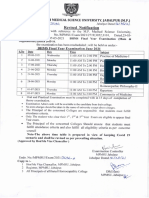
- BHMS Final Year (Main-Supply) Revised Time Table (Jun-2021)Document1 pageBHMS Final Year (Main-Supply) Revised Time Table (Jun-2021)AbhishekNo ratings yet
- Scan 7 Nov 2019Document6 pagesScan 7 Nov 2019AbhishekNo ratings yet
- Part 1 - Clinical Manual - January 2018 - Version 8.0Document260 pagesPart 1 - Clinical Manual - January 2018 - Version 8.0AbhishekNo ratings yet
- Part 4 - Standard Drug List - April 2017 - Version 8Document7 pagesPart 4 - Standard Drug List - April 2017 - Version 8AbhishekNo ratings yet
- Øekad@,U-,P-,E-@ at @1436 Hkksiky Fnukad& 25@02@2022 'KS"K FJDR Inksa Ds Fo:) de Qfuvh Gsyfk VKWFQLJ DH HKRHZDocument1 pageØekad@,U-,P-,E-@ at @1436 Hkksiky Fnukad& 25@02@2022 'KS"K FJDR Inksa Ds Fo:) de Qfuvh Gsyfk VKWFQLJ DH HKRHZAbhishekNo ratings yet
- Part 3 - Procedures - July 2015 - Version 7.1Document57 pagesPart 3 - Procedures - July 2015 - Version 7.1AbhishekNo ratings yet
- BHMS 3rd YEAR PAPER 2019Document6 pagesBHMS 3rd YEAR PAPER 2019AbhishekNo ratings yet