You might also like
- Surgical Instruments SlidesDocument142 pagesSurgical Instruments SlidesGil Platon Soriano100% (2)
- Carpal Tunnel Syndrome ExercisesDocument2 pagesCarpal Tunnel Syndrome ExercisesIgor GjorgjievNo ratings yet
- Articulo Ingles de ENFILADODocument6 pagesArticulo Ingles de ENFILADOruthy arias anahuaNo ratings yet
- Radiological Examination of ScoliosisDocument18 pagesRadiological Examination of ScoliosisFatenNo ratings yet
- Physical Examination ScoliosisDocument7 pagesPhysical Examination Scoliosisyosua_edwinNo ratings yet
- Skoliosis 1 PDFDocument7 pagesSkoliosis 1 PDFMr. wNo ratings yet
- Effects of Traditional vs. Dynamic Bracing On Scoliotic CurvesDocument13 pagesEffects of Traditional vs. Dynamic Bracing On Scoliotic Curvesalfman05302001No ratings yet
- ScoliosisDocument11 pagesScoliosisFatenNo ratings yet
- Measurement of Scoliosis Cobb Angle by End VertebrDocument7 pagesMeasurement of Scoliosis Cobb Angle by End VertebrAnDi Anggara PeramanaNo ratings yet
- Sagittal Plane White PaperDocument14 pagesSagittal Plane White PaperAnant JainNo ratings yet
- Factor Predict ProgressDocument4 pagesFactor Predict ProgressronnyNo ratings yet
- Intraobserver and Interobserver Reliability of The Lenke Classification Among Spine SurgeonsDocument4 pagesIntraobserver and Interobserver Reliability of The Lenke Classification Among Spine SurgeonsazevedoNo ratings yet
- TKF Taylor Scoliosis MeasurementDocument11 pagesTKF Taylor Scoliosis MeasurementGregory SOLOMONSNo ratings yet
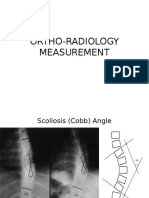
- Ortho Radiology MeasurementDocument25 pagesOrtho Radiology MeasurementNasrul Ha100% (1)
- PDF 6Document13 pagesPDF 6Amina GoharyNo ratings yet
- KJTCV 51 254Document6 pagesKJTCV 51 254gagah152No ratings yet
- Evaluation of Patients With AisDocument50 pagesEvaluation of Patients With AisJosh JoshiNo ratings yet
- INVESTIGATION AND TREATMENT OrthoDocument9 pagesINVESTIGATION AND TREATMENT OrthoMuhammad Jamil Mohamed ShafiNo ratings yet
- Radiographic Evaluation of Spinal Deformity PDFDocument8 pagesRadiographic Evaluation of Spinal Deformity PDFmogosadrianNo ratings yet
- PIIS0003999305009998Document6 pagesPIIS0003999305009998yohanNo ratings yet
- 2022 SRSDocument21 pages2022 SRSTulio RangelNo ratings yet
- Ortho LucaDocument8 pagesOrtho LucaDr TNTNo ratings yet
- The Progression of Lumbar Curves in Adolescent Lenke 1 Scoliosis and The Distal Adding-On Phenomenon. - Lakhal Et Al.2014Document6 pagesThe Progression of Lumbar Curves in Adolescent Lenke 1 Scoliosis and The Distal Adding-On Phenomenon. - Lakhal Et Al.2014Mohammad KaramNo ratings yet
- Pelvic Tilt in The StandingDocument3 pagesPelvic Tilt in The StandingEvanEvan22No ratings yet
- Stretching vs. Traction in ScoliosisDocument11 pagesStretching vs. Traction in ScoliosisLaszlo PeterNo ratings yet
- Sky Line 1Document6 pagesSky Line 1ramadhanNo ratings yet
- The Reliability and Validity of Three Non-Radiological Measures of Thoracic Kyphosis and Their Relations To The Standing Radiological Cobb AngleDocument9 pagesThe Reliability and Validity of Three Non-Radiological Measures of Thoracic Kyphosis and Their Relations To The Standing Radiological Cobb Angle박진영No ratings yet
- Pediatric Scoliosis What Is Scoliosis?Document8 pagesPediatric Scoliosis What Is Scoliosis?Yak NafarNo ratings yet
- Adolescent Idiopathic ScoliosisDocument29 pagesAdolescent Idiopathic ScoliosisfenskaNo ratings yet
- Wits AnalysisDocument1 pageWits Analysisjeff diazNo ratings yet
- Zheng2016 Article AReliabilityAndValidityStudyFoDocument15 pagesZheng2016 Article AReliabilityAndValidityStudyFoMIGUEL ANGEL PALOMINO CAMPONo ratings yet
- ScoliosisDocument5 pagesScoliosisIbe JulienneNo ratings yet
- HIP JOINT Special Tests-WPS OfficeDocument51 pagesHIP JOINT Special Tests-WPS OfficeManisha MishraNo ratings yet
- Kyp Ho Scoliosis 1Document70 pagesKyp Ho Scoliosis 1Tias DiahNo ratings yet
- ScoliosisDocument5 pagesScoliosisIbe JulienneNo ratings yet
- Scoliosis MedbackDocument18 pagesScoliosis MedbackVanessa Yvonne GurtizaNo ratings yet
