You might also like
- Chase Sep V 2.9Document11 pagesChase Sep V 2.9faxev83733100% (2)
- Explanation of Benefits This Is Not A BillDocument1 pageExplanation of Benefits This Is Not A BillShannonNo ratings yet
- Chase Sep V 2.9Document11 pagesChase Sep V 2.9faxev8373350% (2)
- Trader TemplateDocument4 pagesTrader TemplateAndre ParnellNo ratings yet
- Statement 2023 07 09Document4 pagesStatement 2023 07 09blackson knightsonNo ratings yet
- Boa JanDocument4 pagesBoa JanHumayon Malek40% (5)
- IYYSCP007870400100 R 19125 DA6 E1 E3621Document1 pageIYYSCP007870400100 R 19125 DA6 E1 E3621Genesis De La Rosa SibajaNo ratings yet
- Feb 2020Document4 pagesFeb 2020andreaNo ratings yet
- July 23, 2009 Through August 24, 2009 JPMorgan Chase BankDocument4 pagesJuly 23, 2009 Through August 24, 2009 JPMorgan Chase BankMaria Blackburn33% (3)
- Bank Statement JuneDocument4 pagesBank Statement JuneHugo Beltran100% (1)
- Estmt - 2022 03 31Document12 pagesEstmt - 2022 03 31Laura MCGNo ratings yet
- Agosto 11Document1 pageAgosto 11dakpi479No ratings yet
- Ebay Order Baterias 9V - Edenorte-FusionadoDocument4 pagesEbay Order Baterias 9V - Edenorte-FusionadoYamilka MedranoNo ratings yet
- FIS TheGlobalPaymentsReport 2023Document182 pagesFIS TheGlobalPaymentsReport 2023Erlend ClaessenNo ratings yet
- Estatement PDFDocument5 pagesEstatement PDFTena Chamberlin100% (1)
- Chapter 2 Cash and Cash EquivalentsDocument13 pagesChapter 2 Cash and Cash Equivalents5555-899341No ratings yet
- Bank of BarodaDocument2 pagesBank of BarodaSudhir SatyanarayanNo ratings yet
- Dover StatementDocument4 pagesDover StatementHeritage Digital ArtsNo ratings yet
- 1563270990991Document11 pages1563270990991JohnNo ratings yet
- Eob RemittanceDocument3 pagesEob RemittanceAndres ChavarrioNo ratings yet
- Eob RemittanceDocument3 pagesEob RemittanceAndres ChavarrioNo ratings yet
- Eob RemittanceDocument2 pagesEob RemittanceAndres ChavarrioNo ratings yet
- Octubre 20Document1 pageOctubre 20dakpi479No ratings yet
- Septiembre 8Document1 pageSeptiembre 8dakpi479No ratings yet
- Agosto 25Document1 pageAgosto 25dakpi479No ratings yet
- Octubre 6Document1 pageOctubre 6dakpi479No ratings yet
- Septiembre 23Document1 pageSeptiembre 23dakpi479No ratings yet
- Payroll DetailDocument7 pagesPayroll Detailnileshbj.taskseverydayNo ratings yet
- Well 56Document6 pagesWell 56Farheen BakaliNo ratings yet
- Seminario Fénix de Brian TracyDocument1 pageSeminario Fénix de Brian TracyVíctor Antonio Rivera fermaintNo ratings yet
- HPP - 317733732 - 12152023Document6 pagesHPP - 317733732 - 12152023Andres Felipe Chavarrio SuarezNo ratings yet
- Sushma Medical BillDocument1 pageSushma Medical Billganeshmadley2000No ratings yet
- 317733731 ---Document4 pages317733731 ---Andres Felipe Chavarrio SuarezNo ratings yet
- Cigna (Constitution) - 1256722 - 12272023Document6 pagesCigna (Constitution) - 1256722 - 12272023Andres Felipe Chavarrio SuarezNo ratings yet
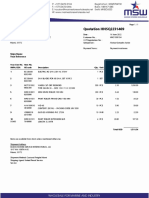
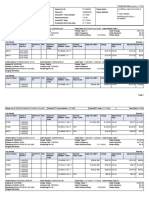
- Quotation HNSQ2231469: Ships Name Your ReferenceDocument2 pagesQuotation HNSQ2231469: Ships Name Your ReferenceRicardo QuijadaNo ratings yet
- Earnings StatementDocument1 pageEarnings StatementsheneriaelamNo ratings yet
- Invoice Gh00094427Document1 pageInvoice Gh00094427Ahmed GomaaNo ratings yet
- OpTransactionHistoryUX307 11 2020Document4 pagesOpTransactionHistoryUX307 11 2020Ajay MauryaNo ratings yet
- Member Loan LedgerDocument2 pagesMember Loan Ledgersumalinogstevensidney491No ratings yet
- Chase DecemberDocument3 pagesChase Decemberraheemtimo1No ratings yet
- Statement of Account: Date Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing BalanceDocument2 pagesStatement of Account: Date Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing Balancepsyamala2004No ratings yet
- Caroline Kemunto Nyabunga - 1000680050Document1 pageCaroline Kemunto Nyabunga - 1000680050Jason MoutiNo ratings yet
- CheckMultipleDetails 2024 01 19 07 08 01Document4 pagesCheckMultipleDetails 2024 01 19 07 08 01hillumbertoNo ratings yet
- Telos PaymentDocument2 pagesTelos Paymentanusha.veldandiNo ratings yet
- Pharmacy Issue Receipt PrintDocument1 pagePharmacy Issue Receipt PrintrajeshbhramaNo ratings yet
- 318466915 - CopyDocument7 pages318466915 - CopyAndres Felipe Chavarrio SuarezNo ratings yet
