Professional Documents
Culture Documents
Review Article May-2023
Uploaded by
Vishw PatelOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Review Article May-2023
Uploaded by
Vishw PatelCopyright:
Available Formats
REVIEW ARTICLE
CORONAVIRUS DISEASE 2019 (COVID-19): PUBLIC HEALTH EMERGENCY
Babita Sarangia*, Jyotirmaya Sahooa, Utpal Janab and Guru P. Mohantac
(Received 16 May 2022) (Accepted 06 March 2023)
ABSTRACT
An outbreak of a respiratory sickness started in Wuhan, China in December 2019 and the causative
agent was found be a novel betacoronovirus of the same subgenus as SARSCoV and named se-
vere acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Coronavirus disease 2019 (COVID-19)
quickly spread around the world, with clinical signs ranging from mild respiratory symptoms to severe
pneumonia and a fatality rate estimated around 2%. Lower respiratory tract infections can occur in im-
munocompromised subjects and the elderly persons. Respiratory droplets are the causative agent for
the person-to-person spread of the disease resembling the spread of influenza. Individual to individual
spread turned into the primary mode of transmission. The transmission of the disease might be more
likely in the earlier stage of infection as the viral RNA levels appear to be higher. Accurate diagnosis in
the early stages of the epidemic helps control the spread of the disease.
Keywords: Betacoronovirus, Coronavirus disease around 14.8 % and it is 0.2 % in ages between 10 to 39.
2019 (COVID-19), Severe Acute Respiratory Syndrome Individual to individual transmission is happening both in
Coronavirus 2 (SARS-CoV-2), Mode of Transmission, the community and healthcare settings. The WHO has
Preventive Measures recently declared the COVID-19 epidemic a public health
emergency of universal concern2.
INTRODUCTION
At present, cases of COVID-19 have been found in
As per the World Health Organization (WHO), viral numerous nations around the globe. As per the report, up to
diseases proceed to develop and represent a serious the 1st of April 2020, the number of affirmed cases in China
issue to general wellbeing. The severe acute respiratory reached 81,590 of which 3,319 were dead, and 76,238
syndrome coronavirus (SARS-CoV) and H1N1 influenza were cured. The number of confirmed cases in the world
have been considered viral epidemics over the most reached 879,675 of which 43,944 were dead, and 183,665
recent twenty years. In 2012, the Middle East respiratory were cured3. On the 31st of January, 2020, the WHO
syndrome coronavirus (MERS-CoV) was first detected announced that COVID-19 was recorded as the Public
in Saudi Arabia1. In December 2019, an outbreak of Health Emergency of International Concern (PHEIC),
respiratory sickness started in Wuhan, China, and a novel implying that it might pose risks to different nations and
beta coronavirus was identified as the causative agent. requires a coordinated international response4. Later,
In January 2020, it was named severe acute respiratory 20,000 cases were confirmed and almost 1000 deaths
syndrome coronavirus 2 (SARS-CoV-2). Coronavirus have been reported in the European Region by the morning
disease 2019 (COVID-19) has quickly spread worldwide of 12 March 2020. This made WHO’s Director-General,
with clinical signs of mild respiratory symptoms to Dr. Tedros Adhanom Ghebreyesus announce COVID-19,
severe pneumonia. The fatality rate was estimated at as a pandemic5. Globally, as of 1st July 2022, there have
around 2% and increased gradually with the age. The been 545,226,550 confirmed cases including 6,334,728
death percentage in old age people above 80 years is deaths reported to WHO6.
a
Department of Pharmacy, ARKA Jain University, Gamaharia, Seraikela Kharsawan - 832 108, Jharkhand, India
b
Department of Pharmaceutics, Shiva Institute of Pharmacy, Chandpur, Bilaspur - 174 004, Himachal Pradesh, India
c
Department of Pharmacy, Annamalai University, Annamalai Nagar, Chidambaram- 608 002, Tamil Nadu, India
*For Correspondence: E-mail: aubabita2014@gmail.com
https://doi.org/10.53879/id.60.05.13515
INDIAN DRUGS 60 (05) MAY 2023 7
The most up-to-date source for the epidemiology of long, with a G+C content of 38%, and enclosed by a 5′-
this emerging pandemic can be obtained from official cap and 3′-poly(A) tail16,17. An envelope containing viral
sources such as the WHO Novel Coronavirus (COVID-19) nucleocapsid covers the virus. The positive sense RNA
Situation Board and the Johns Hopkins Center for Systems is attributed to the helical symmetry in the arrangement
Science and Engineering site for Coronavirus Global of the nucleocapsid16. The electron micrographs of
Cases COVID-19 as depicted in Table I which uses SARS-CoV-2 revealed a diverging spherical outline
openly public sources to track the spread of the epidemic. with some degree of pleomorphism. The diameters of
COVID-19 is a serious disease of international concern6,7. virion are varying from 60 to 140 nm. The solar structure
of CoV is due to the presence of distinct spikes of 9
ORIGIN AND CLASSIFICATION to 12 nm18. The CoV genome is arranged linearly as
5′- leader-UTR-replicate-structural genes (S-E-M-N)-3′
CoVs are derived from the Latin word Coronam, which UTR-poly(A)19. It also contains accessory genes, such
means crown. It is a positive-stranded RNA virus. Virus as 3a/b, 4a/b, and the hemagglutinin-esterase gene
appears like a crown under the electron microscope and (HE)16. SARS-CoV-2 is similar in genomics but lacks
the spike glycoprotein on the envelope is responsible for HE which is the characteristic of some beta CoVs17. The
the crown shape of the virus. CoV belongs to the subfamily positive-sense genome of CoVs serves as the mRNA.
Orthocoronavirinae of the family Coronaviridae and order The polyprotein gene 1a/1ab (pp1a/1ab) formation may
Nidovirales. Alpha, beta, delta, and gamma CoVs are occur by translation through mRNA20. The nonstructural
the four genera of the subfamily. Beta CoVs are again proteins (nsps), encoded by the polyprotein gene form
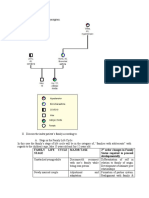
divided into five sub-genera or lineages (Fig.1)8,9. Alpha a replication-transcription complex (RTC) in double-
and beta CoVs are the two predictable gene sources for membrane vesicles (DMVs)21. Subsequently, a nested
rodents and bats. Whereas delta and gamma CoVs are the set of subgenomic RNAs (sgRNAs) is synthesized from
probable gene sources for avian species. Seven human RTC by a discontinuous transcription process22. There
CoVs (HCoVs) have been identified so far. Some HCoVs are four important structural proteins such as spike (S),
were detected in the mid-1960s and the rest in the new membrane (M), envelope (E), and nucleocapsid (N)
millennium. 2% of the population are healthy carriers of which are encoded by CoVs (Fig. 2). The S protein is
a CoV. Acute respiratory infections occur in 5% to 10% of large and functional. The arrangement of the trimer on
the population9. HCoVs such as HCoV-229E, HCV-NL63, the virion surface gives a crown-like appearance. It is
and beta CoVs of the A lineage like HCoV-OC43, and also considered a class I viral transmembrane protein.
HCoV-HKU1 are the source of common cold and self- Interaction of this protein with the host cell receptor enables
limiting upper respiratory infections in immune-competent the infectious virion particles to enter the cell. The M protein
individuals. However, Immunocompromised and elderly is the most abundant viral protein. It gives a definite shape
persons suffer from lower respiratory tract infections. to the viral envelope. The E protein is the most enigmatic
Other beta HCoVs of the B and C lineage such as SARS- and smallest. The N protein is multipurpose. It plays a
CoV, SARS-CoV-2, and MERS-CoV spread epidemics role in complex formation with the viral genome. It also
which include various respiratory and extra-respiratory enhances the transcription efficiency by facilitating the M
infections. The mortality rates are 10% and 35% in cases protein interaction during virion assembly. SARS-CoV-2
of SARS-CoV and MERS-CoV, respectively. The survivors genome also contains 15 nsps, nsp1 to nsp10 and nsp12
with SARS-CoV-2 having clinically significant COVID-19 to nsp16, and 8 accessory proteins (3a, 3b, p6, 7a, 7b,
disease were not observed with long-term complications. 8b, 9b, and ORF14). All these proteins play a specific
The mortality rate was between 1% to 2% worldwide1. role in viral replication9,12,15,23-26.
COVID-19 shows clinical symptoms such as fever,
nonproductive cough, fatigue, dyspnea, myalgia, normal Mutation in coronavirus
or diminished leukocyte counts, and radiographic evidence
of pneumonia10,11. Adult males are more preferentially Coronavirus (Fig. 2) just like other viruses holds a
infected with SARS-CoV-2 than children12,13. By some simple structure and has long RNA polymerase tightly
estimates, it has a higher reproductive number than packed into the core surrounded by a protective protein
SARS14, and more people have been reported to have layer known as capsid or nucleocapsid. There is protein
been infected or died from it than SARS15. structure projecting out of envelope are known as spikes
or peplomers. The spikes help the virus adhere to the host
Genomics and gene sequencing cells and get into the host. While multiplying or replication
CoV is an unsegmented, single-stranded, positive there can be slight changes during the replication or
sense RNA genome of around 30 kb. It is 29,891 bp reading codons due to alterations or missing codons,
8 INDIAN DRUGS 60 (05) MAY 2023
Table I: Name of the official sources for COVID-19
Sr. No. Name of official source Weblink References
1 WHO Novel Coronavirus (COVID-19) Situation https://covid19.who.int 6
Board
2 The Johns Hopkins Center for Systems Science https://coronavirus.jhu.edu › map 7
and Engineering site for Coronavirus Global Cases
COVID-19
Table II: Vaccines offered in India
Sr. No. Brand name Mfg. by Vaccine type Age range Efficacy (Highest) References
1 Covishield Astrazeneca Non-Replicating 18+ 91% 109
(Oxford) viral vector
2 Covaxin Bharat Biotech Inactivated 14< 77.8% (In adults 110
>60) 93% overall
3 Moderna NIAID RNA 18+ 90% 111
4 Sputnik V Gamaleya Non-Replicating 12< 91.6% 112
Research Institute Viral vector
5 Johnson & Janssen Non-Replicating 18+ 82% 113
Johnson Pharmaceuticals Viral vector
6 Novavax Novavax Protein Subunit 18+ 90.4% 114
7 ZyCov D Cadila Healthcare DNA based 12-18 yrs 90% or higher 115
Ltd. vaccine
and deletion of amino sugars leading to the formation COVID variants
of an altered protein structure. There can be misreading The variant is slightly different from the same entity.
of amino groups during the transcription or translation In the case of the SARS-CoV 2 virus, it is a mutation
process. As the virus replication and multiplication is a in viruses that they adapt to survive in the changing
repetitive process, the chances of variation or mutation environment; every time a virus is transferred from one
also increase. This mistake leads to changed information, person to another, there is a change in the strains. Few
making slightly changed viruses with variations known variants are as follows29:
as variants. Mutation does not change the mechanism
much but may alter transmissibility adherence to a host 1. α Variants (Alpha variants) from the UK, aka B.1.1.7.
that may or may not be more lethal than the previous 2. β Variants (Beta variants) from South Africa aka
one. Even though the mutation may appear in the entire B.1.351. Found in parts of Nigeria. It is more easily
genome of the virus’s RNA when the subset is observed transmissible but less than the original variants
a small potion can be easily noticed in the spike proteins. 3. γ Variants (Gamma variants) from Brazil aka P.1.
