You might also like
- Road ConstructionDocument100 pagesRoad ConstructionStalyn Zuñiga100% (1)
- Abdominal TraumaDocument60 pagesAbdominal Traumamel_chakNo ratings yet
- Acute Abdominal Pain: Presented by Dr. Kolahdouzan Thoracic Surgen Alzahra HospitalDocument77 pagesAcute Abdominal Pain: Presented by Dr. Kolahdouzan Thoracic Surgen Alzahra HospitalGraceline Margaretha Marsintauly SianiparNo ratings yet
- Acute Abdominal Pain 2Document72 pagesAcute Abdominal Pain 2ngockhanh1971No ratings yet
- UT Trauma HandbookDocument49 pagesUT Trauma Handbooksgod34No ratings yet
- Abdominal TraumaDocument60 pagesAbdominal Traumaapi-19916399No ratings yet
- History of Madre de DiosDocument3 pagesHistory of Madre de DiosMisterJanNo ratings yet
- First Responder ManualDocument69 pagesFirst Responder ManualCristina Joy Vicente Cruz100% (3)
- Classical Disc Herniation by DR Anupreet BassiDocument17 pagesClassical Disc Herniation by DR Anupreet Bassidr_bassiNo ratings yet
- Low BackDocument7 pagesLow BackMuhammad FahmyNo ratings yet
- The Radiology Handbook: A Pocket Guide to Medical ImagingFrom EverandThe Radiology Handbook: A Pocket Guide to Medical ImagingRating: 3.5 out of 5 stars3.5/5 (8)
- How To Take HistoryDocument59 pagesHow To Take HistoryBelalNo ratings yet
- Abdominal Trauma - 0Document129 pagesAbdominal Trauma - 0Tan DanNo ratings yet
- Differential Diagnosis of Back PainDocument26 pagesDifferential Diagnosis of Back PainKristy Besarab100% (1)
- Cae Grammar TensesDocument4 pagesCae Grammar TensesYana MarinkovaNo ratings yet
- Nanotechnology in Civil EngineeringDocument22 pagesNanotechnology in Civil EngineeringNehad AhmedNo ratings yet
- 6 - Pediatric Disorders - Rosales (P2) - AfssstDocument11 pages6 - Pediatric Disorders - Rosales (P2) - AfssstFranz Earl Niño AlbesaNo ratings yet
- Ghost Hawk ExcerptDocument48 pagesGhost Hawk ExcerptSimon and SchusterNo ratings yet
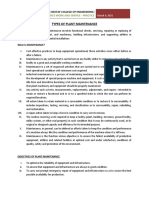
- Types of Plant MaintenanceDocument7 pagesTypes of Plant MaintenanceTHEOPHILUS ATO FLETCHERNo ratings yet
- Family Medicine DepartmentDocument45 pagesFamily Medicine Departmentسليمان فايزNo ratings yet
- Abdomen Blunt Trauma 2 - 3 - 2020Document6 pagesAbdomen Blunt Trauma 2 - 3 - 2020Iqra NazNo ratings yet
- 2 Acute Shoulder Pain Diagnosis and ManagementDocument42 pages2 Acute Shoulder Pain Diagnosis and Managementmk78_inNo ratings yet
- Gastrointestinal Alterations (Class 8)Document38 pagesGastrointestinal Alterations (Class 8)Danial HassanNo ratings yet
- Acute Coronary SyndromeDocument36 pagesAcute Coronary SyndromeSiti FatimahNo ratings yet
- PY6030 Term 1Document13 pagesPY6030 Term 1AlexaJoiceJumao-AsNo ratings yet
- Evaluation of Abdominal Pain in The Emergency DepartmentDocument11 pagesEvaluation of Abdominal Pain in The Emergency DepartmentUshnish ChatterjeeNo ratings yet
- Acute Coronary SyndromeDocument27 pagesAcute Coronary SyndromeHassan MuhammadNo ratings yet
- (NS) Week 11 SBL Fractures QuestionsDocument16 pages(NS) Week 11 SBL Fractures QuestionsJoei “Jojo” GohNo ratings yet
- Low Back Pain: Management Update: DR Dewanta Sembiring, SpsDocument46 pagesLow Back Pain: Management Update: DR Dewanta Sembiring, SpsYoke RetnaningpuriNo ratings yet
- Spinal Cord Injury: Andi IhwanDocument31 pagesSpinal Cord Injury: Andi IhwanAndi Muliana SultaniNo ratings yet
- Schuster AthleticPelvisDocument26 pagesSchuster AthleticPelvisTheScribbl3rNo ratings yet
- Abdominal TraumaDocument41 pagesAbdominal TraumaAhmad Shafwan NatsirNo ratings yet
- Nurul Qalby C111 13 064 A. Anisa Nasir C111 13 082 Sitti Magfirah Adnan C111 13 090Document32 pagesNurul Qalby C111 13 064 A. Anisa Nasir C111 13 082 Sitti Magfirah Adnan C111 13 090Nurul Qalby AmiluddinNo ratings yet
