You might also like
- Fosfomycin: Review and Use Criteria BackgroundDocument12 pagesFosfomycin: Review and Use Criteria BackgroundAbu Azzam Al-Hadi100% (1)
- Kel. 5 IO Jurol 1Document8 pagesKel. 5 IO Jurol 1Anonymous yyq6Ys7ENo ratings yet
- Fosfomycin-An Old-New AntibioticDocument4 pagesFosfomycin-An Old-New Antibioticvetma1No ratings yet
- Fosfomycin Trometamol in Patients With Renal Insufficiency and in The ElderlyDocument10 pagesFosfomycin Trometamol in Patients With Renal Insufficiency and in The ElderlyInternational Medical PublisherNo ratings yet
- S 005 LBL 7Document14 pagesS 005 LBL 7Mohammed MohammedNo ratings yet
- RDU On Renal DisordersDocument14 pagesRDU On Renal DisordersATHENA MINERVA MORDENONo ratings yet
- Flucytosi Review of PharmacologyDocument10 pagesFlucytosi Review of PharmacologyHanung PujanggaNo ratings yet
- AusparDocument13 pagesAusparManikandan RajenNo ratings yet
- PDF Share Prescribing Information: Mechanism of ActionDocument3 pagesPDF Share Prescribing Information: Mechanism of Actionmehul da aviatorNo ratings yet
- Tetracyclines: Mechanism of ActionDocument16 pagesTetracyclines: Mechanism of Actionammar amerNo ratings yet
- FOSFOMYCINDocument29 pagesFOSFOMYCINDreamline de SkyNo ratings yet
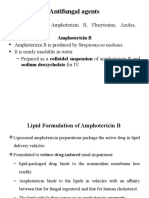
- Antifungal AgentsDocument7 pagesAntifungal AgentstenawNo ratings yet
- Short-Course Nitrofurantoin For The Treatment of Acute Uncomplicated Cystitis in WomenDocument6 pagesShort-Course Nitrofurantoin For The Treatment of Acute Uncomplicated Cystitis in WomenHanifah RifdaNo ratings yet
- Antimicrobials Complete by DR - Mayur Sayta M 91 PDFDocument86 pagesAntimicrobials Complete by DR - Mayur Sayta M 91 PDFRuthvi Jain100% (1)
- Bayer 3rd Proc'99 - PAPICHDocument5 pagesBayer 3rd Proc'99 - PAPICHsergioNo ratings yet
- AntifungalDocument41 pagesAntifungalDeribe BekeleNo ratings yet
- Clinical Efficacy of Fosfomycin For The Treatment of Complicated Lower Tract and Uncomplicated Urinary Tract InfectionsDocument7 pagesClinical Efficacy of Fosfomycin For The Treatment of Complicated Lower Tract and Uncomplicated Urinary Tract InfectionsInternational Medical PublisherNo ratings yet
- Chemotherapy NotesDocument9 pagesChemotherapy Notesnileshkumarhjoshi942No ratings yet
- Milta 2 - MarcadoDocument4 pagesMilta 2 - MarcadoVictor RoticivNo ratings yet
- Drug Use in LeprosyDocument23 pagesDrug Use in LeprosyIrish Nicole DCNo ratings yet
- Bedside Discussion Q&A: 1. Target SPO2 For COAD Patient?Document5 pagesBedside Discussion Q&A: 1. Target SPO2 For COAD Patient?Muhammad MuhammadNo ratings yet
- Quinolones, Folic Acid Antagonist, and Urinary Tract AntisepticsDocument29 pagesQuinolones, Folic Acid Antagonist, and Urinary Tract AntisepticsAliImadAlKhasakiNo ratings yet
- AMINOGLYCOSIDESDocument45 pagesAMINOGLYCOSIDESAbdullah EmadNo ratings yet
- ANTIFUNGALS (Autosaved)Document72 pagesANTIFUNGALS (Autosaved)Franci Kay SichuNo ratings yet
- Pdfshare Prescribing Information: Mechanism of ActionDocument3 pagesPdfshare Prescribing Information: Mechanism of Actionmehul da aviatorNo ratings yet
- FarmakokinetikDocument28 pagesFarmakokinetikhello stalkersNo ratings yet
- Anti Fungal TableDocument4 pagesAnti Fungal TableMaebritt TibubosNo ratings yet
- Ramachandran 2015Document17 pagesRamachandran 2015Andreea MihaiNo ratings yet
- Pharmacokinetics and Pharmacodynamics of Intravenous and Oral Azithromycin: Enhanced Tissue Activity and Minimal Drug InteractionsDocument9 pagesPharmacokinetics and Pharmacodynamics of Intravenous and Oral Azithromycin: Enhanced Tissue Activity and Minimal Drug InteractionsAhmad fadhilNo ratings yet
