Professional Documents
Culture Documents
Muscle Dysfunction Associated With Chronic Obstructive Pulmonary Disease
Muscle Dysfunction Associated With Chronic Obstructive Pulmonary Disease
Uploaded by
MarcelaOriginal Description:
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Muscle Dysfunction Associated With Chronic Obstructive Pulmonary Disease
Muscle Dysfunction Associated With Chronic Obstructive Pulmonary Disease
Uploaded by
MarcelaCopyright:
Available Formats
Muscle Dysfunction Associated With
Chronic Obstructive Pulmonary Disease
Neil R MacIntyre MD FAARC
Introduction: Systemic Effects of Chronic Obstructive Pulmonary Disease
on Skeletal Muscle
Respiratory Versus Other Skeletal Muscle Function in COPD
What Effect Do These Muscle Abnormalities Have on Function (Exercise
Tolerance) in COPD?
Approaches to Treatment
Summary
Skeletal-muscle (both respiratory and limb) abnormalities are common and can have profound
effects in patients with chronic inflammatory states such as chronic obstructive pulmonary disease
(COPD). Causes include direct inflammatory-mediator effects on muscle function, malnutrition,
blood-gas abnormalities, compromised oxygen delivery from right-heart dysfunction, electrolyte
imbalances, drugs, and comorbid states. In COPD patients, respiratory muscles are overloaded,
which leads to increased fatigue potential, especially during exercise, when hyperinflation worsens.
Interestingly, overloaded respiratory muscles develop structural changes that help them adapt to
these conditions. In contrast, limb (especially lower extremity) muscles in COPD patients are
underloaded as a consequence of disuse, and this leads to muscle atrophy. Treatment is aimed at
optimizing lung function, nutritional repletion, aerobic exercise training, and (in certain patients)
oxygen therapy. Resistive breathing training is more controversial. Lung-volume-reduction surgery
may help with the hyperinflation effects and improve gas exchange and respiratory-muscle function
in selected patients. Key words: chronic obstructive pulmonary disease, COPD, respiratory muscles.
[Respir Care 2006;51(8):840 – 848. © 2006 Daedalus Enterprises]
Introduction: Systemic Effects of Chronic performance, but also for providing the vital pumping func-
Obstructive Pulmonary Disease on Skeletal Muscle tion of the diaphragm and the heart. The primary structures
of skeletal muscle are sarcomeres.1–5 Sarcomeres contain
Skeletal muscle composes approximately 73% of total actin and myosin components that contract under nerve
body mass. It is critical not only for locomotion and task stimulation, which causes calcium-ion changes across the
membrane. Skeletal muscle is composed of several differ-
ent fiber types, which perform different functions and have
Neil R MacIntyre MD FAARC is affiliated with Respiratory Care Ser- different metabolic properties (Table 1).1–5 The distribu-
vices, Duke University Medical Center, Durham, North Carolina. tion of fiber types in a given muscle depends on the func-
tions the muscle performs. Type I fibers have considerable
Neil R MacIntyre MD FAARC presented a version of this paper at the
37th RESPIRATORY CARE Journal Conference, “Neuromuscular Disease in oxidative capacity and have high mitochondrial density.
Respiratory and Critical Care Medicine,” held March 17–19, 2006, in These fibers provide tonic or repetitive function such as
Ixtapa, Mexico. maintaining antigravity conditions and pumping actions of
Correspondence: Neil R MacIntyre MD FAARC, Respiratory Care Ser-
the heart or the diaphragm. Type I fibers are noticeably
vices, PO Box 3911, Duke University Medical Center, Durham NC 27710. resistant to fatigue. Type II fibers have relatively more
E-mail: neil.macintyre@duke.edu. sarcomeric structures and have less mitochondrial density.
840 RESPIRATORY CARE • AUGUST 2006 VOL 51 NO 8
MUSCLE DYSFUNCTION ASSOCIATED WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE
Table 1. Properties of Muscle-Fiber Types
Muscle-Fiber Type Description Metabolism Myoglobin/mitochondria Function
I Slow, fatigue-resistant Oxidative Rich, “red” Standing
Quiet breathing
IIa* Fast, fatigue-resistant Oxidative/glycolytic Mixed Walking
Hyperventilating
IIb* Fast, fatigable Glycolytic Low, “white” Jumping
Coughing
* An intermediate Type IIx fiber with fast twitch features and intermediate fatigability has also been described.
