You might also like
- Studyprotocol Open Access: Lopes Et Al. Trials (2022) 23:87Document14 pagesStudyprotocol Open Access: Lopes Et Al. Trials (2022) 23:87Rogério MelaréNo ratings yet
- Virtual Reality Exercise Games For High School Students With Intellectual and Developmental DisabilitiesDocument10 pagesVirtual Reality Exercise Games For High School Students With Intellectual and Developmental DisabilitiesShaikh Muhammad UmairNo ratings yet
- Effect of Virtual Reality Exercises On BalanceDocument9 pagesEffect of Virtual Reality Exercises On BalanceLuís Otávio S. BarbosaNo ratings yet
- Influence of The Use of Wii Games On Physical Frailty Components in Institutionalized Older AdultsDocument11 pagesInfluence of The Use of Wii Games On Physical Frailty Components in Institutionalized Older AdultsYanella Millacura MillaldeoNo ratings yet
- Cognitive-Motor Exergaming For Reducing Fall Risk in People With Chronic Stroke: A Randomized Controlled TrialDocument18 pagesCognitive-Motor Exergaming For Reducing Fall Risk in People With Chronic Stroke: A Randomized Controlled TrialZilbran BerontaxNo ratings yet
- Archives of Gerontology and GeriatricsDocument9 pagesArchives of Gerontology and GeriatricsHélio YoshidaNo ratings yet
- Custom-Designed Motion-Based Games For Older Adults: A Review of Literature in Human-Computer InteractionDocument13 pagesCustom-Designed Motion-Based Games For Older Adults: A Review of Literature in Human-Computer InteractionOsman PetitNo ratings yet
- Individual Differences in Response To Cognitive Training: Using A Multi-Modal, Attentionally Demanding Game-Based Intervention For Older AdultsDocument6 pagesIndividual Differences in Response To Cognitive Training: Using A Multi-Modal, Attentionally Demanding Game-Based Intervention For Older Adultsjherj hgcxNo ratings yet
- Ching Teng2019Document15 pagesChing Teng2019Andika ApriyandiNo ratings yet
- Cyber Cycle StudyDocument11 pagesCyber Cycle StudyArunkumar RangarajanNo ratings yet
- Ijmcl v3n3p33 enDocument14 pagesIjmcl v3n3p33 ensamyNo ratings yet
- Webster A. Et Al 2020 Upper Limb Rehabilitation Interventions Using Virtual Reality For People With Multiple Sclerosis A Systematic ReviewDocument27 pagesWebster A. Et Al 2020 Upper Limb Rehabilitation Interventions Using Virtual Reality For People With Multiple Sclerosis A Systematic Reviewsarawu9911No ratings yet
- Chan 2020 DiscussãoDocument47 pagesChan 2020 DiscussãoCássia Fernanda do Carmo AmaralNo ratings yet
- Maharaj 2016Document9 pagesMaharaj 2016dina sarah hanifahNo ratings yet
- Effectiveness of Board Game Activities For Reducing Depression Among Older Adults in Adult Day Care Centers of Taiwan.. A Quasi-Experimental StudyDocument14 pagesEffectiveness of Board Game Activities For Reducing Depression Among Older Adults in Adult Day Care Centers of Taiwan.. A Quasi-Experimental StudyamirvafaaaaNo ratings yet
- IBRO Reports: Research PaperDocument8 pagesIBRO Reports: Research PaperSamara DiasNo ratings yet
- Kottle 2022Document16 pagesKottle 2022annamrobisonNo ratings yet
- Literature ReviewDocument12 pagesLiterature ReviewMax O. ChangNo ratings yet
- Working in Old Age in Mexico Implications For CognDocument21 pagesWorking in Old Age in Mexico Implications For CognMaría Francisca Cabezas HenríquezNo ratings yet
