You might also like
- ECG Interpretations DR RPDocument109 pagesECG Interpretations DR RPArnis Putri RosyaniNo ratings yet
- How To Interpret An ECG in Seven StepsDocument5 pagesHow To Interpret An ECG in Seven StepsCM Najito100% (1)
- Cardiac ArrhythmiasDocument4 pagesCardiac Arrhythmiassmurf096No ratings yet
- Rhythm Description Schematic Diagram Egc Characteristics Sample TraceDocument6 pagesRhythm Description Schematic Diagram Egc Characteristics Sample TraceJhenne Kyle Ko Dee100% (1)
- Ekg Panum or OsceDocument69 pagesEkg Panum or OsceGladish RindraNo ratings yet
- A Simplified ECG GuideDocument4 pagesA Simplified ECG GuidekaelenNo ratings yet
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!From EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!No ratings yet
- Normal Impulse Conduction: Sinoatrial NodeDocument80 pagesNormal Impulse Conduction: Sinoatrial Nodesiusiuwidyanto100% (2)
- ArrhyDocument26 pagesArrhyMouriyan AmanNo ratings yet
- Rhythm Interpretation and Its ManagementDocument6 pagesRhythm Interpretation and Its Managementjh_ajjNo ratings yet
- ECG Rythum Study Guide PDFDocument9 pagesECG Rythum Study Guide PDFArtika MayandaNo ratings yet
- Ecg Rhythms: Normal Sinus RhythmDocument10 pagesEcg Rhythms: Normal Sinus RhythmJethJayme100% (1)
- Pharm Fall Cardiovascular Pharmacology Study Guide-106Document47 pagesPharm Fall Cardiovascular Pharmacology Study Guide-106sean liyanageNo ratings yet
- ECG Interpretations GoodDocument104 pagesECG Interpretations GoodaymenNo ratings yet
- ECG Master Class-2Document138 pagesECG Master Class-2Shohag ID Center100% (1)
- Lab Values and Vital SignsDocument4 pagesLab Values and Vital SignsWole Olaluwoye100% (1)
- ECG ReviewDocument146 pagesECG ReviewThea DinoNo ratings yet
- Ekg Full BibleDocument6 pagesEkg Full BibleTJNo ratings yet
- Internal Medicine #1Document167 pagesInternal Medicine #1Nikhil RayarakulaNo ratings yet
- Classification of MurmursDocument2 pagesClassification of MurmursNazneen SiddiquiNo ratings yet
- Ventricular Rhythms Premature Ventricular Complex (PVC)Document3 pagesVentricular Rhythms Premature Ventricular Complex (PVC)goobyyplssNo ratings yet
- Advanced Ekg Interpretation: Micelle J. Haydel, M.D. LSU New Orleans Emergency MedicineDocument88 pagesAdvanced Ekg Interpretation: Micelle J. Haydel, M.D. LSU New Orleans Emergency MedicineRoroNo ratings yet
- Chapter 1 Compatible ModeDocument93 pagesChapter 1 Compatible ModeJyha KhariNo ratings yet
- Heart Sounds: Mitral Regurgitation Congestive Heart FailureDocument6 pagesHeart Sounds: Mitral Regurgitation Congestive Heart FailurecindyNo ratings yet
- Ekg Normal Dan Acs Sudin TimurDocument59 pagesEkg Normal Dan Acs Sudin TimurArum MaharaniNo ratings yet
- Acid BaseDocument89 pagesAcid BaseEdouinaNo ratings yet
- ECG Dysrhthmias IIIDocument31 pagesECG Dysrhthmias IIIAmani Kayed100% (1)
- EKG - Assignment Without AnswersDocument10 pagesEKG - Assignment Without AnswersJon Millhollon100% (1)
- Sympathomimetic Drugs PharmacologyDocument10 pagesSympathomimetic Drugs PharmacologyHaroon JavedNo ratings yet
- Internal Medicine Topic List 2015Document3 pagesInternal Medicine Topic List 2015Krystal Mae LopezNo ratings yet