Table 2. Systemic Effects of COPD on Skeletal Muscle general. Reduced protein intake leads to muscle break-
down, as muscle proteins and amino acids are used for fuel
Direct Effects
(catabolism). This is particularly true of the sarcomere
Myotoxic cytokines are produced as part of the chronic pro-
inflammatory state structures in type II muscle fibers. Malnutrition also con-
Hypoxia is produced by impaired oxygen delivery tributes to reduced muscle enzyme capacity and reduced
Acidosis is produced by hypercapnia and glycolytic metabolism availability of energy substrates such as adenosine triphos-
Complicating Factors phate, magnesium, and potassium.28 –32
Malnutrition In COPD, hypoxemia is common. Hypoxemia leads to
Comorbid conditions lower O2 content in the blood and can elevate pulmonary
Age vascular resistance, creating pulmonary arterial hyperten-
Pathologic Consequences
sion and consequent right-heart failure.33–37 The resulting
Direct muscle protein structural and biochemical changes
Ischemia reperfusion injury
reduced cardiac output, coupled with the low oxygen con-
Reduced glutathione and defense against oxidative stress tent, reduces oxygen delivery to all the organs of the body,
including skeletal muscle. Interestingly, because the work
COPD ⫽ chronic obstructive pulmonary disease of breathing (load) on the diaphragm is substantially in-
creased in COPD (see below), the respiratory-muscles
“steal” blood away from skeletal muscles, which further
compromises systemic muscle function.38,39
They are capable of performing more sudden, intense ten-
Systemic inflammation may also impair the oxygen trans-
sion-generation, but, depending on their mitochondrial den-
sity, become less and less resistant to fatigue. These mus- port through the cytoplasm and into the mitochondria and
cles perform activities such as jumping and coughing. directly impair mitochondrial oxygen utilization,33–36,40 – 42
Chronic inflammatory states such as chronic obstructive which produces muscle-cell hypoxia and thus a conversion
pulmonary disease (COPD) can profoundly affect skeletal to anaerobic metabolism at low levels of exercise. This
muscle function.6 –9 This is related to systemic inflamma- leads to lactate accumulation and earlier fatigability of the
tory mediators that are persistently elevated in these chronic muscles.28,43– 46
disease states and to various other physiologic and comor- Hypercarbia is also a common occurrence in COPD, as
bid effects (Table 2). the central respiratory controllers in the brainstem reduce
Systemic inflammatory mediators accelerate muscle- ventilation to “protect” overloaded ventilatory muscles.47
protein turnover through ubiquitins.10 –16 This leads to loss Some data suggest that a mild respiratory acidosis might
of muscle mass and the clinical appearance of “muscle attenuate some forms of cellular injury,48 but this has not
wasting.”6 –9,17,18 Chronic inflammation also increases mus- been well studied in skeletal muscle. In contrast, an acute
cle oxidative stress and increases reactive oxygen species, severe respiratory acidosis, as might occur during a COPD
which directly damage muscle proteins and impair their exacerbation, can impair muscle enzyme activity and func-
function.19 –21 Additionally, during muscle-fatigue recov- tion.49 –51
ery, an ischemia reperfusion injury mediated through ad- COPD patients often use corticosteroids. As much as
ditional reactive oxygen species may also develop in the 10% of the COPD population may be on long-term oral
muscles, which further impairs muscle function.19 –21 steroids, and the majority of patients with moderately se-
Patients with COPD are also malnourished, and weight vere COPD take inhaled corticosteroids.52 COPD patients
loss occurs in approximately 30% of COPD out-pa- also take corticosteroids during COPD exacerbations. Cor-
tients22–27 because of decreased caloric intake and the ef- ticosteroids can profoundly affect skeletal muscle. Specif-
fects of chronic inflammation on energy metabolism in ically, corticosteroids reduce contractile proteins, increase
RESPIRATORY CARE • AUGUST 2006 VOL 51 NO 8 841
MUSCLE DYSFUNCTION ASSOCIATED WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE
protein breakdown and turnover, down-regulate growth chanical disadvantage and loss of tension-generation ca-
factors, reduce glycolytic activity, and lead to sarcomere pabilities.
and type II cell atrophy.53–55 It is important to note that respiratory muscles have adap-
Finally, COPD often coexists with other chronic dis- tive capabilities to deal with the chronically elevated work
eases that can, by themselves, affect skeletal muscle. Con- load and distorted diaphragm geometry.68,69 Structurally, di-
gestive heart failure and reduced cardiac output can impair aphragmatic sarcomeres become shorter to adapt to the new
oxygen delivery, as described above. Electrolyte and met- shorter resting length. This returns some of the efficiency lost
abolic disturbances from chronic renal or liver disease can in the earlier phases of COPD. More oxidative or type I
also impair muscle function. Diabetes and altered glucose sarcomeres also develop, and these increase endurance capa-
metabolism can also contribute to muscle dysfunction. The bilities. Capillary density is also increased, which leads to the
aging process also impacts muscle function, as there is a respiratory muscles “stealing” blood flow.38,70,71 However,
normal age-related decline in muscle mass.56,57 along with this is a small decrease in type II fibers, which can
lead to less force-generation capability by the diaphragm.70
Respiratory Versus Other Skeletal Also observed in diaphragm biopsies of hyperinflated COPD
Muscle Function in COPD patients are structural changes in titins and nebulins, which
are large muscle proteins that stabilize the actin and myosin
Respiratory muscles in COPD have considerably differ- contractile proteins.72
ent loading patterns than other skeletal muscles. In limb An important question is whether respiratory muscles in
muscles, especially lower-extremity limb muscles, muscle fact fatigue. Fatigue, by definition, is the loss of muscle
weakness and respiratory insufficiency lead to inactivity contractile capabilities induced by heavy loading and re-
and chronic underloading of the muscles. In contrast, re- coverable by rest.73 Fatigue must be distinguished from
spiratory muscles have to deal with an increased work to reduced muscle capability and from muscle injury that
breathe and are thus chronically overloaded. These differ- reduces function.74 Fatigue is of 2 types: peripheral (direct
ent loading patterns produce profoundly different biochem- muscle failure) and central (either a reduction in neural
ical and structural effects over time, as well as affecting stimulation or an increase in inhibitor neuron activity).
the pattern of regional blood flow. Central fatigue is sometimes thought of as a “protective”
In limb muscles, underloading leads to less muscle mass, mechanism that prevents muscles from being injured un-
especially decreases in the type I fibers.58 – 63 This reduces der overload conditions.75 Interestingly, endorphins may
the oxidative capacity of the muscles and makes them play an important role in reducing neural stimulation of
more prone to fatigue. There is also less capillary density the muscles.
with underloading, which leads to reduced regional blood Under normal conditions, respiratory muscles appear
flow delivery, nutrient delivery, and waste removal. Un- capable of maintaining approximately 40% of their max-
loading also leads to less glutathione and other defenses imum pressure-generation capability on a repetitive basis
against oxidative stress. almost indefinitely.76 But when the pressure requirement
In COPD the high inspiratory (and expiratory) airway to breathe is high, especially if the inspiratory time re-
resistance can dramatically increase the pressure require- quired to deliver an adequate tidal breath becomes suffi-
ments for airflow and thus dramatically increase the work ciently long, it does appear that respiratory muscle can
of breathing.64,65 To put numbers on this, consider that the fatigue. This is most easily represented by the pressure/
normal work of breathing at rest is roughly 5 J/min and the inspiratory-time relationship or pressure-time index:
respiratory muscles require roughly 5 mL/min of oxygen
delivery to do this. In COPD, however, these loads and PTI⫽Pdi/Pdi-max⫻TI/Ttot
energy requirements can be increased 5-fold or even 10-
fold.65 in which PTI is the pressure-time index, Pdi is the dia-
Compounding the effects of excessive loading is the phragm pressure during the breath, Pdi-max is the maximum
fact that the work pattern is of an inefficient type, in that diaphragm pressure possible, and TI/Ttot is the ratio of the
high pressure is required for a given movement or dis- inspiratory time to the total-breathing-cycle time (ie,
placement of the sarcomeres.65 This “isometric” type work duty cycle).77 When the PTI of the respiratory muscles
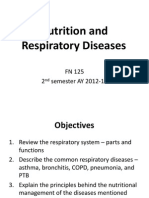
is far less oxygen-efficient than the low-pressure work is ⱖ 0.15, fatigue will occur (Fig. 1).