The spike proteins act as an antigen for the preparation These are first detected in Brazilian people traveling
of vaccination and thus play a crucial role in the study of to Japan in Jan 2021. These are observed to be more
viruses and vaccine preparations. Virus keeps multiplying contagious than their preceding variants.
themselves inside the human host but they are not
4. Δ Variants: From India aka B.1.617.2. It is about
competent enough to carry out the multiplication so they
50% more contagious/ transmissible and more lethal
use the host cells. They depend on host cell metabolism,
variants than the actual virus.
proteins introduce their RNA or viral DNA to replicate
and form proteins into a cell. Any change in the protein 5. Ω(Omicron): From South Africa aka B.1.1.529 was
structure will need different vaccine preparations, studies, reported to WHO on November 2021 to be less lethal
and measures27, 28. than its previous variants.
INDIAN DRUGS 60 (05) MAY 2023 9
MHV-A
Γ-CoVs
IBV
α-CoVs SW1
HCoV-229E
HCoV-NL63
TGEV δ-CoVs
Β-CoVs HKU11
Bat-SL ZC45
Bat-SL ZX 21 KKU17
2019-nCoV
Family: Coronaviridea SARS-CoV
Order: Nidovirales Subfamily :Orthocoronavirina MERS-CoV
HCoV-OC43
: The phylogenetic tree of Coronavirus (representative CoVs, with the new HKU-1
MHV-A59
avirus 2019‐nCoV highlighted in red)8,9
Γ-CoVs
IBV
SW1
δ-CoVs
HKU11
KKU17
Fig. 1: The phylogenetic tree of Coronavirus (representative CoVs, with the new coronavirus 2019-nCoV)8,9
Fig: 1. The phylogenetic tree of Corona virus (representative CoVs, with the new coronavirus
2019‐nCoV highlighted in red)8,9
Fig. 2: Structure of Coronavirus9,12,15,23-26
Fig. 2: Structure of Coronavirus9,12,15,23-26
10 INDIAN DRUGS 60 (05) MAY 2023
High
Medium
Low
Fig. 3: Predicted infection from COVID-19 in INDIA. Total infections (Asymptomatic+
Hospital+ Symptomatic)106
Fig. 3: Predicted infection from COVID-19 in INDIA. Total infections (asymptomatic+ hospital+ symptomatic)106
Fig. 3: Predicted infection from COVID-19 in INDIA. Total infections (Asymptoma
Hospital+ Symptomatic)106
High
Medium
Low
Fig. 4: Predicted hospitalizations from COVID-19 in INDIA (hospitalized cases)106
Fig. 4: Predicted Hospitalizations from COVID-19 in INDIA (Hospitalized cases)106
INDIAN DRUGS 60 (05) MAY 2023 11
CLINICAL MANIFESTATIONS the air. Hence airborne transmission is different from
droplet transmission. As the mechanism of transmission
Much like the manifestations of SARS-CoV and
is uncertain, airborne precautions are recommended
MERS-CoV infections, patients with positive COVID-19
routinely in some countries. Infected droplets can spread
show clinical symptoms such as fever, nonproductive
1–2 m and deposit on surfaces. In favorable atmospheric
cough, fatigue, dyspnea, myalgia, normal or diminished
conditions, the virus can remain viable on surfaces for days.
leukocyte counts, and radiographic evidence of
However, common disinfectants like sodium hypochlorite,
pneumonia12,14,30,31. Less common symptoms include
hydrogen per‐ oxide, etc. can destroy the virus in less
headache, dizziness, abdominal pain, diarrhea, nausea,
than a minute43. The virus is also present in the stool.
and vomiting12,30. Pregnant and non-pregnant women have
Water contamination with subsequent transmission of
similar characteristics32. Common laboratory abnormalities
the infection through aerosolization/feco oral route is also
found in COVID-19 patients are lymphopenia 25,26,33
assumed44. Transplacental transmission from pregnant
prolonged prothrombin time, and elevated lactate
women to their fetus is not clear till now but the post-
dehydrogenase30. ICU-admitted patients had more
natal transmission is described45. The incubation period
laboratory abnormalities12,30. Some patients had elevated
varies from 2 to 14 d [median 5 d]. The virus enters the
aspartate aminotransferase, creatine kinase, creatinine,
respiratory mucosa via angiotensin receptor 2 (ACE)46. It
and C-reactive protein12,33,34. Most patients showed normal
mainly affects the respiratory system of our body such as
serum procalcitonin levels12, 30,33.
the nasopharyngeal tract and lungs because the ACE2
receptor is highly present in those areas to which spikes
PATHOGENESIS
of SARS-CoV-2 bound. The life cycle of the virus with the
Even though the pathogenesis of COVID-19 is host consists of 5 steps; attachments(A), penetration(P),
ineffectively comprehended, the similar mechanisms of biosynthesis(B), mutation(M), and release(R). Once
SARS-CoV and MERS-CoV still can give us a great deal of viruses bind to host receptor(A), they enter into host cells
data on the pathogenesis of SARS-CoV-2 contamination through endocytosis or membrane fusion(P). Viral content
to encourage our recognition of COVID-1935, although is released inside the host cells and the viral RNA enters
the analysis of the risk associated with the transmission the nucleus for replication. The viral mRNA converts
rate is incomplete. Epidemiologic investigation in Wuhan itself into viral proteins through translation. The new viral
towards the start of the outbreak recognized an underlying proteins are made and get mutated(M) inside the host
relationship with a seafood market that sold live animals. cell, replicate, and released(R) outside for the new host47.
Subsequently, the market was closed for disinfection since
most patients had worked or visited36. The progression of TRANSMISSION
COVID-19 was due to the primary mode of transmission
The transmission of the disease is faster at the initial
which is attributed to individual-to-individual spread. It is
stage due to higher viral RNA levels soon after the onset
estimated that the respiratory droplets are the causative
of symptoms in comparison to the later stage of infection48.
agent for the person-to-person spread of SARS-CoV-2
Additional data are yet to produce for confirmation of this
resembling the spread of influenza. The virus gets
hypothesis. The transmission rate might be influenced by
discharged in the respiratory secretions because of droplet
infection control interventions and locations in the case of
transmission. A person can be infected when he or she
an individual with symptomatic infection. The secondary
comes into direct contact with the mucous membrane of
transmission rate is documented to be from 1 to 5 percent
the infected person while talking, sneezing, and coughing.
among tens of thousands of close contacts of confirmed
When a person touches his or her eyes, nose, or mouth
patients in China as indicated by a joint WHO-China
after touching the infected surface can cause infection.
report49. The symptomatic secondary attack rate was
Droplets generally do not linger in the air and travel not
found to be 0.45 percent in the U.S.50. Transmission of
exceeding two meters (about six feet)37. The size of the SARS-CoV-2 has also been reported from asymptomatic
droplets also determines the severity of the respiratory individuals or individuals within the incubation period but
infection. Respiratory droplets are > 5-10 µm in diameter the degree to which it occurs stays obscure51,52,53,54,33. A
whereas droplet nuclei are ≤ 5 µm in diameter38. As per few serological tests are under development. Serologic
the literature the mode of primary transmission was screening may provide information on the epidemiologic
through respiratory droplets and contact routes39,40,41,42,12,34. analysis and asymptomatic infection55. RNA sample has
Droplet transmission refers to the presence of microbes been detected in blood and stool specimens in the case
within droplet nuclei. Droplets travel over distances of SARS-CoV-2 infection56,57. In some cases, the live virus
greater than 1m and remain for a longer period in has been cultured from stool58. At room temperature, the
12 INDIAN DRUGS 60 (05) MAY 2023
virus is stable in faeces and urine for at least 1-2 days. In inflammatory response, hepatic tissue injury is also seen in
stool of diarrhea patients who have higher pH than normal patients with COVID-19 due to compensatory proliferation
stool, the virus is stable for up to 4 days. Further infection of hepatocytes and upregulation of ACE2 expression61.
can be prevented by the use of disinfectants and fixatives. Epidemiologic factors were used for the confirmation of
The minimal reduction in virus concentration is observed COVID-19. Within 14 days of symptom onset, the person
after 21 days at 4°C and -80 °C. For quick reduction in who was in close contact with a laboratory-confirmed
virus concentration, it should be heated at 56 °C at around COVID-19 patient or has a history of travel from affected
10000 units per 15 mins. SARS-CoV-2 is more stable geographic areas like China, Italy, Iran, Japan, South
than HCoVs as one log reduction in virus concentration Korea, etc. are included under epidemiologic factors1.
was observed at stable room temperature59. The spread
of infection was not due to fecal or oral transmission as The WHO recommends collecting specimens from
reported jointly by WHO-China49. both the lower respiratory tract such as expectorated
sputum, endotracheal aspirate, or bronchoalveolar
DIAGNOSIS lavage (BAL) and the upper respiratory tract (nasal- and
oropharyngeal samples). Mechanically ventilated patients
COVID-19 is diagnosed by auxiliary examinations were subjected to the collection of BAL samples as
such as nucleic acid detection, immune identification lower respiratory tract samples seem to remain positive
technology Point-of-care Testing (POCT) of IgM/IgG, for a longer period. Collected samples were stored at a
enzyme-linked immunosorbent assay (ELISA), CT scan, temperature of 4ᵒ C. Reverse polymerase chain reaction
and blood culture. Clinical manifestations of the infection (RT-PCR) technology is used for the amplification of the
are based on epidemiological history. However, the genetic materials extracted from the collected samples.
patients are showing atypical clinical symptoms such Subsequently, a double-stranded DNA molecule from
as respiratory symptoms, cough, fever, dyspnea, viral an RNA mold is developed through this process. The
pneumonia, etc. Hence, auxiliary examinations are genetic code particularly for CoV is conserved after
necessary along with the epidemiological history for sufficient development of genetic material. The probes
diagnosis4. The availability of testing will vary based on used are based on the initial gene sequence released
which country a person lives in and the increasing number by the Shanghai Public Health Clinical Center & School
of cases on daily basis also affects the availability of the of Public Health, Fudan University, Shanghai, China
testing. A normal or decreased total white blood cell count on Virological.org. It was subsequently followed by
can be observed in the early stage. Total lymphocyte confirmatory evaluation by additional labs. In case of a
count also decreases at the initial stage. positive result, the test is repeated for verification. Viral
clearance is required before release from observation.