- Upright, Prone, and Supine Spinal Morphology and Alignment in Adolescent Idiopathic ScoliosisDocument8 pagesUpright, Prone, and Supine Spinal Morphology and Alignment in Adolescent Idiopathic ScoliosisMr. wNo ratings yet
- Young Adult Hip A Systematic Approach To The Plain Radiographic Evaluation of TheDocument21 pagesYoung Adult Hip A Systematic Approach To The Plain Radiographic Evaluation of TheManolis MorakisNo ratings yet
- Manuscript 2Document6 pagesManuscript 2Bodin TappariyapolNo ratings yet
- Adolescent Idiopathic ScoliosisDocument42 pagesAdolescent Idiopathic ScoliosisPerjalanan SukarNo ratings yet
- The Use of Cephalometrics As An Aid To Planning and Assessing Orthodontic Treatment, - American Journal of Orthodontics, Vol. 46, Pp. 721-735, 1960 C.C. SteinerDocument15 pagesThe Use of Cephalometrics As An Aid To Planning and Assessing Orthodontic Treatment, - American Journal of Orthodontics, Vol. 46, Pp. 721-735, 1960 C.C. SteinerMiguel Jaèn100% (1)
- Assessment PDFDocument7 pagesAssessment PDFdrprasantNo ratings yet
- Scoliosis: Ns. M. Nurman, S.Kep Stikes Tuanku Tambusai BangkinangDocument36 pagesScoliosis: Ns. M. Nurman, S.Kep Stikes Tuanku Tambusai Bangkinangwindy noviantyNo ratings yet
- Análisis de Wits, Iinclinación Del Plano Silla-Nasion en La RelacionesDocument11 pagesAnálisis de Wits, Iinclinación Del Plano Silla-Nasion en La RelacionesRicardo LaraNo ratings yet
- 10 Thoracolumbar Spine - ScoliosisDocument8 pages10 Thoracolumbar Spine - Scoliosis楊畯凱No ratings yet
- BracingDocument14 pagesBracingrenihardiyantiNo ratings yet
- Accuracy of Planar Anteversion THADocument8 pagesAccuracy of Planar Anteversion THAManny TantorNo ratings yet
- Clubfoot Imaging - Overview, Radiography, Computed TomographyDocument7 pagesClubfoot Imaging - Overview, Radiography, Computed TomographysidikNo ratings yet
- Cervical Spine AnatomyDocument67 pagesCervical Spine AnatomyAnonymous glhczXqdDNo ratings yet
- Weiss 1995Document5 pagesWeiss 1995RelviGuzmanApazaNo ratings yet
- Natural History of AISDocument42 pagesNatural History of AISJosh JoshiNo ratings yet
- Nyffeler - Effects of Glenoid Compont Version On Humeral Head Displacement and Joint Reaction ForcesDocument5 pagesNyffeler - Effects of Glenoid Compont Version On Humeral Head Displacement and Joint Reaction ForcesRaphael BazanNo ratings yet
- Primary Hip Arthroplasty Templating On Standard Radiographs A Stepwise ApproachDocument31 pagesPrimary Hip Arthroplasty Templating On Standard Radiographs A Stepwise ApproachMarius Chirila100% (1)
- Effect of Cervical Flexion and Extension On Thoracic Sagittal AlignmentDocument5 pagesEffect of Cervical Flexion and Extension On Thoracic Sagittal AlignmentQuiroprácticaParaTodosNo ratings yet
- Re-Re-evaluation of The Condylar Path As The Reference of OcclusionDocument10 pagesRe-Re-evaluation of The Condylar Path As The Reference of Occlusionaziz2007No ratings yet
- What Process Is Best Seen Using A Perpendicular CR With The Elbow in Acute Flexion and With The Posterior Aspect of The Humerus Adjacent To The Image ReceptorDocument22 pagesWhat Process Is Best Seen Using A Perpendicular CR With The Elbow in Acute Flexion and With The Posterior Aspect of The Humerus Adjacent To The Image ReceptorKalpana ParajuliNo ratings yet
- The Clinical Relevance of Hyperkyphosis: A Narrative Review: M. C. Koelé, W. F. Lems and H. C. WillemsDocument7 pagesThe Clinical Relevance of Hyperkyphosis: A Narrative Review: M. C. Koelé, W. F. Lems and H. C. WillemsSoare Elena-CosminaNo ratings yet
- The Clinical Relevance of Hyperkyphosis: A Narrative Review: M. C. Koelé, W. F. Lems and H. C. WillemsDocument7 pagesThe Clinical Relevance of Hyperkyphosis: A Narrative Review: M. C. Koelé, W. F. Lems and H. C. WillemsSoare Elena-CosminaNo ratings yet
- Ventral Correction of Postsurgical Cervical KyphosisDocument7 pagesVentral Correction of Postsurgical Cervical Kyphosis박진영No ratings yet
- 3 - Epidemiology: J 1 6 0 D Gih WitnDocument1 page3 - Epidemiology: J 1 6 0 D Gih WitnIkaKusumaWardhaniNo ratings yet