pattern of normal breathing, and it predisposes to early
fatigue. Respiratory muscles are also compromised by hy- What Effect Do These Muscle Abnormalities Have
perinflation produced by airway collapse and low elastic on Function (Exercise Tolerance) in COPD?
recoil.66,67 As the hyperinflation increases, the diaphragm
is pushed downward and flattens, which shortens the rest- Muscle dysfunction affects exercise tolerance in several
ing length of the diaphragm, producing a substantial me- ways in COPD patients. Respiratory muscle impairment
842 RESPIRATORY CARE • AUGUST 2006 VOL 51 NO 8
MUSCLE DYSFUNCTION ASSOCIATED WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE
Fig. 2. Lung volume (percent of predicted total lung capacity [TLC])
in normal lungs (broken line) versus the lungs of a patient with
Fig. 1. Relationship between duty cycle (ratio of inspiratory time to chronic obstructive pulmonary disease (solid line). As ventilation
total-breathing-cycle time [TI/Ttot]) and critical transdiaphragmatic increases in the normal lungs (as with exercise), the tidal volume
pressure (ratio of the diaphragm pressure to the maximum dia- (lung-volume change) increases, but the end-expiratory volume
phragm pressure [Pdi/Pdi-max]) and development of respiratory mus- remains unchanged. In contrast, the lungs of the patient with chronic
cle fatigue. The dashed lines indicate the 95% confidence inter- obstructive pulmonary disease have an elevated end-expiratory
vals for the critical Pdi/Pdi-max. Fatigue develops with breathing lung volume, even at rest, and it increases further with increasing
patterns that fall to the right of the curve, but not for those that fall ventilation. An increase in tidal volume is thus made more difficult
to the left. This relationship can be mathematically represented by and the ventilatory impairment worsens with exercise. (From Ref-
the product of the TI/Ttot and the critical Pdi/Pdi-max, which is termed erence 67, with permission.)
the pressure-time index. Pressure-time index values above 0.15
fall to the right of the curve and predict fatigue. (From Reference
77, with permission.) cially right-ventricular dysfunction) and those with simple
skeletal-muscle deconditioning. Interestingly, 20% of our
directly limits exercise ventilation capability.6,64,78 In ad- total COPD population did not appear limited by any of
dition, exercise-induced wasted ventilation and early lactic these factors yet still complained of dyspnea and/or fatigue
acidosis in these patients further increases the exercise that prevented further exercise. One might speculate that
ventilation requirement and thus further worsens the load/ peripheral muscle factors might be playing a role in lim-
capability relationship in the respiratory muscles.45 Impor- iting many of these patients. Taken together, these data
tantly, the lung hyperinflation in COPD patients increases suggest that skeletal-muscle (both respiratory and limb)
with exercise, which further shortens the diaphragm and dysfunction contribute to substantial exercise limitation in
further compromises its force-generation capability during the majority of COPD patients.
exercise (Fig. 2).67 In the limb muscles, the structural and
metabolic abnormalities noted above lead to early lactic Approaches to Treatment
acidosis and task failure with exercise.58 – 61,79
In a large sample of COPD patients undergoing pulmo- There are a number of ways to address both the respi-
nary rehabilitation, we found that 25% of this population ratory and the systemic muscle dysfunction associated with
had primary ventilatory load/capability limitations to ex- COPD. Appropriate bronchodilator therapy reduces in-
ercise (ie, the ratio of required exercise ventilation to max- spiratory (and expiratory) loading and air trapping, which
imum voluntary ventilation exceeded 0.8).80 Another 18% increases ventilatory capability, improves oxygenation, and
of this population was limited by gas exchange (oxygen reduces load on the respiratory muscles.
saturation [measured via blood-gas analysis or pulse oxim- Exercise therapy is clearly beneficial in patients with
etry] fell below 88%), whereas 25% were primarily lim- COPD.45,81– 85 Lower-limb muscle exercise in particular
ited by the cardiovascular system (maximum heart rate has been shown in numerous studies and several meta-
was achieved). This cardiovascular group probably repre- analyses to increase muscle mass and increase functional
sents both patients with true cardiac dysfunction (espe- performance (Fig. 3). Both strength and endurance train-
RESPIRATORY CARE • AUGUST 2006 VOL 51 NO 8 843
MUSCLE DYSFUNCTION ASSOCIATED WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE
tilation increases rarely occur after pulmonary rehabilita-
tion, even though ventilatory efficiency is improved.83 Per-
haps the exercise ventilation these patients can generate
during limb exercise is simply insufficient to endurance
condition or train the respiratory muscles.