The ARDS (Acute Respiratory Stress Syndrome) in It is evaluated by repeating the laboratory tests in case
COVID-19 is due to the occurrence of cytokine storms of positive COVID-19 diagnosed patients1. .
that results in exaggerated immune response, immune
regulatory network imbalance, and, finally, multiple-organ Clinically proven specific antiviral agents are not
failure60. It is reported that the liver enzymes, LDH, muscle available for SARS-CoV-2 infection62,63. The important
enzymes, and C-reactive protein level are increased, supportive treatment like the use of broad-spectrum
whereas lymphopenia appears to be a negative prognostic antibiotics to cover secondary bacterial infection, oxygen
factor. Patients in critical condition show increased D-dimer therapy, and conservation fluid management is coming
value but the procalcitonin level is normal. Decreased under the COVID-19 management strategy64, whereas
blood lymphocytes count and multiorgan imbalance such hemodynamic support is essential for managing septic
as high amylase and coagulation disorders were also found shock. Several potential therapeutic agents have been
in critical conditions. Some epidemiologic and clinical recommended to reuse the existing antiviral agents
information is required to determine who should have or develop effective interventions against this novel
testing performed. Certain criteria are fixed in the U.S. to coronavirus based on the research on molecular
put the persons under investigation (PUI). Patients with mechanisms of coronavirus infection65 and the genomic
positive COVID-19 have developed symptoms of acute organization of SARS-CoV-266.
respiratory illness such as cough, and difficulty breathing
with fever as reported by the U.S. CDC. PUI are put in place TREATMENT
of infection control and prevention measures immediately
after a recommendation and tested for other sources A novel nucleotide analog, remdesivir show strong
of respiratory infection. In addition to the exaggerated activity against SARS-CoV-2 under in vitro condition.
INDIAN DRUGS 60 (05) MAY 2023 13
Randomized trials are under process to evaluate the the immunodominant region88. Hence, knowledge and
efficacy of remdesivir which is a potential target for understanding of S protein will help to develop the potential
moderate or severe COVID-1967. Remdesivir also shows vaccine candidates based on the whole S protein, S protein
strong activity in both in vitro and in vivo conditions subunits, or specific potential epitopes of S protein against
against related coronaviruses including SARS and MERS- SARS-CoV-2. Scientists from all over the world are trying
CoV68,69. Remdesivir is used compassionately in the case hard to develop working vaccines with robust protective
of one of the first patients with COVID-19 in the U. S. immunity against COVID-19. Vaccine candidates, like
which is described through an investigational new drug mRNA-1273 SARS-CoV-2 vaccine, INO-4800 DNA
application case report70. Any clinical effect of remdesivir coronavirus vaccine, and adenovirus type 5 vector vaccine
against COVID-19 remains unknown. Both chloroquine candidate (Ad5- nCoV), are a few examples under phase
and hydroxychloroquine inhibit SARS-CoV-2 in vitro, I clinical trials, while self-amplifying RNA vaccine, oral
although hydroxychloroquine is reported to be a more recombinant COVID-19 vaccine, BNT162, plant-based
potent antiviral agent71. Several clinical trials are under COVID-19 vaccine, and Ii-Key peptide COVID-19 vaccine
process in China to evaluate the efficacy of chloroquine are under preclinical trials89. Similarly, the WHO, on its
and hydroxychloroquine against COVID-1972. Chloroquine official website, has mentioned a detailed list of COVID-19
shows strong antiviral impacts on SARS-CoV infection vaccine agents that are under consideration. Vaccines
of primate cells. The inhibitory effects on the cells are that are under different phases of trials are live attenuated
examined before or after exposure of the drug to a virus virus vaccines, formaldehyde alum inactivated vaccine,
that was therapeutically advantageous. It also indicates adenovirus type 5 vector vaccine, LNP-encapsulated
the prophylactic use of infected persons. Chloroquine mRNA vaccine, DNA plasmid vaccine, and S protein,
interferes with terminal glycosylation of the ACE2 receptor. S-trimer, and Ii-Key peptide as a subunit protein vaccine,
Additionally, it elevates endosomal pH73. The combined etc90. Effective vaccines and viral shedding are essential
protease inhibitors lopinavir and ritonavir have primarily to reduce the severity of the disease which will help to
been used for HIV infection. The combination also shows control coronavirus outbreaks. In addition to recombinant
the in vitro activity against the SARS-CoV and in vivo DNA, and protein vaccines other vaccination strategies
activity against MERS-CoV respectively74,75. Many case such as live-attenuated virus, viral vectors, inactivated
studies depicting the use of this combination against virus, and subunit vaccines are tested against SARS-CoV
COVID-19 are available76,77,78 but its efficacy is unclear. 291. The very first experimental coronavirus vaccine was
Enormous randomized trials are being conducted for the injected into volunteers in the US on 16th March 2020. The
evaluation. Another IL-6 inhibitor, tocilizumab, is used initial trial included 45 people aged 18 to 55 and doses of
in severe conditions as reported in the guidelines from mRNA-1273 into the arms of healthy participants at Kaiser
China’s National Health Commission. Still, the drug is Permanente Washington Research Institute (KPWHRI).
under clinical trial for evaluation79. It was considered the first-stage study of a potential
COVID-19 immunization. The study included the tech
Several attempts are being made to design and company operations manager Jennifer Haller. He was
develop vaccines for CoV infection, mostly by targeting the first participant in this study. The biotech company
the spike glycoprotein. We are dependent solely on Moderna prepared an investigational vaccine that is free
implementing effective infection control measures to of any part of the actual coronavirus and cannot cause
lessen the risk of possible nosocomial transmission due infection. It rather incorporates a short segment of lab-
to the lack of effective antiviral therapy and vaccines80. grown messenger RNA and the various doses are being
The majority of the treatment options and strategies tested to check the safety, immune response, and any
that are being evaluated for COVID-19 have been side effects after collecting the blood samples. According
taken from previous experiences in treating SARS-CoV, to Anthony Fauci of the U.S. National Institute of Health,
MERS-CoV, and other emerging viral diseases. Several a vaccine will not be available for widespread use for
therapeutic and preventive strategies, including vaccines, another 12 to 18 months even if all goes well92.
immunotherapeutics, and antiviral drugs, have been
exploited against the previous SARS-CoV and MERS- The effectiveness of a vaccine can be evaluated
CoV outbreaks81-86. The S protein plays a significant role by giving deliberately it to the people who are infected
in the induction of protective immunity against SARS- with the bug in question. Vaccines for the flu, common
CoV87. The development of an effective vaccine depends cold, and other respiratory illness have been developed
upon the identification of the immunodominant region. through these challenging studies. The signs of illness
The C-terminal domain of the S1 subunit is identified as after infection were observed by tracking the record of the
14 INDIAN DRUGS 60 (05) MAY 2023
participants. A study conducted by hVIVO – a subsidiary Ø Wash your hands frequently, especially after contact
of pharmaceutical-services company Open Orphan PLC with infected people or their environment.
in London, has attracted more than 20,000 volunteers in Ø Avoid unprotected contact with farm or wild animals.
exchange for a fee of £3,500 ($4,480) which provided
detailed insights into the course of COVID-19 infection Ø People with symptoms of acute airway infection should
with potentially positive health implications. Such keep their distance, cover coughs or sneezes with
investigation played important role in the development disposable tissues or clothes and wash their hands.
of the vaccines for the treatment of coronavirus infection. Ø Application of strict hygiene measures for the
These trials don’t replace the larger field studies, but prevention and control of infections particularly in
they help give direction on whether a vaccine is worth emergency medicine departments
pursuing93. Ø Individuals that are immunocompromised should
avoid public gatherings.
CONTROL AND PREVENTION
The basic reproductive number (R0) is an indication of
PRACTICE POINTS FROM AN INDIAN
an increase or decrease in the endemic. The R0 value has PERSPECTIVE
been estimated with varying results and interpretations. A total of 1,397 COVID-19 cases including 49
An average number of infections resulting from one Foreign Nationals had been reported from 27 states/
infected individual in a fully susceptible population can union territories across India as on 31 March 2020 at
be measured by the R0 value94. Studies from previous 08.30 PM according to the Ministry of Health & Family
outbreaks were found to be 2.7 for SARS and 2.4 for Welfare102. All states had issued appropriate instructions
2009 pandemic H1N1 influenza95,96. The epidemic will for all children below 10 years of age and all citizens
increase if R0 is greater than 1 whereas R0 is 2.2 for above 65 years (except for public representatives/
COVID-1997. Further analysis of 12 available studies government servants/medical professionals) to remain
found that R0 was 3.2898. R0 is also considered a super at home and avoid mass gatherings unless there is a
spreader as it is an average value. It may hugely be medical reason and essential services requirement. A
responsible for outbreaks within large clusters but not high-level Group of Ministers is constantly reviewing
influence the R0 value99. During the acute phase or pre- the status of cases in India. Necessary steps are
pandemic, R0 may be unstable94. Hence it is required to being implemented by the Government of India across
focus on reducing the value to less than 1 to control the states. Social distancing measures have been issued
infection. Preventive measures are the only strategy to by the government advisory board to slow down the
limit the spread of cases. Preventive measures included rate and extent of disease transmission. Non-urgent
the isolation of the patients with careful infection control. hospitalization and elective surgeries are avoided by the
Simultaneously appropriate measures have to be taken instruction of the health advisory board in consultation
during the diagnosis and clinical care of the infected with professional associations. This was to maintain
patient. Sputum induction and droplet contact should be a strategic distance from hospital-related infections
avoided during sample collection. Airborne precautions to the vulnerable and prepare hospitals effectively for
should be taken while collecting the sample. The effective meeting current and future challenges presented by
way to stop the spread of the disease is by disrupting the COVID-19103. Ministry of Health and Family Welfare was
chain of transmission. Further spreading of the infection
regularly evaluating quarantine facilities. In addition to
in clinics and hospitals can be limited by applying triage,
that preparedness of the hospital in terms of adequate
following correct infection control measures, isolating the
isolation wards, OPD blocks, availability of testing kits,
cases, and contact tracing100. Middle-aged and elderly
medicines, and personal protective equipment (PPEs),
patients with primary chronic diseases, especially high
etc. are evaluated. All public hospitals have been directed
blood pressure and diabetes, were found to be more
susceptible to respiratory failure and, therefore, had to ensure sufficient accessibility of protective gear for all
poorer prognoses. Providing respiratory support at early healthcare workers104. A confirmed covid-19 case must
stages improved the disease prognosis and facilitated be hospitalized and placed in a single patient room with
recovery101. The WHO and other organizations have negative pressure – a minimum of 6 charges per hour.
issued the following general recommendations: Exhausted air has to be filtered through High-Efficiency
Particulate Air (HEPA) and medical personnel entering
Ø Avoid close contact with subjects suffering from acute the room need to wear PPE particularly facemask, gown,
respiratory infections. and eye protection105. The greatest risk of COVID-19
INDIAN DRUGS 60 (05) MAY 2023 15
is transmission to healthcare workers. In the SARS workers also plays an important aspect in the response.
outbreak of 2002, 21% of those affected were healthcare Health professionals should be aware of the precautions
workers106. necessary to avoid the transmission and spread of the
disease. Accurate diagnosis in the early stages of the
COVID-19 modeling with India SIM predicted that the epidemic helps control the spread of the disease. More
community transmission of COVID-19 in INDIA most likely so future outbreaks of viruses are likely to continue. So,
started in early March 2020. To stop the transmission,
comprehensive measures should be devised to prevent
state or local containment was the best option rather
future outbreaks. However, the development of suitable
than National containment. Approximately 300 and 400
therapeutic agents such as designing antiviral drugs
million Indians were likely to be infected by July 2020,
and vaccines against COVID-19 will help to control the
without interventions. Most of these cases would be mild.
infection.
