You might also like
- Human Challenge Studies To Accelerate Coronavirus Vaccine LicensureDocument5 pagesHuman Challenge Studies To Accelerate Coronavirus Vaccine LicensurePablo Segales BautistaNo ratings yet
- Vaccine Development, Testing, and RegulationDocument12 pagesVaccine Development, Testing, and RegulationP Bijoya SinghaNo ratings yet
- Vaccine Against Covid-19 Disease - Present Status of DevelopmentDocument7 pagesVaccine Against Covid-19 Disease - Present Status of DevelopmenthayyatNo ratings yet
- Vaccine Epidemiology Efficacy EffectivenessDocument5 pagesVaccine Epidemiology Efficacy EffectivenessCesar Augusto Hernandez GualdronNo ratings yet
- Epid 2Document4 pagesEpid 2lakshanNo ratings yet
- Entendiendo La Eficacia de Covi19Document5 pagesEntendiendo La Eficacia de Covi19Johan EspinozaNo ratings yet
- Epid 1Document4 pagesEpid 1lakshanNo ratings yet
- COVID-19 Vaccine Surveillance Report: Week 1Document54 pagesCOVID-19 Vaccine Surveillance Report: Week 1camaferNo ratings yet
- U D C C E: Niversity of Haka Pplied Hemistry and Hemical NgineeringDocument6 pagesU D C C E: Niversity of Haka Pplied Hemistry and Hemical NgineeringMD: Shamim HossainNo ratings yet
- 4 PDFDocument18 pages4 PDFMinh TranNo ratings yet
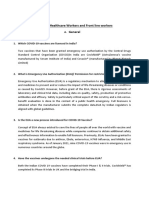
- Faqs For Healthcare Workers and Front Line Workers GeneralDocument12 pagesFaqs For Healthcare Workers and Front Line Workers GeneraltejaNo ratings yet
- Cancer4less Research Paper Ishmita VaishDocument2 pagesCancer4less Research Paper Ishmita Vaishvaishjia23No ratings yet
- Corona Virus ResearchDocument3 pagesCorona Virus ResearchJomark PalganNo ratings yet
- Past SARS-CoV-2 Infection Protection Against Re-InfectionDocument10 pagesPast SARS-CoV-2 Infection Protection Against Re-InfectionRoel PlmrsNo ratings yet
- COVID-19 Vaccine Surveillance Report: Week 2Document55 pagesCOVID-19 Vaccine Surveillance Report: Week 2Kosta GavrasNo ratings yet
- Biology Project 88Document11 pagesBiology Project 88Ayush SinghNo ratings yet
- COVID-19 Vaccine Development - Milestones, Lessons and ProspectsDocument32 pagesCOVID-19 Vaccine Development - Milestones, Lessons and Prospectsnadhia rahdaNo ratings yet
- UKHSA Vaccine Surveillance Report Week 48Document47 pagesUKHSA Vaccine Surveillance Report Week 48Al StatiliusNo ratings yet
- VaccinesDocument4 pagesVaccinesSrikant SinghNo ratings yet
- MCB301 Vaccine DevelopmentDocument3 pagesMCB301 Vaccine DevelopmentUsman SurajNo ratings yet
- Technological Approaches To Streamline Vaccination Schedules, Progressing Towards Single-Dose VaccinesDocument13 pagesTechnological Approaches To Streamline Vaccination Schedules, Progressing Towards Single-Dose VaccinesM OrganicNo ratings yet
- Covid-19: Vaccines To Prevent Sars-Cov-2 Infection: AuthorsDocument42 pagesCovid-19: Vaccines To Prevent Sars-Cov-2 Infection: AuthorsMarcela GarciaNo ratings yet
- The Need For Another Typhoid Fever Vaccine: EditorialcommentaryDocument3 pagesThe Need For Another Typhoid Fever Vaccine: Editorialcommentaryshelly_shellyNo ratings yet
- Logical Division of Ideas OutlineDocument6 pagesLogical Division of Ideas OutlineBrahian SarmientoNo ratings yet
- Vaccine Surveillance Report - Week 37 v2Document33 pagesVaccine Surveillance Report - Week 37 v2Abby EscorzaNo ratings yet
- Government 211016 134210Document27 pagesGovernment 211016 134210KemNo ratings yet
- VACCINES Boosters - EDITEDFINAL 110321Document35 pagesVACCINES Boosters - EDITEDFINAL 110321Sherre Nicole CuentaNo ratings yet
- 1 s2.0 S095279152100090X MainDocument6 pages1 s2.0 S095279152100090X MainNunungTriwahyuniNo ratings yet
- How Do Vaccines WorkDocument5 pagesHow Do Vaccines WorkImaan KhanNo ratings yet
- A Strategic Approach To COVID-19 Vaccine R&D: Lawrence Corey, John R. Mascola, Anthony S. Fauci, Francis S. CollinsDocument6 pagesA Strategic Approach To COVID-19 Vaccine R&D: Lawrence Corey, John R. Mascola, Anthony S. Fauci, Francis S. CollinsGrace AngelinaNo ratings yet