The data supporting strength training of respiratory mus-
cles using periods of high-resistive breathing are mixed.81,83
On one hand, respiratory muscles are chronically exposed
to high-resistive loads imposed by airway obstruction, so
further pressure loading might not be expected to provide
benefit. There are, however, clinical reports that the resis-
tive breathing reduces dyspnea and improves respiratory
muscle strength in some (but not all) patients.83 Current
recommendations suggest limiting respiratory muscle
strength training to only those patients with documented
respiratory muscle weakness.81
The role of oxygen in hypoxemic COPD patients seems
well established, as oxygen improves outcomes and re-
duces mortality90 and improves exercise performance in
hypoxemic patients.91–93 On the other hand, few data in-
Fig. 3. A summary and meta-analysis of trials that examined func-
dicate that oxygen improves long-term training effects in
tional changes after a formal exercise-training program for pa- these patients, and there are no data on whether oxygen in
tients with chronic obstructive pulmonary disease. The study re- between the exercise periods benefits nonresting hypox-
sults are represented by the black dots (mean values) and the emic patients. One interesting note about oxygen is that
horizontal bars (95% confidence intervals). Studies with results to there are several reports that supplemental oxygen during
the right of zero represent significant benefits from the exercise-
training program. This meta-analysis indicates significant func-
exercise, even in only borderline-hypoxemic patients,
tional benefit from the exercise intervention. (From Reference 82, seems to reduce exercise ventilation (presumably through
with permission.) reduced carotid-body output), which may allow a longer or
a higher training period in patients who are otherwise lim-
ited by ventilation.94
ing are effective, but have different effects.86 – 89 Strength There are 2 other approaches to building muscle mass:
training involves high-pressure loading of the muscles, nutrition and hormonal therapy. The American Thoracic
using such techniques as weight lifting or other “isomet- Society has recommended that caloric supplementation in-
ric” procedures. These tend to build more sarcomeres, es- tervention should be considered for the following condi-
pecially type II fibers. In contrast, endurance training in- tions: a body-mass index ⬍ 21 kg/m2, involuntary weight
volves motion loading of the muscles, using such techniques loss of ⬎ 10% during the last 6 months or ⬎ 5% in the
as cycling or walking. These tend to build oxidative and past month, or depletion of lean body mass.81 Caloric sup-
endurance capabilities in muscles, especially in type I fi- port should be based on activity level and the goal of
bers. In general, the higher the exercise training load, the restoring body weight.95–98 High-energy supplements may
better is the effect (Fig. 4).45 This is the rationale for the also be helpful. Adequate protein is essential to stimulate
recommendation that patients exercise as close to their muscle protein synthesis. Various hormonal approaches
maximum heart rate as possible during rehabilitation ses- have also been used to build muscle mass,99 –103 including
sions.81 anabolic steroids and growth hormones, and these are of-
Exercising (and thereby possibly conditioning or train- ten used in conjunction with exercise. In the short-term,
ing) respiratory muscles specifically is less well under- both drug classes increase muscle mass and exercise ca-
stood. Leith and Bradley87 found that isocapnic hyperven- pability, but there are important adverse effects (eg, fluid
tilation (motion work) can improve the maximum voluntary retention and altered glucose metabolism) and long-term
ventilation but not the maximum strength. In contrast, re- outcomes are not known. The progestational agent meges-
sistive breathing (pressure work) could improve maximum terol acetate stimulates appetite and weight gain in COPD
strength but not maximum voluntary ventilation. It would patients, but much of this weight gain is fat, and long-term
therefore stand to reason that increasing ventilation with functional outcome is unclear.
increasing limb exercise should improve diaphragmatic There are 2 surgical approaches to COPD: lung-vol-
endurance capabilities, although few data exist to support ume-reduction surgery (LVRS), and lung transplantation.
this concept. Indeed, significant maximum voluntary ven- LVRS reduces air trapping and improves ventilatory ca-
844 RESPIRATORY CARE • AUGUST 2006 VOL 51 NO 8
MUSCLE DYSFUNCTION ASSOCIATED WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE
Fig. 4. Changes in exercise-test results after exercise rehabilitation in patients with chronic obstructive pulmonary disease. The exercise
tests were performed before and after the exercise rehabilitation, using the same exercise work load, so decreases represent improved
function (less lactate development), lower ventilation requirement, lower oxygen need, lower carbon-dioxide production, and lower heart-
rate requirement. Patients in the left panel underwent a high-intensity exercise program; patients in the right panel underwent a less intense
exercise program. Though both the exercise programs improved function, the high-intensity program produced a greater effect. (From
Reference 45, with permission.)
pability and exercise performance in selected patients with ties and compromised oxygen delivery from right-heart
heterogeneous emphysema and who have large, over-in- dysfunction. In these patients, the chronic overloading of
flated lung regions that are amenable to resection.104 In- respiratory muscles leads to a risk of fatigue at low levels
terestingly, all the studies of LVRS have been done in of exercise, and this is made worse by hyperinflation. Im-
conjunction with rehabilitation programs that emphasize portantly, the overloaded respiratory muscles can structur-
aerobic training. Lung transplantation for COPD removes ally and metabolically adapt to a certain extent to restore
the chronic inflammatory state, reduces air trapping, and some functional capabilities. In the limb muscles of COPD
improves gas exchange. All of these should enhance skel- patients, chronic underloading leads to muscle atrophy.
etal muscle recovery and conditioning if aerobic training is Treatment is aimed at optimizing lung function, nutritional
part of the postoperative management. However, lung- repletion, oxygen therapy in the hypoxemic patient, and
transplant patients must stay on long-term immunosup- aerobic exercise training. LVRS may help with the hyper-
pression therapy and are at risk for repeated infections. inflation effects and improve gas exchange. Lung trans-
What role these may have in skeletal muscle function is plantation likewise should improve respiratory function
largely unknown. and allow more aerobic training, although the effects of
long-term immunosuppression and recurrent infection are
Summary unknown.
Skeletal muscle abnormalities are profound in patients
with chronic inflammatory states, including COPD. These REFERENCES
are caused by direct inflammatory-mediator effects on mus-
1. Burke RE. Motor units: anatomy, physiology and functional orga-
cle function, as well as malnutrition, drugs, and other co- nization. In: Peachey LD, editor. Handbook of physiology: the
morbid states. In the patient with COPD, skeletal muscle nervous system. Motor Control. Bethesda MD: Am Physiol Soc;
dysfunction is further worsened by blood-gas abnormali- 1981: 345–422.