Somewhere between April and May 2020, around 100
million individuals would be infected. Amongst them,
approximately 10 million would be severed and about REFERENCES
2-4 million will require hospitalization (Fig. 3 & Fig. 4). As 1. Cascella M., Rajnik M., Cuomo A., Dulebohn S.C. and Napoli
per the report, this may be the most dangerous period. R.D.: Features, Evaluation and Treatment Coronavirus
(COVID-19), StatPearls - NCBI Bookshelf, 2020.
This peak load would be reduced by 75% by generalized
social distancing. It would be a major issue of hospital 2. Sharma A., Tiwari S., Deb M.K. and Marty J.L.: Severe acute
respiratory syndrome coronavirus-2 (SARS-CoV-2): a global
outbreaks of COVID-19 induced by the admission of
pandemic and treatment strategies, Int. J. Antimicrob.
infected patients into hospitals. Thus there is a need for Agents., 2020, 56(2), 106054.
large temporary hospitals to handle this patient load over 3. Worldometer, Covid-19 Coronavirus Pandemic,
the next three months period. Hospital-based secondary Available at https://www.worldometers.info/
transmission may fuel the epidemic107. coronavirus/?fbclid=IwAR0zkpRD_zQZb4UkziGI_
Xvv75s5Q3eynf7-f9pOspxGbgHbe7OqpGBrIBI (Access
On 11th July 2020, India started Phase-I clinical trials, Date-04 March 2020)
16 candidates were opted and examined at AIIMS, Delhi. 4. Li X., Geng M., Peng Y., Meng L. and Lu S.: Molecular
Usually, it takes 8-10 years for vaccines to reach the immune pathogenesis and diagnosis of COVID-19, J.
market from labs, but in the case of COVID vaccines due Pharm. Anal., 2020,10(2), 102-108.
to emergencies, this period is shortened to a few months. 5. World Health Organization, 72nd Session of the WHO
The shortening of the time duration was done by limiting Regional Committee for Europe, Available at http://
the time of regulatory approvals (licensing registration www.euro.who.int/en/health-topics/health-emergencies/
coronavirus-covid-19/news/news/2020/3/who-announces-
applications and submissions authorized by CDSCO) and
covid-19-outbreak-a-pandemic. Access Date- 19 September
not the specific approvals and thus not comprising with
2021.
vaccines safety and efficacy108. Due to crises phases of
6. World Health Organization, WHO Coronavirus (COVID-19)
clinical trials were done by combining various steps of
Dashboard, Available at https://covid19.who.int. Access
different phases. Out of 25 vaccine trials, India offered
Date- 01 February 2020.
a total of 7 vaccines109-115 (Table II). DCGI permitted 2
vaccines- Bharat Biotech’s Covaxin and ZyCoV-D by 7. John Hopkins University & Medicine, Coronavirus Resource
Center, Available at https://coronavirus.jhu.edu › map.
Zydus Cadila116,117.
Access Date -01 February 2020.
8. Chan J.F., To K.K., Tse H., Jin D.Y. and Yuen K.Y.:
CONCLUSION
Interspecies transmission and emergence of novel viruses:
Since the first outbreak of coronavirus (COVID-19) in lessons from bats and birds, Trends Microbiol., 2013,
Wuhan, China, the disease spread worldwide. The current 21(10), 544-555.
COVID-19 pandemic is an international public health 9. Chen Y., Liu Q. and Guo D., Emerging coronaviruses:
problem. This new virus outbreak has challenged the Genome structure, replication, and pathogenesis, J. Med.
economic, medical, and public health infrastructure of the Virol., 2020, 92(4), 418-423.
whole world. Individuals at extreme ages are at higher risk. 10. Huang C., Wang Y., Li X., Ren L., Zhao J., Hu Y., Zhang
Risk is more significant in the case of immunocompromised L., Fan G., Xu j., Gu X. , Cheng Z. , Yu T. , Xia J. , Wei
Y. , Wu W. , Xie X. , Yin W. , Li H., Liu M. , Xiao Y., Gao H. ,
patients. Complete elimination of risk is not possible
Guo L. , Xie J. , Wang G. , Jiang R. , Gao Z. , Jin Q. , Wang
but prudent adjustments may be warranted. All health J. and Cao B.: Clinical features of patients infected with
care workers should understand the presentation of the 2019 novel coronavirus in Wuhan, China, Lancet, 2020,
disease and workup. Supportive care by the health care 6736(20), 30183-30185.
16 INDIAN DRUGS 60 (05) MAY 2023
11. Peiris J.S., Guan Y. and Yuen K.Y.: Severe acute respiratory 99 cases of 2019 novel coronavirus pneumonia in Wuhan,
syndrome, Nat. Med., 2004, 10(12 Suppl), S88-97. China: a descriptive study. Lancet, 2020,395,10223,
12. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L., Fan P507-513.
G., Xu j., Gu X. , Cheng Z. , Yu T. , Xia J. , Wei Y. , Wu W. , 26. Liu Y., Gayle A.A., Wilder-Smith A. and Rocklöv J.: The
Xie X. , Yin W. , Li H., Liu M. , Xiao Y., Gao H. , Guo L. , Xie reproductive number of COVID-19 is higher compared to
J. , Wang G. , Jiang R. , Gao Z. , Jin Q. , Wang J. and Cao SARS coronavirus. J. Travel. Med., 2020, 27(2), taaa021.
B.: Clinical features of patients infected with 2019 novel 27. Schoeman D. and Fielding B.C.: Coronavirus envelope
coronavirus in Wuhan, China, Lancet, 2020,15, 395(10223), protein: current knowledge. J. Virol., 2019, 16, 69.
497-506.
28. Pardi N., Hogan M. J., Porter F.W. and Weissman D.:
13. Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y., Qiu Y., mRNA vaccines — a new era in vaccinology. Nat. Rev.
Wang J., Liu Y., Wei Y., Xia J., Yu T., Zhang X. and Zhang Drug. Discov., 2018, 17(4), 261–279.
L.: Epidemiological and clinical characteristics of 99 cases
29. World Health Organization, Tracking SARS-CoV-2 Variants,
of 2019 novel coronavirus pneumonia in Wuhan, China: a
Available athttps://www.who.int/activities/tracking-SARS-
descriptive study, Lancet, 2020, 395(10223), 507-513.
CoV-2-variants. Access Date- 19 September 2020.
14. Liu Y., Gayle A.A., Wilder-Smith A. and Rocklöv J.: The
30. Wang D., Hu B., Hu C., Zhu F., Liu X., Zhang J., Wang
reproductive number of COVID-19 is higher compared to
B., Xiang H., Cheng Z., Xiong Y., Zhao Y., Li Y., Wang
SARS coronavirus. J. Travel. Med., 2020, 27(2), taaa021.
X. and Peng Z.: Clinical characteristics of 138 hospitalized
15. Mahase E.: Coronavirus covid-19 has killed more people patients with 2019 novel coronavirus-infected pneumonia
than SARS and MERS combined, despite lower case fatality in Wuhan, China. JAMA, 2020, 323(11),1061-1069.
rate, BMJ, 2020, 368, m641.
31. Zhu N., Zhang D., Wang W., Li X., Yang B., Song J., Zhao
16. Fehr A.R. and Perlman S.: Coronaviruses: an overview of X., Huang B., Shi W., Lu R., Niu P. and Zhan F.: A novel
their replication and pathogenesis. Methods. Mol. Biol., coronavirus from patients with pneumonia in China, 2019.
2015, 1282, 1–23. N. Engl. J. Med., 2020, 382(8), 727-733.
17. Chan J.F., Kok K.H., Zhu Z., Chu H., To K.K., Yuan S. and 32. Chen H., Guo J., Wang C., Luo F., Yu X., Zhang W., Li J.,
Yuen K.Y.: Genomic characterization of the 2019 novel Zhao D., Xu D., Gong G., Liao J., Hou W. and Zhang Y.:
humanpathogenic coronavirus isolated from a patient with Clinical characteristics and intrauterine vertical transmission
atypical pneumonia after visiting Wuhan. Emerg. Microbes, potential of COVID-19 infection in nine pregnant women:
Infect., 2020, 9, 221–236. a retrospective review of medical records. Lancet, 2020,
18. Zhu N., Zhang D., Wang W., Li X., Yang B., Song J., Zhao 395(10226), 809-815.
X., Huang B., Shi W., Lu R., Niu P. and Zhan F.: A novel 33. Bai Y., Yao L., Wei T., Tian F., Jin D.Y., Chen L. and
coronavirus from patients with pneumonia in China, 2019. Wang M.: Presumed asymptomatic carrier transmission
N. Engl. J. Med., 2020, 382, 727–733. of COVID-19. JAMA., 2020, 323(14),1406-1407.
19. Brian D.A. and Baric R.S.: Coronavirus genome structure
34. Chan JF-W., Yuan S., Kok K-H., Tokk W., Chu H., Yang J.,
and replication. Curr. Topics. Microbiol. Immunol., 2005,
Xing F.., Liu J., Yip C.C., Poon R.W., Tsoi H-W., Lo S.K .,
287, 1– 30.
Chan K-H., Poon V.K.., Chan W-M., Ip J.D .,Cai J-P. , Cheng
20. Nakagawa K., Lokugamage K.G. and Makino S.: Viral and
V-C ., Chen H., Hui C.K. and Yuen K.W.: A familial cluster
cellular mRNA translation in coronavirus-infected cells.
Adv. Virus. Res., 2016, 96, 165–192. pneumonia associated with the 2019 novel coronavirus
indicating person to person transmission a study of family
21. Snijder E. J., Van der Meer Y., Zevenhoven-Dobbe J.,
Onderwater J. J. M., Van der Meulen J., Koerten H. K. and cluster. Lancet, 2020, 395(10223), 514-523
Mommaas A. M.: Ultrastructure and origin of membrane 35. Deng S. Q. and Peng H. J.: Characteristics of and Public
vesicles associated with the severe acute respiratory Health Responses to the Coronavirus Disease 2019
syndrome coronavirus replication complex. J. Virol., 2006, Outbreak in China. J. Clin. Med., 2020, 9(2), 575.