- 2018 Article 1381Document15 pages2018 Article 1381Ariane de Senna PoltozziNo ratings yet
- c647 PDFDocument8 pagesc647 PDFSuhlis ShwNo ratings yet
- Internet-Based Brain Training Games, Citizen Scientists, and Big Data Ethical Issues in Unprecedented Virtual TerritoriesDocument4 pagesInternet-Based Brain Training Games, Citizen Scientists, and Big Data Ethical Issues in Unprecedented Virtual TerritoriesManal ChennoufNo ratings yet
- 2022 08 26 505430v1 FullDocument33 pages2022 08 26 505430v1 FullMageeNo ratings yet
- 1 s2.0 S105381192100046X MainDocument9 pages1 s2.0 S105381192100046X MainDavid SilRzNo ratings yet
- Brewer2022 Article AQuickMeasureOfTheoryOfMindInADocument18 pagesBrewer2022 Article AQuickMeasureOfTheoryOfMindInAFlori MNo ratings yet
- Virtual Reality For Social Skills Training in AutismDocument14 pagesVirtual Reality For Social Skills Training in Autismshaima nasimNo ratings yet
- Virtual Reality and Motor Imagery PromisDocument13 pagesVirtual Reality and Motor Imagery PromisLudovica MontesiNo ratings yet
- Virtual Game Vs Physical GameDocument5 pagesVirtual Game Vs Physical GameROBIN DAS 212-15-4153No ratings yet
- Nre 192931Document11 pagesNre 192931Fabricio CardosoNo ratings yet
- Borland R IntellectualDocument23 pagesBorland R Intellectualgameingguy35No ratings yet
- Do Violent Video Games Cause Behavior Problems?: Your Position On An IssueDocument2 pagesDo Violent Video Games Cause Behavior Problems?: Your Position On An IssueXiaresse AndayaNo ratings yet
- Ijerph 19 14081 v2Document10 pagesIjerph 19 14081 v2MULUKEN TILAHUNNo ratings yet
- Reduced Relative Colume in Motor and Attention Regions in Developmental Coordination Disorder - A Voxel-Based Morphometry StudyDocument25 pagesReduced Relative Colume in Motor and Attention Regions in Developmental Coordination Disorder - A Voxel-Based Morphometry StudyAlba GonzálezNo ratings yet
- Effectiveness of Virtual Reality in CPDocument15 pagesEffectiveness of Virtual Reality in CPAnnisa NelsonNo ratings yet
- 4 FFBDocument7 pages4 FFBDian Ika CahyaniNo ratings yet
- Hooper Visual Organization Test PsychometricDocument10 pagesHooper Visual Organization Test PsychometricJosiane AlmeidaNo ratings yet
- tmp25FC TMPDocument9 pagestmp25FC TMPFrontiersNo ratings yet
- CSG Thesis FinalDocument236 pagesCSG Thesis FinalIshal D ProtolzzNo ratings yet
- A Systematic Review of Robotic Rehabilitation For Cognitive TrainingDocument24 pagesA Systematic Review of Robotic Rehabilitation For Cognitive TrainingTaciany SantosNo ratings yet
- Cognitive Benefits of Video Games - Hàn Khải Vinh - Kangaroo 1Document5 pagesCognitive Benefits of Video Games - Hàn Khải Vinh - Kangaroo 1Vinh HanNo ratings yet
- Cognitive Function, Physical Activity, and Aging: Possible Biological Links and Implications For Multimodal InterventionsDocument17 pagesCognitive Function, Physical Activity, and Aging: Possible Biological Links and Implications For Multimodal Interventionskatherine monsalveNo ratings yet
- Use of Serious Games With Older Adults Systematic Literature ReviewDocument17 pagesUse of Serious Games With Older Adults Systematic Literature ReviewtyanafmNo ratings yet
- EPJ Motor Proficiency of Children With Autism Spectrum Disorders and Intellectual Disabilities: A ReviewDocument25 pagesEPJ Motor Proficiency of Children With Autism Spectrum Disorders and Intellectual Disabilities: A ReviewCamila MachadoNo ratings yet