- NOAC ChartDocument2 pagesNOAC Chartsgod34No ratings yet
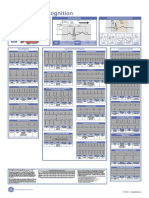
- Poster1 Arrhythmia Recognition e PDFDocument1 pagePoster1 Arrhythmia Recognition e PDFMiko RamosoNo ratings yet
- Ventricular Conduction DisturbancesDocument30 pagesVentricular Conduction DisturbancesNicholas PetrovskiNo ratings yet
- Assessment of The Chest and LungsDocument46 pagesAssessment of The Chest and LungsSumathi GopinathNo ratings yet
- Basic Ecg: in The Eyes of NURSEDocument112 pagesBasic Ecg: in The Eyes of NURSESam jr TababaNo ratings yet
- ELECTROCARDIOGRAM by Aldrin Jayson AlmadenDocument23 pagesELECTROCARDIOGRAM by Aldrin Jayson AlmadenItsMe AJNo ratings yet
- TelemetryDocument3 pagesTelemetryKelly PrattNo ratings yet
- ECG NotesDocument11 pagesECG NotesСео ЮнгааNo ratings yet
- Electrocardiography (Ecg) : Presented By: Fahad I. HussienDocument102 pagesElectrocardiography (Ecg) : Presented By: Fahad I. HussienMustafa A. DawoodNo ratings yet
- Arrhythmias: Sing Khien Tiong Gpst1Document34 pagesArrhythmias: Sing Khien Tiong Gpst1preethi preethaNo ratings yet
- Medsurg Test 4Document11 pagesMedsurg Test 4Tori RolandNo ratings yet
- Sample Acls For DummiesDocument3 pagesSample Acls For DummiesTodd Cole100% (1)
- ECG Made Easy - An Abnormal LookDocument46 pagesECG Made Easy - An Abnormal LookabdallahNo ratings yet
- P Waves: Fast & Easy Ecgs - A Self-Paced Learning ProgramDocument31 pagesP Waves: Fast & Easy Ecgs - A Self-Paced Learning Program.100% (1)
- Hypertensive CrisisDocument1 pageHypertensive Crisisapi-495201002No ratings yet
- 007 - Cardiovascular Physiology) MASTER ECGDocument8 pages007 - Cardiovascular Physiology) MASTER ECGSWATHIKA L100% (1)
- Guaranteed To Pass: Exam Tidbits in Easy To Digest, Bite Sized MorselsDocument2 pagesGuaranteed To Pass: Exam Tidbits in Easy To Digest, Bite Sized MorselsAmberNo ratings yet
- ACLS RhythmsDocument2 pagesACLS RhythmsValerie BatesNo ratings yet
- Ecg Interpretation: Presented by:-ROHINI RAI M SC Nursing Part I, C.O.N, N.B.M.C.HDocument69 pagesEcg Interpretation: Presented by:-ROHINI RAI M SC Nursing Part I, C.O.N, N.B.M.C.HRohini RaiNo ratings yet
- Joseph Brian L. Costiniano, MD, DPCPDocument70 pagesJoseph Brian L. Costiniano, MD, DPCPcarmsNo ratings yet
- My Cheat SheetDocument3 pagesMy Cheat SheetTenzin KyizomNo ratings yet
- ECG Workout Flashcards: Atrial ArrhythmiasDocument27 pagesECG Workout Flashcards: Atrial ArrhythmiasDima HabanjarNo ratings yet
- Normal Sinus RhythmDocument8 pagesNormal Sinus RhythmRosalyn YuNo ratings yet
- Soap TemplateDocument3 pagesSoap TemplaterohitNo ratings yet
- Cs-Cardiac-023-Essential Cardiac LabsDocument2 pagesCs-Cardiac-023-Essential Cardiac LabsColeen YraolaNo ratings yet
- Cardiac Study GuideDocument9 pagesCardiac Study GuideJane DiazNo ratings yet
- IV PDFDocument63 pagesIV PDFelbagouryNo ratings yet
- Cardiac II Study GuideDocument6 pagesCardiac II Study GuiderunnermnNo ratings yet
- Vital Signs LectureDocument67 pagesVital Signs LectureJayrelle D. SafranNo ratings yet