80, 5927–5940. 36. World Health Organization. Novel coronavirus situation
22. Hussain S., Pan J., Chen Y., Yang Y., Xu J., Peng Y., Wu report -2. January 22, 2020, Available at https://www.
Y., Li Z., Zhu Y., Tien P., and Guo D.: Identification of novel who.int/docs/default-source/coronaviruse/situation-
subgenomic RNAs and noncanonical transcription initiation reports/20200122-sitrep-2-2019-ncov.pdf. Access Date- 01
signals of severe acute respiratory syndrome coronavirus. February 2020.
J. Virol., 2005, 79, 5288–5295.
37. Zou L., Ruan F., Huang M., Liang L., Huang H., Hong Z.,
23. Chen Y., Liu Q. and Guo D.: Emerging coronaviruses: Yu J., Kang M., Song Y., Xia J., Guo Q., Song T., He J .,
Genome structure, replication, and pathogenesis. J. Med. Yen H.L., Peiris M. and Wu J.: SARS-CoV-2 Viral Load
Virol., 2020, 92(4), 418-423. in Upper Respiratory Specimens of Infected Patients. N.
24. Peiris J.S., Guan Y. and Yuen K.Y.: Severe acute respiratory Engl. J. Med., 2020, 382(12), 1177-1179.
syndrome. Nat. Med., 2004, 10, S88-97. 38. World Health Organization. Infection prevention and
25. Chen N., Zhou M., Dong X., Qu J., Gong F., Han Y., Qiu control of epidemic- and pandemic-prone acute respiratory
Y., Wang J., Liu Y., Wei Y., Xia J., Yu T., Zhang X. and infections in health care. Geneva: World Health Organization;
Zhang L.: Epidemiological and clinical characteristics of 2014.
INDIAN DRUGS 60 (05) MAY 2023 17
39. Liu J., Liao X., Qian S., Yuan J., Wang F., Liu Y., Wang A.M. and Rolfes M.A.: Active Monitoring of Persons Exposed
Z., Wang FS., Liu L. and Zhang Z.: Community transmission to Patients with Confirmed COVID-19 — United States,
of severe acute respiratory syndrome coronavirus 2, January–February 2020. MMWR. Morb. Mortal. Wkly.
Shenzhen, China, 2020. Emerg. Infect. Dis., 2020, 26(6), Rep., 2020, 69(9), 245-246.
1320-1323. 51. Rothe C., Schunk M., Sothmann P., Bretzel G., Froeschl
40. Li Q., Guan X., Wu P., Xiaoy W., Zhou L., Tong Y., Ren G., Claudia W., Zimmer T., Thiel V., Janke C., Guggemos
R., Leung KS., Lau HY., Wong JY., Xing X. and Xiang N.: W., Seilmaier M., Drosten C., Vollmar P., Zwirglmaier
Early transmission dynamics in Wuhan, China, of novel K., Zange S., Wölfel R. and Hoelscher M.: Transmission
coronavirus-infected pneumonia. N. Engl. J. Med., 2020, of 2019-nCoV Infection from an Asymptomatic Contact in
382(13), 1199-1207. Germany. N. Engl. J. Med., 2020, 382, 970.
41. Burke R.M., Midgley C.M., Dratch A., Fenstersheib M., Haupt 52. Huang L., Zhang X., Zhang X., Wei Z, Zhang L., Xu J.,
T., Holshue M., Ghinai I., Jarashow M.C., Lo J., McPherson Liang P., Xu Y., Zhang C. and Xu A.: Rapid asymptomatic
T.D., Rudman S., Scott S., Hall A.J., Fry A.M. and Rolfes transmission of COVID-19 during the incubation period
M. A: Active monitoring of persons exposed to patients demonstrating strong infectivity in a cluster of youngsters
withconfirmed COVID-19 — United States, January– aged 16-23 years outside Wuhan and characteristics of
February 2020. MMWR. Morb. Mortal. Wkly. Rep., 2020, young patients with COVID-19: A prospective contact-tracing
69(9), 245-246. study. J. Infect., 2020, 80(6), e1–e13.
42. World Health Organization. Report of the WHO-China Joint 53. Yu P., Zhu J., Zhang Z. and Han Y.: A familial cluster
Mission on Coronavirus Disease 2019 (COVID-19) 16-24 of infection associated with the 2019 novel coronavirus
February 2020, Available at https://www.who.int/docs/ indicating potential person-to-person transmission during
default-source/coronaviruse/who-china-joint-mission-on- the incubation period. J. Infect. Dis., 2020, 221(11), 1757-
covid-19-final-report.pdf (Access Date 24 Feb 2020). 1761.
43. Kampf G., Todt D., Pfaender S. and Steinmann E.: 54. Hu Z., Song C., Xu C., Jin G., Chen Y., Xu X., Ma H., Chen
Persistence of coronaviruses on inanimate surfaces and W., Lin Y., Zheng Y., Wang J., Hu Z, Yi Y. and Shen H.:
its inactivation with biocidal agents. J. Hosp. Infect., 2020, Clinical characteristics of 24 asymptomatic infections with
104(3), 246-251. COVID-19 screened among close contacts in Nanjing,
44. World Health Organization, Situation reports, Available China. Sci. China. Life. Sci., 2020, 63(5), 706-711.
at: https://www.who.int/emergencies/diseases/ 55. Li Z., Yi Y., Luo X., Xiong N., Liu Y., Li S., Sun R., Wang
novelcoronavirus-2019/situation-reports/. Access Date- Y., Hu B., Chen W., Zhang Y., Wang J., Huang B., Lin Y.,
19 September 2021 Yang J., Cai W., Wang X., Cheng J., Chen Z., Sun K., Pan
45. Huijun C., Juanjuan G., Chen W., Fan L., Xuechen Y., Wei W., Zhan Z., Chen L. and Ye F.: Development and Clinical
Z., Jiafu L., Zhao D., Xu D.,Gong Q.,Liao J.,Yang H., Hou Application of A Rapid IgM-IgG Combined Antibody Test
W. and Zhang Y.: Clinical characteristics and intrauterine for SARS-CoV-2 Infection Diagnosis. J. Med. Virol., 2020,
vertical transmission potential of COVID-19 infection in 92(9), 1518-1524.
nine pregnant women: a retrospective review of medical 56. Centers for Disease Control and Prevention, Interim Clinical
records. Lancet, 2020, 395(10226), 809–815. Guidance for Management of Patients with Confirmed 2019
46. Cheng Z.J. and Shan J.: 2019 novel coronavirus: where Novel Coronavirus (2019-nCoV) Infection, Available at
we are and what we know. Infection, 2020, 48(2),155- https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-
163. guidance-management-patients.html. Access Date- 14
47. Behl T., Kaur I., Bungau S., Kumar A., Uddin M.S., Kumar February 2020.
C., Pal G., Sahil., Shrivastava K., Zengin G. and Arora S.: 57. Tang A., Tong Z.D., Wang H.L., Dai Y.X., Li K.F., Liu J.N.,
The dual impact of ACE2 in COVID-19 and ironical actions Wu W., Yuan C., Yu M., Li P., and Yan J.: Detection of
in geriatics and pediatrics with possible therapeutic solution. Novel Coronavirus by RT-PCR in Stool Specimen from
Life. Sci., 2020, 257, 118075. Asymptomatic Child, China. Emerg. Infect. Dis., 2020,
48. Zou L., Ruan F., Huang M., Liang L., Huang H., Hong Z., 26(6), 1337-1339.
Yu J., Kang M., Song Y., Xia J., Guo Q. , Song T. , He 58. Wang W., Xu Y., Gao R., Lu R., Han K., Wu G. and Tan
J., Yen H.L. , Peiris M. and Wu J.: SARS-CoV-2 Viral Load W.: Detection of SARS-CoV-2 in Different Types of Clinical
in Upper Respiratory Specimens of Infected Patients. N. Specimens. JAMA., 2020, 323(18), 1843–1844.
Engl. J. Med., 2020, 382(12), 1177-1179. 59. WHO | First data on stability and resistance of SARS
49. Report of the WHO-China Joint Mission on Coronavirus coronavirus compiled by members of WHO laboratory
Disease 2019 (COVID-2019). February 16-24, 2020. http:// network, Available at https://www.who.int/publications/m/
www.who.int/docs/default-source/coronaviruse/who-china- item/first-data-on-stability-and-resistance-of-sars-
joint-mission-on-covid-19-final-report.pdf. (Access Date- 04 coronavirus-compiled-by-members-of-who-laboratory-
March 2020). network. Access Date- 19 September 2021.
50. Burke R.M., Midgley C.M., Dratch A., Fenstersheib 60. Ye Q., Wang B. and Mao J.: The pathogenesis and treatment
M., Haupt T., Holshue M., Ghinai I, Jarashow C.M., Lo of the “Cytokine Storm” in COVID-19. J. Infect., 2020,
J., McPherson T.D., Rudman S., Scott S., Hall A.J., Fry 80(6), 607–613.
18 INDIAN DRUGS 60 (05) MAY 2023
61. Guan G.W., Gao L., Wang J.W., Wen X.J., Mao T.H., Peng of Optimized Dosing Design of Hydroxychloroquine for
S.W., Zhang T., Chen X.M. and Lu F.M..: Exploring the the Treatment of Severe Acute Respiratory Syndrome
mechanism of liver enzyme abnormalities in patients with Coronavirus 2 (SARS-CoV-2). Clin. Infect. Dis., 2020,
novel coronavirus-infected pneumonia. Zhonghua Gan 71(15), 732-739.
Zang Bing Za Zhi., 2020, 28(2), 100-106. 72. Cortegiani A., Ingoglia G., Ippolito M., Giarratand A. and
62. Wit E. de., Doremalen N.v., Falzarano D. and Munster Einav S.: A systematic review on the efficacy and safety of
V.J.: SARS and MERS: recent insights into emerging chloroquine for the treatment of COVID-19. J. Crit. Care,
coronaviruses. Nat. Rev. Microbiol., 2016, 14, 523-534. 2020, 57, 279-283.
63. Zumla A., Chan J.F., Azhar E.I., Hui D.S., and Yuen K.Y.: 73. Groneberg D.A., Poutanen S.M., Low D.E., Lode H., Welte
Coronaviruses - drug discovery and therapeutic options. T. and Zabel P.: Treatment and vaccines for severe acute
Nat. Rev. Drug Discovery., 2016, 15(5), 327-347. respiratory syndrome. Lancet Infect. Dis., 2005, 5,147.