- Sample Q4'22Document3 pagesSample Q4'22Far DinNo ratings yet
- PolicySoftCopy 665735048Document49 pagesPolicySoftCopy 665735048priyanka.vaidNo ratings yet
- JEDSCP009004000000 R 1914197 E9098621Document1 pageJEDSCP009004000000 R 1914197 E9098621ggsk11119No ratings yet
- Statement of AccountDocument5 pagesStatement of AccountAjay MauryaNo ratings yet
- CheckMultipleDetails 2024 01 18 12 06 44Document8 pagesCheckMultipleDetails 2024 01 18 12 06 44hillumbertoNo ratings yet
- Cigna - 22947494 - 12262023Document8 pagesCigna - 22947494 - 12262023Andres Felipe Chavarrio SuarezNo ratings yet
- Acct Statement XX8251 30102023Document2 pagesAcct Statement XX8251 30102023Shivam DubeyNo ratings yet
- USAA CLASSIC CHECKING - SampleDocument3 pagesUSAA CLASSIC CHECKING - SampleJosey WilliamsNo ratings yet
- StatementDocument3 pagesStatementgarrettloehrNo ratings yet
- 319214285Document7 pages319214285Andres Felipe Chavarrio SuarezNo ratings yet
- Downloaded PaycheckDocument3 pagesDownloaded Paycheckcrystalgeronimo0No ratings yet
- Eft # 211203740Document36 pagesEft # 211203740missansheNo ratings yet
- Bharat Re Payment VocherDocument1 pageBharat Re Payment Vocheranusha.veldandiNo ratings yet
- 24-3331 INNOVE-mergedDocument3 pages24-3331 INNOVE-mergedCaloi VillanuevaNo ratings yet
- Indwdhi 20221130Document11 pagesIndwdhi 20221130Mohd HuzaifahNo ratings yet
- Policy 2022-23Document6 pagesPolicy 2022-23paras INSURANCENo ratings yet
- Commission Statement - BA0000281182 03-2024-1st WeekDocument2 pagesCommission Statement - BA0000281182 03-2024-1st WeekNarendar KumarNo ratings yet
- Insurable InterestDocument26 pagesInsurable InterestGaurav NaulakhaNo ratings yet
- IPru Signature LeafletDocument12 pagesIPru Signature Leafletharsh patelNo ratings yet
- One-Pager-POS Saral Nivesh-1Document2 pagesOne-Pager-POS Saral Nivesh-1abilashvincentNo ratings yet
- A Project Report On Organization Study and Awareness of ICICI Prudential Life Insurance Co. LTDDocument78 pagesA Project Report On Organization Study and Awareness of ICICI Prudential Life Insurance Co. LTDBabasab Patil (Karrisatte)No ratings yet
- Chapter 24Document3 pagesChapter 24Trường Nguyễn CôngNo ratings yet
- Bhavin kkkkkkkkk38Document87 pagesBhavin kkkkkkkkk38Sandip ChovatiyaNo ratings yet
- Ready Forward ContractsDocument7 pagesReady Forward ContractsSatyendra Veer SinghNo ratings yet
- Written Report in M103Document7 pagesWritten Report in M103Katrina EreseNo ratings yet
- CS - Exe - FSM - Analysis SheetDocument19 pagesCS - Exe - FSM - Analysis Sheetshivani dhole100% (1)
- Picasso Inn - 10012021Document2 pagesPicasso Inn - 10012021Safin RNo ratings yet
- Final ExamsDocument7 pagesFinal ExamsRiriNo ratings yet
- Brokerage Fees (Local & Foreign)Document3 pagesBrokerage Fees (Local & Foreign)Soraya AimanNo ratings yet
- ECO 301 - Economic Study MethodsDocument8 pagesECO 301 - Economic Study MethodsHerson Marvin LealNo ratings yet
- Project Report On Audit ProgramDocument58 pagesProject Report On Audit Programsubashrao5522No ratings yet
- Dispute Results 3Document20 pagesDispute Results 3Melvin CandelariaNo ratings yet
- Disclaimers - PNB MetLife Aajeevan Suraksha - tcm47-69311Document2 pagesDisclaimers - PNB MetLife Aajeevan Suraksha - tcm47-69311Vandita KhudiaNo ratings yet
- IFMIS Telangana Cheque Issued Report PDFDocument2 pagesIFMIS Telangana Cheque Issued Report PDFSomeshwar Lakavath100% (1)
- CA Final DT Q MTP 2 Nov23 Castudynotes ComDocument10 pagesCA Final DT Q MTP 2 Nov23 Castudynotes ComRajdeep GuptaNo ratings yet
- Corporate Finance Cheat SheetDocument3 pagesCorporate Finance Cheat Sheet050610220479No ratings yet
- User Stories With Acceptance Criteria and Wireframes PDFDocument13 pagesUser Stories With Acceptance Criteria and Wireframes PDFGyanendra KumarNo ratings yet
- Inward Payment FormDocument4 pagesInward Payment FormGustavo Nasser MazzoNo ratings yet
- Singapore Financial SystemDocument69 pagesSingapore Financial SystemlemxramosNo ratings yet
- Responsiveamguide PDFDocument586 pagesResponsiveamguide PDFNader OkashaNo ratings yet
- Fin701 Module2Document3 pagesFin701 Module2Krista CataldoNo ratings yet
- Quiz Chapter-7 Leases-Part-1 2021Document3 pagesQuiz Chapter-7 Leases-Part-1 2021CENTENO, JOAN R.No ratings yet
- Oregon Investment Council 7 29Document95 pagesOregon Investment Council 7 29Zerohedge100% (2)