RESPIRATORY CARE • AUGUST 2006 VOL 51 NO 8 845
MUSCLE DYSFUNCTION ASSOCIATED WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE
2. Ennion S, Sant’Ana Pereira J, Sargeant AJ, Young A, Goldspink G. 19. Jackson MJ, O’Farrell S. Free radicals and muscle damage. Br Med
Characterization of human skeletal muscle fibers according to the Bull 1993;49(3):630–641.
myosin heavy chains they express. J Muscle Res Cell Motil 1995; 20. Buck M, Chojkier M. Muscle wasting and dedifferentiation induced
16(1):35–43. by oxidative stress in a murine model of cachexia is prevented by
3. Hamm TM, Nemeth PM, Solanki L, Gordon DA, Reinking RM, inhibitors of nitric oxide synthesis and antioxidants. EMBO J 1996;
Stuart DG. Association between biochemical and physiological prop- 15(8):1753–1765.
erties in single motor units. Muscle Nerve 1988;11(3):245–254. 21. Llesuy S, Evelson P, Gonzalez-Flecha B, Peralta J, Carreras MC,
4. Henneman E, Mendell LM. Functional organization of motoneuron Poderoso JJ, Boveris A. Oxidative stress in muscle and liver of rats
pool and its inputs. In: Brookhart JM, Mountcastle VB, editors. with septic syndrome. Free Radic Biol Med 1994;16(4):445–451.
Handbook of physiology, Section I: The nervous system, Vol III, 22. Engelen MAM, Schols AMWJ, Baken WC, Wesseling GJ, Wouters
Part 1. Bethesda MD: Am Physiol Soc; 1981: 423–507. EF. Nutritional depletion in relation to respiratory and peripheral
5. Burke RE, Levine DN, Zajac FE 3rd. Mammalian motor units: skeletal muscle function in out-patients with COPD. Eur Respir J
physiological-histochemical correlation in three types in cat gas- 1994;7(10):1793–1797.
trocnemius. Science 1971;174(10):709–712. 23. Schols AM, Soeters PB, Dingemans AM, Mostert R, Frantzen PJ,
6. Begin P, Grassino A. Inspiratory muscle dysfunction and chronic Wouters EF. Prevalence and characteristics of nutritional depletion
hypercapnia in chronic obstructive pulmonary disease. Am Rev in patients with stable COPD eligible for pulmonary rehabilitation.
Respir Dis 1991;143(5 Pt 1):905–912. Am Rev Respir Dis 1993;147(5):1151–1156.
7. Ottenheijm CA, Heunks LM, Sieck GC, Zhan WZ, Jansen SM, 24. Kelsen SG, Ference M, Kapoor S. Effects of prolonged undernu-
Degens H, et al. Diaphragm dysfunction in chronic obstructive trition on structure and function of the diaphragm. J Appl Physiol
pulmonary disease. Am J Respir Crit Care Med 2005;172(2):200– 1985;58(4):1354–1359.
205. 25. Vaz M, Thangam S, Prabhu A, Shetty PS. Maximal voluntary con-
8. DeTroyer A, Pride NB. The chest wall and respiratory muscles in traction as a functional indicator of adult chronic undernutrition.
chronic obstructive pulmonary disease. In: Roussos Ch, editor. The Br J Nutr 1996;76(1):9–15.
thorax, Part C: Disease, 2nd ed. New York: Marcel Dekker; 1995: 26. Fiaccedori E, Zambrelli P, Tortorella G. [Physiopathology of re-
1975–2006. spiratory muscles in malnutrition.] Minerva Anestesiol 1995;61(3):
93–99. Article in Italian
9. Skeletal muscle dysfunction in chronic obstructive pulmonary dis-
27. Openbrier DR, Irwin MM, Rogers RM, Gottlieb GP, Dauber JH,
ease. A statement of the American Thoracic Society and European
Van Thiel DH, Pennock BE. Nutritional status and lung function in
Respiratory Society. Am J Respir Crit Care Med 1999;159(4 Pt
patients with emphysema and chronic bronchitis. Chest 1983;83(1):
2):S1–S40.
17–22.
10. Tiao G, Fagan JM, Samuels N, James JH, Hudson K, Lieberman M,
28. Mitch WE, Medina ER, Grieber S, May RC, England BK, Price SR,
et al. Sepsis stimulates nonlyosomal, energy-dependent proteolysis
et al. Metabolic acidosis stimulates muscle protein degradation by
and increases ubiquitin mRNA levels in rat skeletal muscle. J Clin
activating the adenosine triphosphate-dependent pathway involving
Invest 1994;94(6):2255–2264.
ubiquitin and proteasomes. J Clin Invest 1994;93(5):2127–2133.
11. Llovera M, Garcia-Martinez C, Agell N, Lopez-Soriano FJ, Argiles
29. Fiaccadori E, Coffrini E, Ronda N, Vezzani A, Cacciani G, Frac-
JM. TNF can directly induce the expression of ubiquitin-dependent
chia C, et al. Hypophosphatemia in course of chronic obstructive
proteolytic system in rat soleus muscles. Biochem Biophys Res
pulmonary disease: prevalence, mechanisms, and relationships with
Commun 1997;230(2):238–241.
skeletal muscle phosphorus content. Chest 1990;97(4):857–868.
12. Biolo G, Toigo G, Ciocchi B, Situlin R, Iscra F, Gullo A, Guarnieri
30. Knochel JP. Neuromuscular manifestations of electrolyte disorders.
G. Metabolic response to injury and sepsis: changes in protein Am J Med 1982;72(3):521–535.
metabolism. Nutrition 1997;13(9 Suppl):52S–57S. 31. Fiaccadori E, Coffrini E, Fracchia C, Rampulla C, Montagna T,
13. DiFrancia M, Barbier D, Mege JL, Orehek J. Tumor necrosis fac- Borghetti A. Hypophosphatemia and phosphorus depletion in re-
tor-alpha levels and weight loss in chronic obstructive pulmonary spiratory and peripheral muscles of patients with respiratory failure
disease. Am J Respir Crit Care Med 1994;150(5 Pt 1):1453–1455. due to COPD. Chest 1994;105(5):1392–1398.