- COVID-19 Vaccine Surveillance Report: Week 51Document53 pagesCOVID-19 Vaccine Surveillance Report: Week 51RicardoNo ratings yet
- 1-S2.0-S1044532320300385-Sars Cov VaccineDocument16 pages1-S2.0-S1044532320300385-Sars Cov VaccineSIUSANTO HadiNo ratings yet
- Why Should You Be Vaccinated?: Nicolás Steven Peña Gómez Juan Camilo Rojas Hernández Juan Sebastián Estupiñán PintoDocument9 pagesWhy Should You Be Vaccinated?: Nicolás Steven Peña Gómez Juan Camilo Rojas Hernández Juan Sebastián Estupiñán PintoELNo ratings yet
- UK Vaccine Surveillance Report Week 42Document29 pagesUK Vaccine Surveillance Report Week 42Cam SlaterNo ratings yet
- CholeraDocument7 pagesCholeraDewa Ayu Pradnya DewiNo ratings yet
- A Study On Seroconversion Following First Second.9Document6 pagesA Study On Seroconversion Following First Second.9Darshan GandhiNo ratings yet
- Boosting Immunity To COVID-19 Vaccines: News & ViewsDocument2 pagesBoosting Immunity To COVID-19 Vaccines: News & Viewsbernardo broccaNo ratings yet
- Cost Utility of Vaccination Against COVID-19 in BrazilDocument8 pagesCost Utility of Vaccination Against COVID-19 in BrazilTatiana DutraNo ratings yet
- Topic: The (Covid-19) Vaccine Process. Purpose: To Inform Audience: The Class Tone: FormalDocument8 pagesTopic: The (Covid-19) Vaccine Process. Purpose: To Inform Audience: The Class Tone: FormalBrahian SarmientoNo ratings yet
- Journal of Infectious DiseaseDocument6 pagesJournal of Infectious DiseaseSoham SarangiNo ratings yet
- Piis258953702200061x PDFDocument11 pagesPiis258953702200061x PDFRong LiuNo ratings yet
- The Optimal Strategy For Pertussis Vaccination: A Systematic Review and Meta-Analysis of Randomized Control Trials and Real-World DataDocument26 pagesThe Optimal Strategy For Pertussis Vaccination: A Systematic Review and Meta-Analysis of Randomized Control Trials and Real-World DataIdmNo ratings yet
- The Different Types of COVID-19 VaccinesDocument4 pagesThe Different Types of COVID-19 VaccinesSusanty NazmiNo ratings yet
- Mourtzoukou Et Al-2008-British Journal of SurgeryDocument8 pagesMourtzoukou Et Al-2008-British Journal of SurgeryTony AdeosunNo ratings yet
- Novel VaccineDocument16 pagesNovel Vaccineparam540No ratings yet
- COVAXINDocument3 pagesCOVAXINRakshit VermaNo ratings yet
- Personal ViewDocument11 pagesPersonal ViewruthchristinawibowoNo ratings yet
- Trial of BCG Vaccines in South India For Tuberculosis Prevention: First ReportDocument9 pagesTrial of BCG Vaccines in South India For Tuberculosis Prevention: First ReportMarisa LisnawatiNo ratings yet
- Efficacy and Safety of A RecombinantDocument13 pagesEfficacy and Safety of A RecombinantSofyanNo ratings yet
- Abaclinicaltrialofvaccine 181119065907Document34 pagesAbaclinicaltrialofvaccine 181119065907vũ đình dũngNo ratings yet
- 1 s2.0 S0169409X2030065X MainDocument55 pages1 s2.0 S0169409X2030065X MainLixia WeiNo ratings yet
- WHO 2019 NCoV Vaccines SAGE Recommendation Sinovac CoronaVac 2021.1 EngDocument7 pagesWHO 2019 NCoV Vaccines SAGE Recommendation Sinovac CoronaVac 2021.1 EngMartha Gatica GuevaraNo ratings yet
- Immunizaton During PregnancyDocument6 pagesImmunizaton During PregnancyMohamed SulimanNo ratings yet
- Mamalumpong Jordan A. Bsn-Iii Assignment: Date Published: November 6, 2020 Source: The Francis Crick InstituteDocument2 pagesMamalumpong Jordan A. Bsn-Iii Assignment: Date Published: November 6, 2020 Source: The Francis Crick InstituteJordan Abosama MamalumpongNo ratings yet
- Evaluation and Prevention of Infections Associated With Biologic Agents and JAK Inhibitors in Adults - UpToDateDocument76 pagesEvaluation and Prevention of Infections Associated With Biologic Agents and JAK Inhibitors in Adults - UpToDatemayteveronica1000No ratings yet
- Vaccine SafetyDocument14 pagesVaccine Safetychandru sahanaNo ratings yet
- Nej Mo A 1706804Document12 pagesNej Mo A 1706804rizki agusmaiNo ratings yet
- Post Covid ImmunityDocument2 pagesPost Covid ImmunityIheb LouetiNo ratings yet