64. Huang C., Wang Y., Li X., Ren L., Zhao J., Hu Y., Zhang L., 74. Chan J.F., Yao Y., Yeung M.L., Deng W., Bao L., Jia L.,
Fan G., Xu J., Gu X., Cheng Z., Yu T., Xia J., Wei Y., Wu Li F., Xiao C., Gao H., Yu P., Cai J.P., Chu H., Zhou J.,
W., Xie X., Yin W., Li H., Liu M., Xiao Y., Gao H., Guo L., Xie Chen H., Qin C. and Yuen KY.: Treatment with Lopinavir/
J., Wang G., Jiang R., Gao Z., Jin Q., Wang J. and Cao Ritonavir or Interferon-β1b Improves Outcome of MERS-
B.: Clinical features of patients infected with 2019 novel CoV Infection in a Nonhuman Primate Model of Common
coronavirus in Wuhan, China. Lancet, 2020, 395(10223), Marmoset. J. Infect. Dis., 2015, 212(12), 1904-1013.
497-506. 75. Lim J., Jeon S., Shin H.Y., Kim M.J., Seong Y.M., Lee
65. Groneberg D.A., Hilgenfeld R. and Zabel P.: Molecular W.J., Choe K.W., Kang Y.M., Lee B. and Park S. J.: Case
mechanisms of severe acute respiratory syndrome (SARS). of the Index Patient Who Caused Tertiary Transmission
Respir. Res., 2005, 6(1), 8. of COVID-19 Infection in Korea: The Application of
66. Lu P.R., Zhao X., Li J., Nia P., Yang B., Wu H., Wang W., Lopinavir/Ritonavir for the Treatment of COVID-19 Infected
Song H., Huang B., Zhu N., Bi Y., Ma X., Zhan F., Wang L., Pneumonia Monitored by Quantitative RT-PCR. J. Korean.
Hu T., Zhou H., Hu Z., Zhou W., Zhao L., Chen J., Meng Y., Med. Sci., 2020, 35(6), e79.
Wang J., Lin Y., Yuan J., Xie Z., Ma J., Liu M.J., Wang D., 76. Wang Z., Chen X., Lu Y., Chen F. and Zhang W.: Clinical
Xu W., Holmes E.C., Gao F.G., Wu G., Chen W., Shi W., characteristics and therapeutic procedure for four cases
and Tan W.: Genomic characterisation and epidemiology with 2019 novel coronavirus pneumonia receiving combined
of 2019 novel coronavirus: implications for virus origins and Chinese and Western medicine treatment. Biosci Trends.,
receptor binding, Lancet, 2020, 395(10224), 565-574. 2020, 14(1), 64-68.
67. Gilead Sciences Statement on the Company’s Ongoing 77. Young B.E., Ong S.W.X., Kalimuddin S., Low J.G., Tan S.Y.,
Response to the 2019 Novel Coronavirus (2019-nCoV), Loh J., Ng O.T., Marimuthu K., AngL.W., Mak T.M., Lau
Available at https://www.gilead.com/news-and-press/ S.K., Anderson D.E., Chan K.S., Tan T.Y., Ng T.Y., Cui
company-statements/gilea d-sciences-statement-on-the- L., Said Z., Kurupatham L., Chen M.I.C., Chan M., Vasoo S.,
company-ongoing-response-to-the-2019-new-coronavirus. Wang L.F., Tan B.H., Lin R.T.P., Lee V.J.M., Leo Y.S. and
Access Date- 02 February 2020. Lye D.C.: Epidemiologic Features and Clinical Course of
68. Sheahan T.P., Sims A.C., Graham R.L., Menachery Patients Infected With SARS-CoV-2 in Singapore, JAMA,
V.D., Grelinski L.E., Case J.B., Leist S.R., Pyrc K., Feng 2020, 323,1488-1494.
J.Y., Trantcheva I., Bannister R., Park Y., Babusis D., Clarke 78. Reuters. China approves use of Roche drug in battle against
M.O., Mackman R.L., Spahn J.E., Palmiotti C.A., Siegel D., coronavirus complications. Available at https://www.reuters.
Ray A.S., Cihlar T., Jordan R., Denison M.R. and Baric R.S.: com/article/us-health-coronavirus-china-roche-hldg/china-
Broad-spectrum antiviral GS-5734 inhibits both epidemic approves-use-of roche-arthritis-drug-for-coronavirus-
and zoonotic coronaviruses. Sci. Transl. Med., 2017, patients-idUSKBN20R0LF. Access Date- 11 March 2020.
9(396), eaal3653. 79. Vincent M.J., Bergeron E., Benjannet S., Erickson
69. Wang M., Cao R., Zhang L., Yang X., Liu J., Xu M., Shi Z., R.B., Rollin P.E., Ksiazek G.T., Seidah N.G. and Nicho
Hu Z., Zhong W. and Xiao G.: Remdesivir and chloroquine S.T.: Chloroquine is a potent inhibitor of SARS coronavirus
effectively inhibit the recently emerged novel coronavirus infection and spread. Virol. J., 2005, 2, 69.
(2019-nCoV) in vitro. Cell. Res., 2020, 30, 269-271. 80. Cheng V.C.C., Wong S.C., To K.K.W., Ho P.L. and
70. Holshue M.L., DeBolt C., Lindquist S., Lofy H.K., Wiesman Yuen K.Y.: Preparedness and proactive infection control
J., Bruce H., Spitters C., Ericson K., Wilkerson S., Tural measures against the emerging Wuhan coronavirus
A., Diaz G., Cohn A., Fox L., Patel A., Gerber S.I., Kim L., pneumonia in China. J. Hosp. Infect., 2020, 104, 254–255.
Tong S., Lu X., Lindstrom S., Pallansch M.A., Weldon W.C., 81. Sheahan T.P., Sims A.C., Leist S.R., Schäfer A., Won
Biggs H.M., Uyeki T.M. and Pillai S.K.: First Case of 2019 J., Brown A.J., Montgomery S.A., Hogg A., Babusis
Novel Coronavirus in the United States. N. Engl. J. Med., D., Clarke M.O., Spahn J.E., Bauer L., Sellers S., Porter
2020, 382(10), 929-936. D., Feng J.Y., Cihlar T., Jordan R., Denison M.R. and Baric
71. Yao X., Ye F., Zhang M., Cui C., Huang B., Niu P., Liu R.S.: Comparative therapeutic efficacy of remdesivir and
X., Zhao L., Dong E., Song C., Zhan S., Lu R., Li H., Tan combination lopinavir, ritonavir, and interferon beta against
W., and Liu D.: In vitro Antiviral Activity and Projection MERS-CoV. Nat. Commun., 2020, 11, 222.
INDIAN DRUGS 60 (05) MAY 2023 19
82. Graham R.L., Donaldson E.F. and Baric R.S.: A decade after W., Lee K.H., Lau E.M.C., Ferguson N.M. and Anderson
SARS: strategies for controlling emerging coronaviruses. R.M.: Transmission dynamics of the etiological agent of
Nat Rev Microbiol., 2013, 11, 836–848. SARS in Hong Kong: impact of public health interventions.
83. Yang Z.Y., Kong W.P., Huang Y., Roberts A., Murphy B.R., Science, 2003, 300(5627), 1961-6.x.
Subbarao K. and Nabel G. J.: A DNA vaccine induces 96. Yang Y., Sugimoto J.D., Hallosan M.E., Basta N.E.,Chao
SARS coronavirus neutralization and protective immunity D.L., Matrajt L., Potter G., Kenah E. and Longini Jr I.M..:
in mice. Nature, 2004, 428, 561–564. The transmissibility and control of pandemic influenza A
84. Chu C.M., Cheng V.C., Hung I.F., Wong M.M., Chan K.H., (H1N1) virus. Science, 2009, 326(5953),729-733.
Chan K.S., Kao R.Y.T., Poon L.L.M., Wong C.L.P.,Guan 97. Li Q., Guan X., Wu P., Wang X., Zhou L., Tong Y., Ren R.,
Y., Peiris J.S.M., Yuen K.Y. and HKU/UCH SARS Study Leung K.S.M., Lau E.H.Y., Wong J.Y., Xing X. and Xiang
Group .: Role of lopinavir/ritonavir in the treatment of SARS: N.: Early transmission dynamics in Wuhan, China of novel
initial virological and clinical findings. Thorax, 2004, 59, coronavirus-infected pneumonia. N. Eng. J. Med., 2020,
252–256. 382(13), 1197-1207.
85. Kumar V., Jung Y.S. and Liang P.H.: Anti-SARS coronavirus 98. Liu Y., Gayle A.A., Smith A.W. and Rocklöv J.: The
agents: a patent review (2008–present). Expert. Opin. reproductive number of COVID-19 is higher compared to
Ther. Pat., 2013, 23, 1337–1348. SARS Coronavirus. J. Travel. Med., 2020, 27(2), taaa021.
86. Li E., Yan F., Huang P., Chi H., Xu S., Li G., Liu C., Feng 99. Kucharski A. and Acthaus C.: The role of superspreading
N., Wang H., Zhao Y., Yang S. and Xia X.: Characterization in Middle respiratory syndrome coronavirus (MERS-CoV)
of the immune response of MERS-CoV vaccine candidates transmission. Euro. Surveilli., 2015, 20(25), PII 21167.
derived from two different vectors in mice. Viruses, 2020,12, 100. Cheng V.C.C., Wong S.C., To K.K.W., Ho P.L. and
125. Yuen K.Y.: Preparedness and proactive infection control
87. Du L., He Y., Zhou Y., Liu S., Zheng B.J. and Jiang S.: measures against the emerging Wuhan coronavirus
2009. The spike protein of SARS-CoV—a target for vaccine pneumonia in China. J. Hosp. Infect., 2020,104, 254–255.
and therapeutic development. Nat. Rev. Microbiol., 2009, 101. Kui L., Fang Y.Y., Deng Y., Liu W., Wang M.F., Ma J.P.,
7, 226–236. Xiao W., Wang Y.N., Zhong M.H., Li C.H., Li G.C. and Liu
88. Chen R., Fu J., Hu J., Li C., Zhao Y., Qu H., Wen X., Cao H.G.: 2020. Clinical characteristics of novel coronavirus
S., Wen Y., Wu R., Zhao Q., Yan Q., Huang Y., Ma X., Han cases in tertiary hospitals in Hubei Province. Chin. Med.