14. deGodoy I, Donahoe M, Calhoun WJ, Mancino J, Rogers RM. 32. Stendig-Lindberg G, Bergstrom J, Hultman E. Hypomagnesaemia
Elevated TNF-␣ production by peripheral blood monocytes of and muscle electrolytes and metabolites. Acta Med Scand 1977;
weight-losing COPD patients. Am J Respir Crit Care Med 1996; 201(4):273–280.
153(2):633–637. 33. Sieck GC, Johnson BD. Metabolic and structural alterations in skel-
15. Schols AM, Buurman WA, Staal van den Brekel AJ, Dentener MA, etal muscle with hypoxia. In: Haddad GG, Lister G, editors. Tissue
Wouters EF. Evidence for a relation between metabolic derange- oxygen deprivation: from molecular to integrated function. New
ments and increased levels of inflammatory mediators in a sub- York: Marcel Dekker; 1996:779–827.
group of patients with chronic obstructive pulmonary disease. Tho- 34. Howald H, Pette D, Simoneau JA, Uber A, Hoppeler H, Cerretelli
rax 1996;51(8):819–824. P. Effect of chronic hypoxia on muscle enzyme activities. Int J Sports
16. Mitch WE, Goldberg AL. Mechanisms of muscle wasting: the role Med 1990;11 Suppl 1:S10–S14.
of the ubiquitin-proteasome pathway. N Engl J Med 1996;335(25): 35. Hultman E, Del Canale S, Sjoholm H. Effect of induced metabolic
1897–1905. acidosis on intracellular pH, buffer capacity and contraction force
17. Gosker HR, Kubat B, Schaart G, van der Vusse GJ, Wouters EF, of human skeletal muscle. Clin Sci (Lond) 1985;69(5):505–510.
Schols AM. Myopathological features in skeletal muscle of patients 36. Naeije R. Pulmonary hypertension and right heart failure in chronic
with chronic obstructive pulmonary disease. Eur Respir J 2003; obstructive pulmonary disease. Proc Am Thorac Soc 2005;2(1):20–
22(2):280–285. 22.
18. Agusti AG, Sauleda J, Miralles C, Gomez C, Togores B, Sala E, et 37. Wuyam B, Payen JF, Levy P, Bensaidane H, Reutenauer H, Le Bas
al. Skeletal muscle apoptosis and weight loss in chronic obstructive JF, Benabid AL. Metabolism and aerobic capacity of skeletal mus-
pulmonary disease. Am J Respir Crit Care Med 2002;166(4):485– cle in chronic respiratory failure related to chronic obstructive pul-
489. monary disease. Eur Respir J 1992;5(2):157–162.
846 RESPIRATORY CARE • AUGUST 2006 VOL 51 NO 8
MUSCLE DYSFUNCTION ASSOCIATED WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE
38. Dempsey JA, Harms CA, Ainsworth DM. Respiratory muscle per- 59. Hamilton AL, Killian KJ, Summers E, Jones NL. Muscle strength,
fusion and energetics during exercise. Med Sci Sports Exerc 1996; symptom intensity, and exercise capacity in patients with cardio-
28(9):1123–1128. respiratory disorders. Am J Respir Crit Care Med 1995;152(6 Pt
39. Harms CA, Babcock MA, McClaran SR, Pegelow DF, Nickele GA, 1):2021–2031.
Nelson WB, Dempsey JA. Respiratory muscle work compromises 60. Bernard S, LeBlanc P, Whittom F, Carrier G, Jobin J, Belleau R,
leg blood flow during maximal exercise. J Appl Physiol 1997; Maltais F. Peripheral muscle weakness in patients with chronic
82(5):1573–1583. obstructive pulmonary disease. Am J Respir Crit Care Med 1998;
40. Wittenberg B, Wittenberg J, Caldwell P. Role of myoglobin in the 158(2):629–634.
oxygen supply to red skeletal muscle. J Biol Chem 1975;250(23): 61. Serres I, Gautier V, Varray AL, Prefaut C. Impaired skeletal muscle
9038–9043. endurance related to physical inactivity and altered lung function in
41. Moller P, Hellstrom K, Hermansson IL. Myoglobin content in leg COPD patients. Chest 1998;113(4):900–905.
skeletal muscle in patients with chronic obstructive lung disease. 62. Booth FW, Gollnick PD. Effects of disease on the structure and
Respiration 1984;45(1):35–38. function of skeletal muscle. Med Sci Sports Exerc 1983;15(5):415–
42. Enad JG, Fournier M, Sieck GC. Oxidative capacity and capillary 420.
density of diaphragm motor units. J Appl Physiol 1989;67(2):620– 63. Coyle EF, Martin WH 3rd, Bloomfield SA, Lowry OH, Holloszy
627. JO. Effects of detraining on responses to submaximal exercise.
43. Westerblad H, Lee JA, Lannergren J, Allen DG. Cellular mecha- J Appl Physiol 1985;59(3):853–859.
nisms of fatigue in skeletal muscle. Am J Physiol 1991;261(2 Pt 64. Levison H, Cherniack RM. Ventilatory cost of exercise in chronic
1):C195–C209. Erratum in: Am J Physiol 1991;261(4 Pt 1):follow- obstructive pulmonary disease. J Appl Physiol 1968;25(1):21–27.
ing. 65. MacIntyre NR, Leatherman NE. Mechanical loads on the ventila-
44. Reid MB. Muscle fatigue: mechanisms and regulation. In: Sen CK, tory muscles: a theoretical analysis. Am Rev Respir Dis 1989;
Packer L, Hanninen O, editors. Exercise and oxygen toxicity, 2nd 139(4):968–973.
ed. Amsterdam: Elsevier Science, 1998. 66. Similowski T, Yan S, Gauthier AP, Macklem PT, Bellemare F.