- Infectious Diseases in Solid-Organ Transplant Recipients: A practical approachFrom EverandInfectious Diseases in Solid-Organ Transplant Recipients: A practical approachOriol ManuelNo ratings yet
- Influenza vaccination: What does the scientific proof say?: Could it be more harmful than useful to vaccinate indiscriminately elderly people, pregnant women, children and health workers?From EverandInfluenza vaccination: What does the scientific proof say?: Could it be more harmful than useful to vaccinate indiscriminately elderly people, pregnant women, children and health workers?No ratings yet
- Pts 1 Klas XI 2022 (Print)Document11 pagesPts 1 Klas XI 2022 (Print)WoldiaNo ratings yet
- AnumwraDocument30 pagesAnumwratejasNo ratings yet
- Cancer-Relatedfatiguein Cancersurvivorship: Chidinma C. Ebede,, Yongchang Jang,, Carmen P. EscalanteDocument13 pagesCancer-Relatedfatiguein Cancersurvivorship: Chidinma C. Ebede,, Yongchang Jang,, Carmen P. EscalanteMahdhun ShiddiqNo ratings yet
- Country/Airport City Laboratory: AfghanistanDocument22 pagesCountry/Airport City Laboratory: AfghanistanAliNo ratings yet
- GayDocument15 pagesGayjulyerwanni100% (2)
- With Conviction: Moving AheadDocument155 pagesWith Conviction: Moving Aheadkapadia krunalNo ratings yet
- ICNCDRS Blindness Registry FormDocument4 pagesICNCDRS Blindness Registry FormAprilAngeliRobleNo ratings yet
- Peplu Theory ApplicationDocument7 pagesPeplu Theory ApplicationVarsha Gurung100% (1)
- Murli Deora v. Union of India (Banning of Smoking in Public Places)Document2 pagesMurli Deora v. Union of India (Banning of Smoking in Public Places)Prerna SinghNo ratings yet
- Book Review Contemporary Public Administration (2021) PDFDocument119 pagesBook Review Contemporary Public Administration (2021) PDFTiyas Vika WidyastutiNo ratings yet
- AsthmaDocument10 pagesAsthmaAcohCChaoNo ratings yet
- MSDS STA Neoplastine CI PlusDocument8 pagesMSDS STA Neoplastine CI Plusasmaul husnahNo ratings yet
- Addis Ababa Science and Technology University (AASTU)Document24 pagesAddis Ababa Science and Technology University (AASTU)Wasihun DanielNo ratings yet
- Foundations For Clinical Mental Health Counseling - 3rd EditionDocument369 pagesFoundations For Clinical Mental Health Counseling - 3rd EditionJamie Finotti100% (7)
- Jamie's Story 15q21.3-22.2 DeletionDocument1 pageJamie's Story 15q21.3-22.2 DeletionNatasha RadcliffeNo ratings yet
- What Is The Four Hand Massage?: Enhanced RelaxationDocument3 pagesWhat Is The Four Hand Massage?: Enhanced RelaxationKomal MaqsoodNo ratings yet
- Important Weekly Current Affairs PDF 9 To 16 October: Date Important Days ThemeDocument10 pagesImportant Weekly Current Affairs PDF 9 To 16 October: Date Important Days ThemekavipriyaNo ratings yet
- Applying 5S ProceduresDocument70 pagesApplying 5S ProceduresSanta Best100% (3)
- InterbarkadaDocument8 pagesInterbarkadaJay Vincent DiamanteNo ratings yet
- Skripsi Tanpa Pembahasan PDFDocument73 pagesSkripsi Tanpa Pembahasan PDFMutmainnah MunirNo ratings yet
- Capa SopDocument23 pagesCapa SopHaroon Rasheed100% (3)
- 2 BiotechnologyDocument5 pages2 BiotechnologyJannah BuenavistaNo ratings yet
- Surgical Handicraft Manual For Surgical Residents 2015 PDFDocument295 pagesSurgical Handicraft Manual For Surgical Residents 2015 PDFNamerahN100% (3)
- HPA 14 Assignemnt Due November 16thDocument5 pagesHPA 14 Assignemnt Due November 16thcNo ratings yet
- LCSW Additional CourseworkDocument8 pagesLCSW Additional Courseworkiuhvgsvcf100% (2)
- BinderDocument13 pagesBinderisabel carreauNo ratings yet
- Psychiatry An Evidence Based Text PDFDocument1,336 pagesPsychiatry An Evidence Based Text PDFOscar Ayala100% (1)
- Purpose 1Document4 pagesPurpose 1Rizzah MagnoNo ratings yet
- Job Safety Analysis: Date/ Jsa No: Jsa Team Members Job: Location: Project/ Client: SupervisorDocument1 pageJob Safety Analysis: Date/ Jsa No: Jsa Team Members Job: Location: Project/ Client: SupervisorMuhammad Akbar Al BardawiNo ratings yet
- FPCurriculum OnlineDocument166 pagesFPCurriculum OnlineMulugeta DagneNo ratings yet