- Sebuah Model Farmakokinetik Sederhana Berdasarkan Berarti Hotel Times Untuk Memprediksi Paparan Furosemide Setelah Dosis OralDocument16 pagesSebuah Model Farmakokinetik Sederhana Berdasarkan Berarti Hotel Times Untuk Memprediksi Paparan Furosemide Setelah Dosis OralnurulNo ratings yet
- Chronobiol Int. Pediatr Hematol OncolDocument2 pagesChronobiol Int. Pediatr Hematol OncolSean GreenNo ratings yet
- Pharma Uro Cotrimoxazole +fqsDocument14 pagesPharma Uro Cotrimoxazole +fqsHussein AlhaddadNo ratings yet
- Toxicidad Del Misoprostol Sobre La GestaciónDocument8 pagesToxicidad Del Misoprostol Sobre La GestaciónMario SimonovichNo ratings yet
- Cefiget Range Leaflet PakistanDocument2 pagesCefiget Range Leaflet PakistanZafran KhanNo ratings yet
- Antibiotics/Anti-infective: Classes of Drugs That Act As Anti-InfectivesDocument6 pagesAntibiotics/Anti-infective: Classes of Drugs That Act As Anti-InfectivesJL D. BusiaNo ratings yet
- Pharma Reviewer-1Document9 pagesPharma Reviewer-1pinpindalgoNo ratings yet
- Articulo en Ingles de Fumonisinas en EquinosDocument8 pagesArticulo en Ingles de Fumonisinas en Equinosalejandro sotoNo ratings yet
- ChemotherapyDocument10 pagesChemotherapyHasnat HussainNo ratings yet
- JCM 01368-17Document7 pagesJCM 01368-17Smriti SrivastavaNo ratings yet
- Zhan El 2004Document7 pagesZhan El 2004Jaya Semara PutraNo ratings yet
- 317567fumonisin B1Document3 pages317567fumonisin B1tophesnyksNo ratings yet
- Newer Antimalarial DrugsDocument3 pagesNewer Antimalarial DrugsZīshān FārūqNo ratings yet
- Methane Attenuates Lung Ischemiareperfusion Damage Via Controlling PI3KAKTNF?B Signaling WalkwayzfbutDocument2 pagesMethane Attenuates Lung Ischemiareperfusion Damage Via Controlling PI3KAKTNF?B Signaling Walkwayzfbutfridgeplow4No ratings yet
- Fosamin 3 G: DescriptionDocument2 pagesFosamin 3 G: DescriptionSaifur Rahman SuzonNo ratings yet
- Antibacterial and Antifungal DrugsDocument7 pagesAntibacterial and Antifungal Drugszzb9k9w9gzNo ratings yet
- 22 1-S2.0-S0924857908002392-MainDocument3 pages22 1-S2.0-S0924857908002392-MainLookpear ShiiNo ratings yet
- Emerging Mechanisms of Fluoroquinolone Resistance: Special IssueDocument5 pagesEmerging Mechanisms of Fluoroquinolone Resistance: Special IssueAyi Yurike Tri YantiNo ratings yet
- Fluoroquinolone ReviewDocument13 pagesFluoroquinolone ReviewStrept Pneumonia100% (1)
- Flu Oro Quino L OnesDocument28 pagesFlu Oro Quino L Onesbushe_yhane23No ratings yet
- Nutrition and Cancer: To Cite This Article: Weiqun Wang, Yuichiro Tanaka, Zhengkang Han & Carl M. Higuchi (1995)Document12 pagesNutrition and Cancer: To Cite This Article: Weiqun Wang, Yuichiro Tanaka, Zhengkang Han & Carl M. Higuchi (1995)juanita calistaNo ratings yet
- Quinolone: Quinolone, Folic Acid Antagonists and Urinary Tract AntisepticsDocument9 pagesQuinolone: Quinolone, Folic Acid Antagonists and Urinary Tract AntisepticsNirav ValandNo ratings yet
- Sulfonamides and Sulfonamide Combinations : Continued On Next PageDocument4 pagesSulfonamides and Sulfonamide Combinations : Continued On Next PageIfan ZulfantriNo ratings yet
- Chloramphenicol: Ayen University - Al College of PharmacyDocument7 pagesChloramphenicol: Ayen University - Al College of Pharmacyمحمد حميد عطيةNo ratings yet
- Targeting Enzymes Involved in Chemotherapeutic AgentsDocument43 pagesTargeting Enzymes Involved in Chemotherapeutic AgentsAnuj DesaiNo ratings yet
- Study of Antiepileptic Drug Fosphenytoin A ProdrugDocument10 pagesStudy of Antiepileptic Drug Fosphenytoin A ProdrugAhmadNo ratings yet
- Advances in Veterinary Antimicrobial Therapy and Forensic ToxicologyDocument230 pagesAdvances in Veterinary Antimicrobial Therapy and Forensic ToxicologySunilNo ratings yet
- Antifung G6Document28 pagesAntifung G6Nigel MaphosaNo ratings yet