- Exercise Prescription Basics: Kevin Deweber, MD, Faafp Director, Primary Care Sports Medicine Fellowship UsuhsDocument33 pagesExercise Prescription Basics: Kevin Deweber, MD, Faafp Director, Primary Care Sports Medicine Fellowship UsuhsnarayankhurdeNo ratings yet
- The Role of USG in ED (Ali Haedar)Document27 pagesThe Role of USG in ED (Ali Haedar)Bayu AkbarNo ratings yet
- Case StudyDocument6 pagesCase StudyMurad KurdiNo ratings yet
- Nurul Hudayani C 111 06 100 Supervisor Dr. Muh. Andry Usman, SP - OTDocument14 pagesNurul Hudayani C 111 06 100 Supervisor Dr. Muh. Andry Usman, SP - OTamel015No ratings yet
- Initial Management in Musculoskeletal Trauma: Yoyos D. IsmiartoDocument40 pagesInitial Management in Musculoskeletal Trauma: Yoyos D. IsmiartozaroziNo ratings yet
- Abdominal TraumaDocument6 pagesAbdominal TraumaIlyes FerenczNo ratings yet
- Back Pain: Group 4Document71 pagesBack Pain: Group 4Cesar Guico Jr.No ratings yet
- Chest Pain DDDocument79 pagesChest Pain DDkashmala afzalNo ratings yet
- Intro To Ped Radiology - Ped Rad Fellow - MahmoodDocument58 pagesIntro To Ped Radiology - Ped Rad Fellow - MahmoodKelvin ZhouNo ratings yet
- RheumatologyDocument21 pagesRheumatologycksingh873808No ratings yet
- Closed Comminutive Fracture Middle Left Clavicle Allman Classification Group IDocument32 pagesClosed Comminutive Fracture Middle Left Clavicle Allman Classification Group IWilliamtatokieesz Tembokrumahampebenjol-benjolNo ratings yet
- Oa Case ReportDocument26 pagesOa Case Reportaliffikri52100% (1)
- Acute Low Back Pain: University of Michigan Guidelines For Health System Clinical CareDocument14 pagesAcute Low Back Pain: University of Michigan Guidelines For Health System Clinical CareMohamed KassimNo ratings yet
- Chest PainDocument30 pagesChest PainLamya ZamanNo ratings yet
- مرض السكرDocument17 pagesمرض السكرgadert2020No ratings yet
- Internal Organ InjuriesDocument57 pagesInternal Organ InjuriesHANIFF FAIZAL BIN CHEK ANI CHEK ANI IPG KDANo ratings yet
- Abdominal Trauma: Ghidirim GH., Mishin I., Zastavnitsky GH., Vozian MDocument129 pagesAbdominal Trauma: Ghidirim GH., Mishin I., Zastavnitsky GH., Vozian MBedah MalangNo ratings yet
- This Study Resource Was: Assessment & Reasoning Cardiac SystemDocument6 pagesThis Study Resource Was: Assessment & Reasoning Cardiac SystemSharon TanveerNo ratings yet
- Single Jejunal Blowout Perforation Following Blunt Abdominal Trauma: Diagnostic DilemmaDocument3 pagesSingle Jejunal Blowout Perforation Following Blunt Abdominal Trauma: Diagnostic DilemmapricillyaNo ratings yet
- Scribe America Final, Emergency DepartmentDocument41 pagesScribe America Final, Emergency DepartmentJulio CastilloNo ratings yet
- Lyceum-Northwestern University College of Medicine Medicine 1 - Clinical Workshop 1 Topic-Back Pain Group-1Document9 pagesLyceum-Northwestern University College of Medicine Medicine 1 - Clinical Workshop 1 Topic-Back Pain Group-1Sachin KpNo ratings yet
- 1.1 Evaluación Clínica en Padecimientos VascularesDocument31 pages1.1 Evaluación Clínica en Padecimientos VascularesMarisolCamposNo ratings yet
- Acute Coronary Syndrome: PGI Calro Antonio H. Lanuza Manila Doctors Hospital - Internal Medicine DepartmentDocument60 pagesAcute Coronary Syndrome: PGI Calro Antonio H. Lanuza Manila Doctors Hospital - Internal Medicine DepartmentCarlo LanuzaNo ratings yet
- PANCREATITISDocument11 pagesPANCREATITISLuis Morales CotaNo ratings yet
- Total Knee Replacement: Done By: Sajeda Moha'dDocument27 pagesTotal Knee Replacement: Done By: Sajeda Moha'dlolo223No ratings yet