- Phlebolymphology: Vol 28 - No. 1 - 2021 - P1-36 No. 103Document39 pagesPhlebolymphology: Vol 28 - No. 1 - 2021 - P1-36 No. 103Jing CruzNo ratings yet
- Transport in Animals BookletDocument32 pagesTransport in Animals Bookletsreetyy jNo ratings yet
- Lesson 4 - The Circulatory SystemDocument19 pagesLesson 4 - The Circulatory SystemAimee GraceNo ratings yet
- R Series Product ManualDocument186 pagesR Series Product ManualppdeepakNo ratings yet
- Cardiomyopathy SeminarDocument17 pagesCardiomyopathy SeminarJyoti SinghNo ratings yet
- PAVSDMAPCAsDocument3 pagesPAVSDMAPCAsRajesh SharmaNo ratings yet
- Sony Hilal Wicaksono, MD Universitas Indonesia HospitalDocument14 pagesSony Hilal Wicaksono, MD Universitas Indonesia HospitalSonyHilalWicaksonoNo ratings yet
- Penyakit-Penyakit Jantung Kongenital.: M.S.GanesanDocument63 pagesPenyakit-Penyakit Jantung Kongenital.: M.S.GanesanSyukri SamsudinNo ratings yet
- Principle Management of Acute Coronary Syndrome: Nahar Taufiq Bagian Kardiologi Dan Kedokteran Vaskuler FK UGM YogyakartaDocument57 pagesPrinciple Management of Acute Coronary Syndrome: Nahar Taufiq Bagian Kardiologi Dan Kedokteran Vaskuler FK UGM YogyakartaIntan Farida YasminNo ratings yet
- PT EducationDocument4 pagesPT Educationapi-248017509No ratings yet
- Holter Contec TLC9803 User Manual - EnglishDocument53 pagesHolter Contec TLC9803 User Manual - EnglishEdward MoralesNo ratings yet
- Peds Shelf NotesDocument74 pagesPeds Shelf NotesRandy BornmannNo ratings yet
- CLINICAL PHARMA QuestionsDocument13 pagesCLINICAL PHARMA QuestionsAminatNo ratings yet
- 01 STR 29 1 251Document6 pages01 STR 29 1 251RAFAEL BRITONo ratings yet
- Effects of Vasopressors On Cerebral Circulation.6Document11 pagesEffects of Vasopressors On Cerebral Circulation.6diego morenoNo ratings yet
- Reading ExercisesDocument20 pagesReading Exercisesmuhammad dzikra azidanNo ratings yet
- Cyanotic Congenital Heart DiseasesDocument25 pagesCyanotic Congenital Heart DiseasesAlvin OmondiNo ratings yet
- Pathology of HEART - 1Document175 pagesPathology of HEART - 1Abdukadir AzamNo ratings yet
- AmyloidosisDocument15 pagesAmyloidosisNicoletta OrphanouNo ratings yet
- Cardiology - Pericardial Disease PDFDocument1 pageCardiology - Pericardial Disease PDFPshtiwan MahmoodNo ratings yet
- HypertensionDocument5 pagesHypertensionCia Yee YeohNo ratings yet
- CardiacDocument10 pagesCardiacMarcus Reynolds100% (1)
- Stroke AHA GuidelinesDocument104 pagesStroke AHA GuidelinesCristina ZeamaNo ratings yet
- Research ProposalDocument9 pagesResearch ProposalAbiola IbrahimNo ratings yet
- 9 ECG Strips On The NCLEXDocument1 page9 ECG Strips On The NCLEXSibel ErtuğrulNo ratings yet
- Circulation Blood Components Worksheet 2021Document4 pagesCirculation Blood Components Worksheet 2021api-523306558No ratings yet
- Heart FailureDocument108 pagesHeart FailureDeasy Rizka Rahmawati100% (1)
- Fluid Management in Neurology & Neurocritical Care: DR Nagesh JadavDocument12 pagesFluid Management in Neurology & Neurocritical Care: DR Nagesh JadavNagesh JadavNo ratings yet
- 1 Acute Inferior Wall MI With First Degree BlockDocument53 pages1 Acute Inferior Wall MI With First Degree BlockKarthik KannappanNo ratings yet