- Resident Ortho RotationDocument18 pagesResident Ortho RotationRuth PoeryNo ratings yet
- Floating Shoulder, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandFloating Shoulder, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Hyperkyphosis, (Humpback) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHyperkyphosis, (Humpback) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Neurosurgery Procedure Charges DraftDocument8 pagesNeurosurgery Procedure Charges DraftRam Kumar ShresthaNo ratings yet
- Tirumala Tirupati Devasthanams: TirupatiDocument3 pagesTirumala Tirupati Devasthanams: Tirupativenkatraju.YNo ratings yet
- Esu-X 300 NT (CL II B CEE 93/42) : SER Anual ForDocument35 pagesEsu-X 300 NT (CL II B CEE 93/42) : SER Anual Foralejandro sanche mejoradaNo ratings yet
- Suresh Pandey Consultant Orthopedic Surgeon ComsDocument55 pagesSuresh Pandey Consultant Orthopedic Surgeon ComsAryo WibisonoNo ratings yet
- AHN-II Lec2Document20 pagesAHN-II Lec2Abdullah BhattiNo ratings yet
- Table of Contents - YjomsDocument6 pagesTable of Contents - YjomsSUMEET SODHINo ratings yet
- Deltoid Ligament Rupture in Ankle Fracture - Diagnosis and ManagementDocument11 pagesDeltoid Ligament Rupture in Ankle Fracture - Diagnosis and ManagementDiana Marcela Benítez HernándezNo ratings yet
- Tuberculosis of The HipDocument33 pagesTuberculosis of The Hipmuhammad bayu wicaksonoNo ratings yet
- Drexel University College of Medicine Department of AnesthesiologyDocument1 pageDrexel University College of Medicine Department of AnesthesiologydrexelanesthesiaNo ratings yet
- Generaciones de Clavos Endomedulares PDFDocument4 pagesGeneraciones de Clavos Endomedulares PDFkariNo ratings yet
- N. S. Surgical Gujarat IndiaDocument10 pagesN. S. Surgical Gujarat IndiaN. S. SurgicalNo ratings yet
- Brochure FLEXIT EngDocument12 pagesBrochure FLEXIT EngalNo ratings yet
- Total Ankle Arthroplasty - Why Does It Fail?Document7 pagesTotal Ankle Arthroplasty - Why Does It Fail?drjorgewtorresNo ratings yet
- Occupational Health and Safety Quiz: The Canadian Veterinary Journal. La Revue Veterinaire Canadienne February 1997Document5 pagesOccupational Health and Safety Quiz: The Canadian Veterinary Journal. La Revue Veterinaire Canadienne February 1997Jai ChaudhryNo ratings yet
- Nursing Intervention (Risk For Trauma) RationaleDocument5 pagesNursing Intervention (Risk For Trauma) RationaleJay VillasotoNo ratings yet
- E-Catalogue PT MedtekDocument7 pagesE-Catalogue PT MedtekMB SNo ratings yet
- Ultrasound Technical OfferDocument3 pagesUltrasound Technical OfferHani Al-NassNo ratings yet
- Nicole M. Wikoff: Professional SummaryDocument2 pagesNicole M. Wikoff: Professional SummaryJay KulkarniNo ratings yet
- The Brace - An Introduction To Orthodontics For GDPsDocument8 pagesThe Brace - An Introduction To Orthodontics For GDPsChris BarrowNo ratings yet
- Pediatric Hip Dysplasia Case StudyDocument13 pagesPediatric Hip Dysplasia Case Studyapi-349474075No ratings yet
- ALVO Operating TablesDocument44 pagesALVO Operating Tablesvanxuong90No ratings yet
- Ebook Endoscopic Craniosynostosis Surgery An Illustrated Guide To Endoscopic Techniques PDF Full Chapter PDFDocument67 pagesEbook Endoscopic Craniosynostosis Surgery An Illustrated Guide To Endoscopic Techniques PDF Full Chapter PDFsteven.forsythe586100% (27)
- DDH - PFDocument34 pagesDDH - PFAnnisa Oktoviani MursidaNo ratings yet
- Matching Nail Angle and Native Neck-Shaft AngleDocument4 pagesMatching Nail Angle and Native Neck-Shaft AngleDavidBeatonComuladaNo ratings yet
- Chap 2. HOSPITAL AND ITS ORGANIZATIONDocument47 pagesChap 2. HOSPITAL AND ITS ORGANIZATIONhunnylandNo ratings yet
- Gopalan'S Evidence Based Orthopaedic Principles: Hitesh Gopalan U, Ms OrthDocument10 pagesGopalan'S Evidence Based Orthopaedic Principles: Hitesh Gopalan U, Ms OrthDebangshu Kumar0% (1)
- Real Time Surveys Reveal True Feelings About RegistrationDocument8 pagesReal Time Surveys Reveal True Feelings About RegistrationBrittany LudwigNo ratings yet