- Advance Trauma Life Support: Andi Siswandi, MD Surgeon Malahayati University, Medicine FacultyDocument76 pagesAdvance Trauma Life Support: Andi Siswandi, MD Surgeon Malahayati University, Medicine Facultyhari dorismanNo ratings yet
- Tho A Co Abdominal Injuries ChapterDocument26 pagesTho A Co Abdominal Injuries ChapteroajaisjsNo ratings yet
- Understanding Athletic Pubalgia: A ReviewDocument5 pagesUnderstanding Athletic Pubalgia: A ReviewMikeNo ratings yet
- Abdominal Aortic AneurysmDocument1 pageAbdominal Aortic Aneurysmdragtoss2No ratings yet
- Abdominal InjuriesDocument3 pagesAbdominal InjuriesNeha SarfrazNo ratings yet
- Clinical Decision Making To Determine Need For Medical ReferralDocument12 pagesClinical Decision Making To Determine Need For Medical ReferralaroobaNo ratings yet
- Jama 268 6 030Document6 pagesJama 268 6 030Thiago Scharth MontenegroNo ratings yet
- Abdominal Pain: Essential Diagnosis and Management in Acute MedicineFrom EverandAbdominal Pain: Essential Diagnosis and Management in Acute MedicineNo ratings yet
- BW650 InstallDocument7 pagesBW650 InstallfreekenzoNo ratings yet
- PD2017 013 PDFDocument36 pagesPD2017 013 PDFChico Hermanu BrillianNo ratings yet
- Week 5 Reading TextsDocument3 pagesWeek 5 Reading Textskerem ozan emirNo ratings yet
- Pointy Hat - The Cowboy - Ranger ConclaveDocument5 pagesPointy Hat - The Cowboy - Ranger Conclave678ojyhiopNo ratings yet
- Latihan Soal Dan Evaluasi Materi ComplimentDocument6 pagesLatihan Soal Dan Evaluasi Materi ComplimentAvildaAfrinAmmaraNo ratings yet
- 0000 Mathematica at WWUDocument11 pages0000 Mathematica at WWUWilhelm Richard WagnerNo ratings yet
- Bank of South Sudan Act, 2011 - Bank of South SudanDocument59 pagesBank of South Sudan Act, 2011 - Bank of South SudanAnnadevaraNageswararaoNo ratings yet
- Unit 19-20Document10 pagesUnit 19-20Wulan AnggreaniNo ratings yet
- Profit Loss Account TemplateDocument4 pagesProfit Loss Account TemplatesnehaNo ratings yet
- COMMUNICABLEDocument6 pagesCOMMUNICABLEAngeline TaghapNo ratings yet
- Communityhealth 141122094330 Conversion Gate02Document22 pagesCommunityhealth 141122094330 Conversion Gate02Titser JoNo ratings yet
- Unit 1 Hello There!: PAG E Lesson Vocabulary Grammar Listening Track: UNIT 1Document10 pagesUnit 1 Hello There!: PAG E Lesson Vocabulary Grammar Listening Track: UNIT 1Analia SanlongNo ratings yet
- Second SundayDocument6 pagesSecond SundayAlfred LochanNo ratings yet
- E8 Practice Test Second Term Grade 8 - 962023103557Document13 pagesE8 Practice Test Second Term Grade 8 - 962023103557Duy HoangNo ratings yet
- Comp2-Cause-Effect EssayDocument4 pagesComp2-Cause-Effect Essayapi-316060728No ratings yet
- NCM 109 SKILLS LAB DAY 1 Laboratory and Diagnostics22Document55 pagesNCM 109 SKILLS LAB DAY 1 Laboratory and Diagnostics22Joseph DusichNo ratings yet
- Timeline of My Exposure To Traditional and New Media - Justine Sheen Gay-12 ABM-BDocument16 pagesTimeline of My Exposure To Traditional and New Media - Justine Sheen Gay-12 ABM-Bapi-389627320No ratings yet
- Kerala University PHD Course Work Exam SyllabusDocument4 pagesKerala University PHD Course Work Exam Syllabuslozuzimobow3100% (2)
- 2019 Admax CataDocument30 pages2019 Admax CataEVENTIA AFRICANo ratings yet
- Potter's House Christian FellowshipDocument12 pagesPotter's House Christian Fellowshipwattssteve21No ratings yet
- 13 Datasheet Chint Power Cps Sca5ktl-Psm1-EuDocument1 page13 Datasheet Chint Power Cps Sca5ktl-Psm1-EuMARCOS DANILO DE ALMEIDA LEITENo ratings yet
- Vibration Control Technology Industry (Freudenberg Schwab)Document111 pagesVibration Control Technology Industry (Freudenberg Schwab)ismailNo ratings yet
- ObliCon Reviewer SMDocument111 pagesObliCon Reviewer SMJessa Marie BrocoyNo ratings yet