X. and Huang X.: 2020. Identification of the immunodominant J., 2020, 133, 1025–1031.
neutralizing regions in the spike glycoprotein of porcine 102. World Health Organization, Novel Coronavirus Disease
deltacoronavirus. Virus. Res., 2020, 276, 197834. (COVID-19) Situation Update Report-9, Available at https://
89. Precision Vaccinations, 2020. Coronavirus vaccines, www.who.int › india-situation-report-9. Access Date-25
Available at https://www.precisionvaccinations.com/ March 2020.
vaccines/coronavirus-vaccines. Access Date- 19 103. W orld Health Organization. Novel Coronavirus
September 2021. Disease (COVID-19) Situation Update Report
90. WHO. 2020. Draft landscape of COVID-19 candidate -8, Available at https://www.who.int/docs/default-
vaccines–20 March 2020. Available at https://www.who.int/ source/wrindia/situation-report/india-situation-
blueprint/priority-diseases/key-action/novel-coronavirus- report 8bc9aca340f91408b9efbedb3917565fc.
landscape-ncov.pdf?ua=1. Access Date- 19 September pdf?sfvrsn=5e0b8a43_2 (Access Date-25 March 2020).
2021. 104. M inistry of Health and Family Welfare Directorate
91. Graham R.L., Donaldson E.F. and Baric R.S.: A decade after General of Health Services [Emergency Medical
SARS: strategies for controlling emerging coronaviruses. Relief], Novel Coronavirus Disease 2019(COVID-19):
Nat. Rev. Microbiol., 2013, 11, 836-848. Guidelines on rational use of Personal Protective
92. India Today, US: Coronavirus vaccine test opens Equipment, Available at https://www.mohfw.gov.in/pdf/
with first doses, Available at https://www.indiatoday. GuidelinesonrationaluseofPersonalProtectiveEquipment.
in/world/story/us-coronavirus-vaccine-test-opens-1st- pdf. Access Date- 16 May 2021.
doses-1656207-2020-03-16. Access Date-19 September 105. Jernigan D.B.: Update: Public Health Response to the
2021. Coronavirus Disease 2019 Outbreak-United States
93. The Wall Stree Journal, Wanted: People willing to get sick februaryb24 2020. Centre for Diseases Control and
to find coronavirus vaccine , Available at https://www.wsj. Prevention, MMWR. Morb. Mortal. Wkly. Rep., 2020,
com/articles/wanted-people-willing-to-get-sick-to-find- 69(8), 216-219.
coronavirus-vaccine-11584615600. Access Date- 19 March 106. De C., Huiwen X., Andre R., Lokesh S., Cruz D. and Cruz
2020. C.S.D.: Protecting health-care workers from subclinical
94. Bauch C. and Oraby T.: Assessing the pandemic potential coronavirus infection. Lancet Resp. Med., 2020, 8(3), e13.
of MERS-Cov. Lancet, 2013, 382(9893), 662-664. 107. Siddiqui A.F.,Wiederkehr M.,Rozonova L. and Flahault A.:
95. Riley S., Fraser C., Donelly C.A., Ghani A.C., Abu-Raddad Situation of India in the COVID-19 Pandemic: India’s Initial
L.J., Hedley A.J., Leung G.M., Ho L.M., Lam T.H., Thach Experience. Int. J. Environ. Res. Public Health, 2020,
T.Q., Chau P., Chan K.P., Lo S.V., Leung P.Y., Tsang T., Ho 17(3), 8994.
20 INDIAN DRUGS 60 (05) MAY 2023
108. Perapeddan B.S.: AIIMS to start phase-I testing of 114. World Health Organization, The Novavax Vaccine against
indigenous COVID-19 vaccine, Available at https://www. COVID-19: What you need to know, Available at https://www.
thehindu.com/news/national/aiims-to-start-phase-1- who.int/news-room/feature-stories/detail/the-novavax-
testing-of-indigenous-covid-19-vaccine/article32142671. vaccine-against-covid-19-what-you-need-to-know. Access
ece. Access Date- 20 July 2020. Date-13 June 2022.
109. Coronavirus disease (COVID-19): Vaccines, ChAdOx1 nCov- 115. Precession Vaccinations, ZyCoV-D COVID-19 Vaccine,
19 Corona Virus Vaccine (Recombinant) COVISHIELDTM, Available at https://www.precisionvaccinations.com/
Available at https://www.seruminstitute.com/product_ vaccines/zycov-d-covid-19-vaccine. Access Date-23
covishield.php. Access Date-23 August 2022. August 2022.
110. COVAXIN®- India’s First Indigenous COVID-19 Vaccine 116. World Health Organization, Accelerating a safe and
Available at https://www.bharatbiotech.com/covaxin.html. effective COVID-19 Vaccine, Available at https://www.who.
Access Date-23 August 2022. int/emergencies/diseases/novel-coronavirus-2019/global-
111. Moderna COVID-19 Vaccine, Centers for Disease Control research-on-novel-coronavirus-2019-ncov/accelerating-a-
and Prevention, Available at https://www.cdc.gov/vaccines/ safe-and-effective-covid-19-vaccine. Access Date 26 April
covid-19/info-by-product/moderna/index.html. Access 2022.
Date-23 August 2022. 117. M andaviya M.: COVID-19: Covaxin, Corbevax,
112. Sputnik V The first registered COVID-19 vaccine, Available ZyCoV-D get emergency use nod by drug regulator,
at https://sputnikvaccine.com/. Access Date-23 August 2022. Available at https://www.cnbctv18.com/healthcare/
covid-19-bharat-biotechs-covaxin-gets-dgci-nod-for-
113. Jansen (Johnson & Johnson) COVID-19 Vaccine, Centers
children-between-6-12-years-13278482.htm. Access
for Disease Control and Prevention, Available at https://
Date- 26 April 2022.
www.cdc.gov/vaccines/covid-19/info-by product/janssen/
index.html. Access Date-06April 2022.
NOW AVAILABLE ! IDMA-APA GUIDELINES /
TECHNICAL MONOGRAPHS
TECHNICAL MONOGRAPH NO. 1 TECHNICAL MONOGRAPH NO. 2
STABILITY TESTING OF EXISTING PRIMARY & SECONDARY CHEMICAL
DRUGS SUBSTANCES AND PRODUCTS REFERENCE SUBSTANCES
TECHNICAL MONOGRAPH NO. 3 TECHNICAL MONOGRAPH NO. 4
INVESTIGATION OF OUT OF SPECIFICATION PHARMACEUTICAL PREFORMULATION
(OOS) TEST RESULTS ANALYTICAL STUDIES
TECHNICAL MONOGRAPH NO. 5 TECHNICAL MONOGRAPH NO. 6
ENVIRONMENTAL MONITORING CORRECTIVE/PREVENTIVE ACTIONS
IN CLEANROOMS (CAPA) GUIDELINE
TECHNICAL MONOGRAPH NO. 7 TECHNICAL DOCUMENT NO. 8
DATA INTEGRITY GOVERNANCE QUALITY 4.0 DIGITAL
TECHNOLOGY OF THE FUTURE
Copies are available at IDMA Office, Mumbai. We do not mail any publications against VPP payment.
All payments to be made in advance as Cheque/DD/RTGS/NEFT in favour of
“INDIAN DRUG MANUFACTURERS’ ASSOCIATION” at Mumbai.
For more details please contact: PUBLICATIONS DEPARTMENT Tel.: 022 - 2494 4624 / 2497 4308
E-mail: publications@idmaindia.com/actadm@idmaindia.com
Website: www.idma-assn.org/www.indiandrugsonline.org
INDIAN DRUGS 60 (05) MAY 2023 21
You might also like
- India, Article OriginalDocument18 pagesIndia, Article OriginalYan BejaranoNo ratings yet
- Sars-Cov-2 / Covid-19 and Its Transmission, Prevention, Treatment and Control - An UpdateDocument12 pagesSars-Cov-2 / Covid-19 and Its Transmission, Prevention, Treatment and Control - An UpdateMafalda ChoupinaNo ratings yet
- JMV 25766 PDFDocument19 pagesJMV 25766 PDFQfb Victor RobledoNo ratings yet
- The Cytokine Storm and COVID-19Document24 pagesThe Cytokine Storm and COVID-19gevowo3277No ratings yet
- COVID 19, An Emerging Coronavirus Infection CurrentDocument8 pagesCOVID 19, An Emerging Coronavirus Infection CurrentAsepNo ratings yet
- Corona Virus 19Document14 pagesCorona Virus 19مجد ابو القاسمNo ratings yet
- Coronavirus3 PDFDocument28 pagesCoronavirus3 PDFWilmar David Medina MadridNo ratings yet
- 2021 Virus Associated Ribozymes and Nano Carriers Against COVID 19Document16 pages2021 Virus Associated Ribozymes and Nano Carriers Against COVID 19muhammad neyaziNo ratings yet
- Corona Virus DiseaseDocument6 pagesCorona Virus DiseaseSAKET MEHTANo ratings yet
- Covid 19 A Dreaded Pandemic DiseaseDocument6 pagesCovid 19 A Dreaded Pandemic DiseasegygyNo ratings yet
- Highlights, Evaluation, and Treatment of Coronavirus (COVID-19)Document23 pagesHighlights, Evaluation, and Treatment of Coronavirus (COVID-19)Catchuela, JoannNo ratings yet
- International Journal of Antimicrobial AgentsDocument9 pagesInternational Journal of Antimicrobial AgentsautomationenggNo ratings yet
- Bab 2 Review Literatur: 2.1. Corona Virus Disease 2019 (COVID-19)Document21 pagesBab 2 Review Literatur: 2.1. Corona Virus Disease 2019 (COVID-19)Ali Zainal Enal ShahabNo ratings yet
- Pathogens: Sars-Cov-2 and Coronavirus Disease 2019: What We Know So FarDocument14 pagesPathogens: Sars-Cov-2 and Coronavirus Disease 2019: What We Know So FarBakir ŠiljakNo ratings yet
- Zhou2020 Article CoronavirusDisease2019COVID-19 PDFDocument10 pagesZhou2020 Article CoronavirusDisease2019COVID-19 PDFElena AlexandraNo ratings yet
- COVID-19 and Tuberculosis: HighlightDocument7 pagesCOVID-19 and Tuberculosis: HighlightMariaNo ratings yet
- JMB030-03-01 Fdoc 1Document12 pagesJMB030-03-01 Fdoc 1Bárbara Paranhos CoelhoNo ratings yet
- Sars-Cov-2: An Emerging Coronavirus That Causes A Global ThreatDocument8 pagesSars-Cov-2: An Emerging Coronavirus That Causes A Global ThreatIoana CucuNo ratings yet
- Comparative Review of Sars-Cov-2, Sars-Cov, Mers-Cov, and Influenza A Respiratory VirusesDocument14 pagesComparative Review of Sars-Cov-2, Sars-Cov, Mers-Cov, and Influenza A Respiratory Virusesfani rudiyantiNo ratings yet
- Journal - SARS in Geriatric - AlbertoDocument5 pagesJournal - SARS in Geriatric - AlbertoalbertoNo ratings yet
- COVID Status and Future PerspectivesDocument8 pagesCOVID Status and Future PerspectivesLuis BenitezNo ratings yet