45. Casaburi R, Patessio A, Ioli F, Zanaboni S, Donner CF, Wasserman Contractile properties of the human diaphragm during chronic hy-
K. Reductions in exercise lactic acidosis and ventilation as a result perinflation. N Engl J Med 1991;325(13):917–923.
of exercise training in patients with obstructive lung disease. Am 67. O’Donnell DE. Exercise limitation and clinical exercise testing in
Rev Respir Dis 1991;143(1):9–18. chronic obstructive pulmonary disease. In: Weisman IM, Zeballos
46. Kwast KE, Hand SC. Acute depression of mitochondrial protein RJ, editors. Progress in respiratory research. Vol 32: Clinical ex-
synthesis during anoxia: contributions of oxygen sensing, matrix ercise testing. Basel: Karger; 2002: 138–158.
acidification, and redox state. J Biol Chem 1996;271(13):7313– 68. Levine S, Gregory C, Nguyen T, Shrager J, Kaiser L, Rubinstein N,
7319. Dudley G. Bioenergetic adaptation of individual human diaphrag-
47. Eldridge FL. Central integration of mechanisms in exercise hyper- matic myofibers to severe COPD. J Appl Physiol 2002;92(3):1205–
pnea. Med Sci Sports Exerc 1994;26(3):319–327. 1213.
48. Kavanagh BP. Therapeutic hypercapnia: careful science, better tri- 69. Lenine S, Kaiser L, Leferovich J, Tikunov B. Cellular adaptations
als (editorial). Am J Respir Crit Care Med 2005;171(2):96–97. in the diaphragm in chronic obstructive pulmonary disease. N Engl
49. Bangsbo J, Madsen K, Kiens B, Richter EA. Effect of muscle J Med 1997;337(25):1799–1806.
acidity on muscle metabolism and fatigue during intense exercise in 70. Levine S, Nguyen T, Kaiser LR, Rubinstein NA, Maislin G, Greg-
man. J Physiol 1996;495(Pt 2):587–596. ory C, et al. Human diaphragm remodeling associated with chronic
50. Karlsson J, Diamant B, Folkers K. Exercise-limiting factors in re- obstructive pulmonary disease: clinical implications. Am J Respir
spiratory distress. Respiration 1992;59 Suppl 2:18–23. Crit Care Med 2003;168(6):706–713.
51. Gertz I, Hedenstierna G, Hellers G, Wahren J. Muscle metabolism 71. Sheel AW, Derchak PA, Pegelow DF, Dempsey JA. Threshold
in patients with chronic obstructive lung disease and acute respi- effects of respiratory muscle work on limb vascular resistance.
ratory failure. Clin Sci Mol Med 1977;52(4):396–403. Am J Physiol Heart Circ Physiol 2002;282(5):H1732–H1738.
52. MacIntyre NR. Corticosteroids and chronic obstructive lung dis- 72. Ottenheijm CA, Heunks LM, Hafmans T, van der Ven PF, Benoist
ease. Respir Care 2006;51(3):289–296. C, Zhou H, et al. Titin and diaphragm dysfunction in chronic ob-
53. Decramer M, Lacquet LM, Fagard R, Rogiers P. Corticosteroids structive pulmonary disease. Am J Respir Crit Care Med 2006;
contribute to muscle weakness in chronic airflow obstruction. Am J 173(5):527–534.
Respir Crit Care Med 1994;150(1):11–16. 73. Vollestad NK. Measurement of human muscle fatigue. J Neurosci
54. Decramer M, de Bock V, Dom R. Functional and histologic picture Methods 1997;74(2):219–227.
of steroid-induced myopathy in chronic obstructive pulmonary dis- 74. Merton PA. Voluntary strength and fatigue. J Physiol 1954;123(3):
ease. Am J Respir Crit Care Med 1996;153(6 Pt 1):1958–1964. 553–564.
55. Hall-Angeras M, Angeras U, Zamir O, Hasselgren PO, Fischer JE. 75. Gandevia SC, Allen GM, McKenzie DK. Central fatigue: critical
Interaction between corticosterone and tumor necrosis factor stim- issues, quantification and practical implications. Adv Exp Med Biol
ulated protein breakdown in rat skeletal muscle, similar to sepsis. 1995;384:281–294.
Surgery 1990;108(2):460–466. 76. Roussos CS, Macklem PT. Diaphragmatic fatigue in man. J Appl
56. Larsson L, Ansved T, Edstrom L, Gorza L, Schiaffino S. Effects of Physiol 1977;43(2):189–197.
age on physiological, immunohistochemical and biochemical prop- 77. Bellemare F, Grassino A. Evaluation of human diaphragm fatigue.
erties of fast-twitch single motor units in the rat. J Physiol 1991; J Appl Physiol 1982;53(5):1196–1206.
443:257–275. 78. Polkey MI, Kyroussis D, Hamnegard CH, Mills GH, Green M,
57. Grimby G, Saltin B. The aging muscle. Clin Physiol 1983;3(3): Moxham J. Diaphragm strength in chronic obstructive pulmonary
209–218. disease. Am J Respir Crit Care Med 1996;154(5):1310–1317.
58. Gosselink R, Troosters T, Decramer M. Peripheral muscle weak- 79. Troosters T, Gosselink R, Rollier H. Change in lower limb muscle
ness contributes to exercise limitation in COPD. Am J Respir Crit strength contributes to altered six minute walking distance in COPD
Care Med 1996;153(3):976–980. (abstract). Eur Respir J Suppl 1996;9:144S.
RESPIRATORY CARE • AUGUST 2006 VOL 51 NO 8 847
MUSCLE DYSFUNCTION ASSOCIATED WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE
80. Plankeel JF. McMullen B. MacIntyre NR. Exercise outcomes after 93. Jakobsson P, Jorfeldt L. Long-term oxygen therapy may improve
pulmonary rehabilitation depend on the initial mechanism of exer- skeletal muscle metabolism in advanced chronic obstructive pul-
cise limitation among non-oxygen-dependent COPD patients. Chest monary disease patients with chronic hypoxaemia. Respir Med 1995;
2005;127(1):110–116. 89(7):471–476.