- Determining The Effect of Sleep Deprivation To Cognitive PerformanceDocument8 pagesDetermining The Effect of Sleep Deprivation To Cognitive Performancejhestoni liwesNo ratings yet
- Biofeedback For Training Balance and Mobility Tasks in Older Populations: A Systematic ReviewDocument15 pagesBiofeedback For Training Balance and Mobility Tasks in Older Populations: A Systematic ReviewRitu SinghNo ratings yet
- Social Balance Ball Designing and Evaluating An Exergame That Promotes Social Interaction Between Older and Younger PlayersDocument25 pagesSocial Balance Ball Designing and Evaluating An Exergame That Promotes Social Interaction Between Older and Younger PlayerstyanafmNo ratings yet
- J Intellect Disabil Res - 2023 - LalorDocument23 pagesJ Intellect Disabil Res - 2023 - LalorIvca Garrido MezaNo ratings yet
- Efffectiveness of VRR in MSDocument9 pagesEfffectiveness of VRR in MSSM199021No ratings yet
- Neurobiological Mechanisms Underlying Internet Gaming DisorderDocument15 pagesNeurobiological Mechanisms Underlying Internet Gaming DisorderKhaira MaulidaNo ratings yet
- Nintendo Wii Versus Xbox Kinect For Assisting People With Parkinson's DiseaseDocument20 pagesNintendo Wii Versus Xbox Kinect For Assisting People With Parkinson's DiseaseASD2019No ratings yet
- Jurnal Internasional Loren 2Document7 pagesJurnal Internasional Loren 2Loren syafritaNo ratings yet
- How Are Combinations of Physical Activity SedentarDocument26 pagesHow Are Combinations of Physical Activity SedentarMORRIN CHOIRUNNISA THOHIRANo ratings yet
- Childhood ObesityDocument10 pagesChildhood ObesityedgarNo ratings yet
- Chao 2014Document24 pagesChao 2014Adrian BotelloNo ratings yet
- Correlation Between Videogame Mechanics and ExecutiveDocument23 pagesCorrelation Between Videogame Mechanics and ExecutiveChristian F. VegaNo ratings yet
- The Effects of A Virtual Reality Rehabilitation Task On Elderly Subjects - An Experimental Study Using Multimodal DataDocument9 pagesThe Effects of A Virtual Reality Rehabilitation Task On Elderly Subjects - An Experimental Study Using Multimodal DataAgus SGNo ratings yet
- Relation Between Executive Functions and Screen Time Exposure in Under 6Document10 pagesRelation Between Executive Functions and Screen Time Exposure in Under 6eup_1983No ratings yet
- Cognitive Games and BenefitsDocument16 pagesCognitive Games and BenefitsPierre UlysseNo ratings yet
- Journal Pre-Proof: Computers & EducationDocument15 pagesJournal Pre-Proof: Computers & EducationvogonsoupNo ratings yet
- Enhancing the Human Experience - Strategic Insights into Augmentation and BeyondFrom EverandEnhancing the Human Experience - Strategic Insights into Augmentation and BeyondNo ratings yet
- Solar Powered Sensor Base Irrigation System: Puneeth Kumar G.B Swathi H.CDocument4 pagesSolar Powered Sensor Base Irrigation System: Puneeth Kumar G.B Swathi H.CfarizalNo ratings yet
- Sizing & Costing - HEX& Storage TanksDocument26 pagesSizing & Costing - HEX& Storage TanksNg Kai EnNo ratings yet
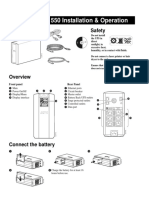
- Back-UPS RS 550 Installation & Operation: Inventory SafetyDocument7 pagesBack-UPS RS 550 Installation & Operation: Inventory SafetyAndrej VukalovicNo ratings yet