- Antifungal Agents 17971Document35 pagesAntifungal Agents 17971TES SENNo ratings yet
- Otc Template Pi BromhexineDocument6 pagesOtc Template Pi BromhexinedahlyahanumNo ratings yet
- Pharmacology- The Molecular Dance: Understanding Drug Interactions: Harmony and Chaos: The Symphony of Drug InteractionsFrom EverandPharmacology- The Molecular Dance: Understanding Drug Interactions: Harmony and Chaos: The Symphony of Drug InteractionsNo ratings yet
- Medication ErrorsDocument3 pagesMedication ErrorsjamiemapanaoNo ratings yet
- Abc Ven 2020Document81 pagesAbc Ven 2020CorneLia JacintaNo ratings yet
- Hospital Pharmacy ProfileDocument7 pagesHospital Pharmacy ProfileJessica BautistaNo ratings yet
- Master Program in Clinical Pharmacy Curriculum 1 PDFDocument1 pageMaster Program in Clinical Pharmacy Curriculum 1 PDFhadiatussalamah100% (2)
- Nepalese Pharmaceutical Industries & Who GMPDocument6 pagesNepalese Pharmaceutical Industries & Who GMPJaya Bir Karmacharya100% (1)
- Curriculum VitaeDocument5 pagesCurriculum Vitaeapi-404239289No ratings yet
- 1.1 Drug Discovery and DevelopmentDocument50 pages1.1 Drug Discovery and DevelopmentgoswamiphotostatNo ratings yet
- Banned Drugs ListDocument380 pagesBanned Drugs ListKarthik75% (4)
- Berno 1Document24 pagesBerno 1Try AdipradanaNo ratings yet
- Ambrisentan: Jamie D. Croxtall and Susan J. KeamDocument10 pagesAmbrisentan: Jamie D. Croxtall and Susan J. KeamElden Kyle BillonesNo ratings yet
- TMC Formulary 2018: Dosage Form Dosage Strength Brand Name With Item Description Generic NameDocument15 pagesTMC Formulary 2018: Dosage Form Dosage Strength Brand Name With Item Description Generic NameKj BrionesNo ratings yet
- Obat Generik Dan Persamaan ObatnyaDocument4 pagesObat Generik Dan Persamaan ObatnyaAlya PuspitaNo ratings yet
- Clinical Research ICRIDocument37 pagesClinical Research ICRIanu87scorpNo ratings yet
- Part No Product Name Location Batch No Expired Date QTY OnhandDocument6 pagesPart No Product Name Location Batch No Expired Date QTY OnhandRatih SafrianiNo ratings yet
- Biowaivers & BiosimilarsDocument11 pagesBiowaivers & BiosimilarsomicspublishinggroupNo ratings yet
- Obat ObatDocument8 pagesObat ObatMuhammad Aulia KurniawanNo ratings yet
- Cluster SPKDocument2 pagesCluster SPKHeru Khairul UmamNo ratings yet
- 13 Chapter 5Document64 pages13 Chapter 5yoganaNo ratings yet
- Social-Behavioral-Administrative Sciences Questions Part3Document17 pagesSocial-Behavioral-Administrative Sciences Questions Part3Rawan Alanazi100% (1)
- Con 528103Document17 pagesCon 528103Jagdish ChanderNo ratings yet
- Price List PT - Thirza 2019Document8 pagesPrice List PT - Thirza 2019Permana JuliansyahNo ratings yet
- Acetaminophen Toxicity in ChildrenDocument5 pagesAcetaminophen Toxicity in Childrendaniascl9527No ratings yet
- Hard HPMC CapsulesDocument3 pagesHard HPMC CapsulesnaturalcapsulesNo ratings yet
- ActemraDocument7 pagesActemraLinda KvastadNo ratings yet
- Chapter 9 - Solid Oral Modified-Release Dosage Forms PDFDocument7 pagesChapter 9 - Solid Oral Modified-Release Dosage Forms PDFRence Kier Sieth RubiasNo ratings yet
- Hospital Pharmacy and Its Organization-Lecture NotesDocument13 pagesHospital Pharmacy and Its Organization-Lecture NotesPatras BhattiNo ratings yet
- Oral Thin Films ThesisDocument4 pagesOral Thin Films Thesisbskb598g100% (1)
- Med Ex 1Document117 pagesMed Ex 1alex_paskaNo ratings yet
- Regulatory Framework For Cell Therapies - Europe, US, and JapanDocument60 pagesRegulatory Framework For Cell Therapies - Europe, US, and JapannovrodNo ratings yet
- Preventing Medication Errors in Pediatric and Neonatal PatientsDocument55 pagesPreventing Medication Errors in Pediatric and Neonatal PatientsJanarth NanNo ratings yet