- Article Epidemio Therapeutics Vaccines Covid PDFDocument12 pagesArticle Epidemio Therapeutics Vaccines Covid PDFAlexRázuriNo ratings yet
- Ageing Research ReviewsDocument11 pagesAgeing Research ReviewsLorena Morena Rosa MelchiorNo ratings yet
- The COVID-19 Pandemic: Critical Reviews in Clinical Laboratory SciencesDocument25 pagesThe COVID-19 Pandemic: Critical Reviews in Clinical Laboratory SciencesSir Ahmet AydınNo ratings yet
- Covide 19 BeginigDocument14 pagesCovide 19 BeginigHamza MehalliNo ratings yet
- Novel 2019 Coronavirus Structure, Mechanism of Action, Antiviral Drug Promises and Rule Out Against Its TreatmentDocument10 pagesNovel 2019 Coronavirus Structure, Mechanism of Action, Antiviral Drug Promises and Rule Out Against Its TreatmentZied TrikiNo ratings yet
- Velavan Et Al-2020-Tropical Medicine International HealthDocument4 pagesVelavan Et Al-2020-Tropical Medicine International Healthjunior rodriguesNo ratings yet
- Covid-19: Characteristics and TherapeuticsDocument29 pagesCovid-19: Characteristics and TherapeuticsHelenaNo ratings yet
- IPIntJComprAdvPharmacol 5-2-49 57Document9 pagesIPIntJComprAdvPharmacol 5-2-49 57jmakbar AkbarNo ratings yet
- The Pathophysiology of Virulence of The COVID-19Document31 pagesThe Pathophysiology of Virulence of The COVID-19Glaneisia MitchellNo ratings yet
- The Pathophysiology of Virulence of The COVID-19Document31 pagesThe Pathophysiology of Virulence of The COVID-19Vania ShaulaNo ratings yet
- Annals of PhytomedicineDocument9 pagesAnnals of PhytomedicinegygyNo ratings yet
- New ChallengeDocument3 pagesNew ChallengeEliana TorresNo ratings yet
- Patfis Covid 6Document6 pagesPatfis Covid 6mayaNo ratings yet
- Life Sciences: Rishabh Hirawat, Mohd Aslam Saifi, Chandraiah GoduguDocument14 pagesLife Sciences: Rishabh Hirawat, Mohd Aslam Saifi, Chandraiah GoduguPaoloMafaldoNo ratings yet
- JMV 9999 NaDocument9 pagesJMV 9999 Nafk unswagatiNo ratings yet
- An Update On COVID 19 Pandemic The Epidemiology Pathogenesis Prevention and Treatment Strategies (Important)Document13 pagesAn Update On COVID 19 Pandemic The Epidemiology Pathogenesis Prevention and Treatment Strategies (Important)ayoubNo ratings yet
- JCMM 24 6558Document13 pagesJCMM 24 6558Roberto D. GarceteNo ratings yet
- Ajmr 8 2 3Document6 pagesAjmr 8 2 3Ahasan Ullah KhanNo ratings yet
- Covid-19 - A Pandemic by Sars-Cov-2: Harsh R Darji (J18Imt601)Document3 pagesCovid-19 - A Pandemic by Sars-Cov-2: Harsh R Darji (J18Imt601)Harsh Darji100% (1)
- COVID-19 and Diabetes MellitusDocument6 pagesCOVID-19 and Diabetes MellitusUlysses GamayonNo ratings yet
- Life 12 01245Document11 pagesLife 12 01245mol3cul4RNANo ratings yet
- A Perspective About Coronavirus Disease 2019 (COVID-19) : Review ArticleDocument21 pagesA Perspective About Coronavirus Disease 2019 (COVID-19) : Review ArticleWarner LlaveNo ratings yet
- CovidnewDocument11 pagesCovidnewJoy Chakraborty RoniNo ratings yet
- TRADUCCION (1) 1 - The COVID-19 Epidemic PDFDocument3 pagesTRADUCCION (1) 1 - The COVID-19 Epidemic PDFSikamelNo ratings yet
- Covid19 PDFDocument40 pagesCovid19 PDFMan Hong SoNo ratings yet
- Emj 99836 Invited - Review OzdemirDocument6 pagesEmj 99836 Invited - Review Ozdemirdayuseed001No ratings yet
- Coronavirus Disease 2019 (COVID-19) - UpToDateDocument43 pagesCoronavirus Disease 2019 (COVID-19) - UpToDateGloria MiramontesNo ratings yet
- A Review of Sars-Cov-2 and The Ongoing Clinical Trials: Molecular SciencesDocument19 pagesA Review of Sars-Cov-2 and The Ongoing Clinical Trials: Molecular SciencesJoseGarciaNo ratings yet
- Decoding Covid-19 With The Sars-Cov-2 GenomeDocument12 pagesDecoding Covid-19 With The Sars-Cov-2 GenomemmNo ratings yet
- Waste 4Document6 pagesWaste 4Sajin AlexanderNo ratings yet
- International Journal of Antimicrobial Agents: Heng Li, Shang-Ming Liu, Xiao-Hua Yu, Shi-Lin Tang, Chao-Ke TangDocument8 pagesInternational Journal of Antimicrobial Agents: Heng Li, Shang-Ming Liu, Xiao-Hua Yu, Shi-Lin Tang, Chao-Ke TangKenia FrnNo ratings yet
- Human and Novel Coronavirus Infections in Children: A ReviewDocument21 pagesHuman and Novel Coronavirus Infections in Children: A ReviewWilmer UcedaNo ratings yet
- COVID-19 and Multiorgan ResponsDocument21 pagesCOVID-19 and Multiorgan ResponssamuelNo ratings yet
- Banerjee 2021Document15 pagesBanerjee 2021georgeNo ratings yet
- Reviews: Characteristics of Sars-Cov-2 and Covid-19Document14 pagesReviews: Characteristics of Sars-Cov-2 and Covid-19Ioana CoseruNo ratings yet
- Facing COVID-19 with the benefits of medical cannabisFrom EverandFacing COVID-19 with the benefits of medical cannabisNo ratings yet
- Ah102 Syllabus 20180417Document7 pagesAh102 Syllabus 20180417api-410716618No ratings yet
- Nursing InformaticsDocument28 pagesNursing Informaticsd1choosenNo ratings yet
- An Assessment of Manual Medical Record System of Fr. Simpliciano Academy Inc. School Year 2018-2019Document66 pagesAn Assessment of Manual Medical Record System of Fr. Simpliciano Academy Inc. School Year 2018-2019Dimple SalesNo ratings yet
- Research EssayDocument12 pagesResearch Essayapi-608972617No ratings yet
- Future Challenges and Objectives For Pda in Asiapac: Connecting People, Science and RegulationDocument11 pagesFuture Challenges and Objectives For Pda in Asiapac: Connecting People, Science and RegulationhuykhiemNo ratings yet
- Academic Record Cgfns PDFDocument2 pagesAcademic Record Cgfns PDFSdgfh Wanda100% (1)
- Caring For A Sick Elder PPDocument19 pagesCaring For A Sick Elder PPKAMILAH EDUARDONo ratings yet
- Roxas Memorial Provincial HospitalDocument11 pagesRoxas Memorial Provincial HospitalJuvie Lie Fancubila FerrenNo ratings yet
- Implementation of A Community-Based Exercise Program For Parkinson Patients: Using Boxing As An ExampleDocument10 pagesImplementation of A Community-Based Exercise Program For Parkinson Patients: Using Boxing As An Examplesunardi irwaniNo ratings yet
- Recording and Reporting Based On FHSISDocument40 pagesRecording and Reporting Based On FHSISAnonymous h2EnKyDbNo ratings yet
- The Impact of The COVID 19 Pandemic On Low Income Households in The Philippines Impending Human Capital CrisisDocument20 pagesThe Impact of The COVID 19 Pandemic On Low Income Households in The Philippines Impending Human Capital CrisisKim DumaganNo ratings yet
- Group 4Document19 pagesGroup 4SAGARGAONKAR386079No ratings yet
- DAFTAR PUSTAKA SiapDocument3 pagesDAFTAR PUSTAKA SiapRatria Andika PutraNo ratings yet
- TIGER Initiative Informatics DefinitionsDocument9 pagesTIGER Initiative Informatics DefinitionslaggantigganNo ratings yet
- 1 +Bharath+Biotech+PPTDocument20 pages1 +Bharath+Biotech+PPTTapan SharmaNo ratings yet
- Update in Anaesthesia PDFDocument64 pagesUpdate in Anaesthesia PDFShabih RazaNo ratings yet
- Guidebook For Preacc Entrylevelstandards SHCO PDFDocument162 pagesGuidebook For Preacc Entrylevelstandards SHCO PDFArun Kumar100% (3)
- Physiotherapy Practice in Stroke Rehabilitation: A Cross-Sectional Survey of Physiotherapists in The State of Kerala, IndiaDocument7 pagesPhysiotherapy Practice in Stroke Rehabilitation: A Cross-Sectional Survey of Physiotherapists in The State of Kerala, IndiaRithika JananiNo ratings yet
- Emergency Obstetric and Newborn CareDocument4 pagesEmergency Obstetric and Newborn CaremnmrznNo ratings yet
- A Comparison of Conventional and New Rubber Dam Systems in Dental PracticeDocument8 pagesA Comparison of Conventional and New Rubber Dam Systems in Dental PracticeShinta PurnamasariNo ratings yet
- List Jurnal Scopus - Public Health, Environmental and Occupational HealthDocument41 pagesList Jurnal Scopus - Public Health, Environmental and Occupational HealthindiraDLNo ratings yet
- 2019 Spena and Cristina Practising Innovation in The Healthcare EcosystemDocument14 pages2019 Spena and Cristina Practising Innovation in The Healthcare Ecosystemwihaga satya khresnaNo ratings yet
- 130300-Standards For Acute and Critical Care NursingDocument12 pages130300-Standards For Acute and Critical Care Nursingapi-315277523No ratings yet
- Melanoma Pathology Reporting and StagingDocument10 pagesMelanoma Pathology Reporting and StagingLizbeth QuinteroNo ratings yet
- Daftar PustakaDocument3 pagesDaftar PustakaPrama GitaNo ratings yet
- Jonas Salk BiographyDocument3 pagesJonas Salk BiographyhapsNo ratings yet
- The Deadly Impossibility of Herd Immunity Through Vaccination by DR Russell BlaylockDocument3 pagesThe Deadly Impossibility of Herd Immunity Through Vaccination by DR Russell BlaylockAsimuddin68No ratings yet
- Tranaxemic AcidDocument6 pagesTranaxemic AcidCharan Teja ReddyNo ratings yet
- Eating Disorders in Male and Female AthletesDocument4 pagesEating Disorders in Male and Female AthletesmartinNo ratings yet
- Family Life Cycle Stage Major Task 2 Order Changes in Family Status Required To Proceed DevelopmentallyDocument6 pagesFamily Life Cycle Stage Major Task 2 Order Changes in Family Status Required To Proceed DevelopmentallyAris Jasper NacionNo ratings yet