- Pacsystems Rx3I: Central Processing UnitDocument12 pagesPacsystems Rx3I: Central Processing UnitDekali FouadNo ratings yet
- Roller Coaster Tycoon 3 ManualDocument14 pagesRoller Coaster Tycoon 3 Manualjohnlondon125No ratings yet
- SPE 11579 Improved Well Stimulation With Resin-Coated ProppantsDocument8 pagesSPE 11579 Improved Well Stimulation With Resin-Coated ProppantsbayuNo ratings yet
- TEMPCORE® Process To Produce Low-Cost High Strength RebarsDocument7 pagesTEMPCORE® Process To Produce Low-Cost High Strength Rebarsamber sareenNo ratings yet
- GPC Browser GuideDocument11 pagesGPC Browser GuideAmr RizkNo ratings yet
- NetSuite SuiteTax Setup Guide PDFDocument75 pagesNetSuite SuiteTax Setup Guide PDFAnurag Singh100% (1)
- Chapt 1 Quy Dinh Lien Quan KD XNK - Ver2020Document9 pagesChapt 1 Quy Dinh Lien Quan KD XNK - Ver2020Thy NguyễnNo ratings yet
- Cybersecurity Essentials v3 0 OverviewDocument1 pageCybersecurity Essentials v3 0 OverviewMuhammad Yasir KhanNo ratings yet
- Partex EnglishDocument16 pagesPartex EnglishDaniyal ParvezNo ratings yet
- Seminar Report ON Cloud Storage 1Document25 pagesSeminar Report ON Cloud Storage 1Krishna KhedkarNo ratings yet
- User Manual: PV Analyzer Z100Document37 pagesUser Manual: PV Analyzer Z100Duyệt Đinh XuânNo ratings yet
- Power SupplyDocument15 pagesPower SupplyVelu SNo ratings yet
- Hands On - Docker Coreos - Docker - Kubernetes Deployment With ForemanDocument14 pagesHands On - Docker Coreos - Docker - Kubernetes Deployment With ForemanpepeqfNo ratings yet
- CCTV and Access Control SpecificationDocument9 pagesCCTV and Access Control Specificationbipin19901100% (1)
- Sage Tutorial PDFDocument113 pagesSage Tutorial PDFIonut StoicaNo ratings yet
- 4/3 Directional High-Response Control Valves, Direct Operated, With Integrated Control Electronics (OBE)Document14 pages4/3 Directional High-Response Control Valves, Direct Operated, With Integrated Control Electronics (OBE)yasin çakırNo ratings yet
- Netec Video Player Quick Start Guide 5.10Document10 pagesNetec Video Player Quick Start Guide 5.10ubik59No ratings yet
- Select and Use ICT ToolsDocument36 pagesSelect and Use ICT ToolsKathrine Victorino0% (1)
- Introduction To Classification - PPT Slides 1Document62 pagesIntroduction To Classification - PPT Slides 1Saurabh PratapNo ratings yet
- Grade 10 Math Q2 FULL Week 1 - WatermarkDocument28 pagesGrade 10 Math Q2 FULL Week 1 - WatermarkSophia Junelle100% (1)
- TC55 Android KK BSP v2.68 GMS LifeGuard Update 11 ReleaseNotesDocument9 pagesTC55 Android KK BSP v2.68 GMS LifeGuard Update 11 ReleaseNotesJose De LeonNo ratings yet
- LKPD PPKN Xi Bab 1-2 Substansi HamDocument8 pagesLKPD PPKN Xi Bab 1-2 Substansi HamFandi SetiawanNo ratings yet
- Item StockDocument50 pagesItem StockRizki AmrullahNo ratings yet
- Learn Python - Step-by-StepDocument40 pagesLearn Python - Step-by-Stepharish400No ratings yet
- Trojan HorseDocument6 pagesTrojan Horsemathew roshanNo ratings yet
- Slem Housekeeping Grades 9 10 Week - 8Document9 pagesSlem Housekeeping Grades 9 10 Week - 8Anne AlejandrinoNo ratings yet
- Aerial Infrared Thermography For Low-Cost and Fast Fault Detection in Utility-Scale PV Power PlantsDocument14 pagesAerial Infrared Thermography For Low-Cost and Fast Fault Detection in Utility-Scale PV Power PlantsJoão TeixeiraNo ratings yet