81. American Thoracic Society and European Respiratory Society. Ev- 94. Porszasz J, Emtner M, Goto S, Somfay A, Whipp BJ, Casaburi R.
idence based guidelines for pulmonary rehabilitation. Am J Respir Exercise training decreases ventilatory requirements and exercise-
Crit Care Med (2006, in press) induced hyperinflation at submaximal intensities in patients with
82. Lacasse Y. Wong E. Guyatt GH. King D, Cook DJ, Goldstein RS. COPD. Chest 2005;128(4):2025–2034.
Meta-analysis of respiratory rehabilitation in chronic obstructive 95. Ferriera IM, Brooks D, Lacasse Y, Goldstein RS. Nutritional sup-
pulmonary disease. Lancet 1996;348(9034):1115–1119. port for individuals with COPD: a meta-analysis. Chest 2000;117(3):
83. American College of Chest Physicians; American Association of 672–678.
Cardiovascular and Pulmonary Rehabilitation. Pulmonary rehabil- 96. Whittaker JS, Ryan CF, Buckley PA, Road JD. The effects of
itation: joint ACCP/AACVPR evidence-based guidelines. ACCP/ refeeding on peripheral and respiratory muscle function in malnour-
AACVPR Pulmonary Rehabilitation Guidelines Panel. Chest 1997; ished chronic obstructive pulmonary disease patients. Am Rev Re-
112(5):1363–1396. spir Dis 1990;142(2):283–288.
84. Sala E, Roca J, Marrades RM, Alonso J, Gonzalez De Suso JM, 97. Rogers RM, Donahoe M, Costantino J. Physiologic effects of oral
Moreno A, et al. Effects of endurance training on skeletal muscle supplemental feeding in malnourished patients with chronic ob-
bioenergetics in chronic obstructive pulmonary disease. Am J Re- structive pulmonary disease: a randomized control study. Am Rev
spir Crit Care Med 1999;159(6):1726–1734. Respir Dis 1992;146(6):1511–1517.
85. Maltais F, LeBlanc P, Simard C, Jobin J, Berube C, Bruneau J, et 98. Schols AMWJ, Slangen J, Volovics L, Wouters EF. Weight loss is
al. Skeletal muscle adaptation to endurance training in patients with a reversible factor in the prognosis of chronic obstructive pulmo-
chronic obstructive pulmonary disease. Am J Respir Crit Care Med nary disease. Am J Respir Crit Care Med 1998;157(6 Pt 1):1791–
1996;154(2 Pt 1):442–447. 1797.
86. Fitts RH, McDonald KS, Schluter JM. The determinants of skeletal 99. Yeh SS, DeGuzman B, Kramer T; M012 Study Group. Reversal of
muscle force and power: their adaptability with changes in activity COPD-associated weight loss using the anabolic agent oxandrolone.
pattern. J Biomech 1991;24 Suppl 1:111–122. Chest 2002;122(2):421–428.
87. Leith DE. Bradley M. Ventilatory muscle strength and endurance 100. Schols AM, Soeters PB, Mostert R, Pluymers RJ, Wouters EF.
training. J Appl Physiol 1976;41(4):508–516. Physiologic effects of nutritional support and anabolic steroids in
88. Bernard S, Whittom F, Leblanc P, Jobin J, Belleau R, Berube C, et patients with chronic obstructive pulmonary disease: a placebo-
al. Aerobic and strength training in patients with chronic obstruc- controlled randomized trial. Am J Respir Crit Care Med 1995;152(4
tive pulmonary disease. Am J Respir Crit Care Med 1999;159(3): Pt 1):1268–1274.
896–901. 101. Casaburi R, Bhasin S, Cosentino L, Porszasz J, Somfay A, Lewis
89. Casaburi R, Porszasz J, Burns MR, Carithers ER, Chang RS, Coo- MI, et al. Effects of testosterone and resistance training in men with
per CB. Physiologic benefits of exercise training in rehabilitation of chronic obstructive pulmonary disease. Am J Respir Crit Care Med
patients with severe chronic obstructive pulmonary disease. Am J 2004;170(8):870–878.
Respir Crit Care Med 1997;155(5):1541–1551. 102. Burdet L, de Muralt B, Schutz Y, Pichard C, Fitting JW. Admin-
90. Nocturnal Oxygen Therapy Trial Group. Continuous or nocturnal istration of growth hormone to underweight patients with chronic
oxygen therapy in hypoxemic chronic obstructive lung disease: a obstructive pulmonary disease. A prospective, randomized, con-
clinical trial. Ann Intern Med 1980;93(3):391–398. trolled study. Am J Respir Crit Care Med 1997;156(6):1800–1806.
91. Payen JF, Wuyam B, Levy P, Reutenauer H, Stieglitz P, Paramelle 103. Weisberg J, Wanger J, Olson J, Streit B, Fogarty C, Martin T,
B, Le Bas JF. Muscular metabolism during oxygen supplementa- Casaburi R. Megestrol acetate stimulates weight gain and ventila-
tion in patients with chronic hypoemia. Am Rev Respir Dis 1993; tion in underweight COPD patients. Chest 2002;121(4):1070–1078.
147(3):592–598. 104. Fishman A, Martinez F, Naunheim K, Piantadosi S, Wise R, Ries
92. Cotes JE, Gilson JC. Effect of oxygen on exercise ability in chronic A, et al. A randomized trial comparing lung-volume-reduction sur-
respiratory insufficiency: use of portable apparatus. Lancet 1956; gery with medical therapy for severe emphysema. N Engl J Med
270(6928):872–876. 2003;348(21):2059–2073.
Discussion MacIntyre: It’s a fascinating ques- trol. And I’d let them try to trigger as
tion. I struggle back and forth as to much as possible, if for no other rea-
what to do with an acutely overloaded son than to keep the muscles stimu-
Mehta: I am interested in patients
respiratory muscle system, and I’m not lated and performing at least some con-
with COPD who present with acute yet sure what the best way is. We tend traction.
respiratory failure. You said that con- to put them on a high level of support After the first 24 to 48 hours, and
trolled ventilation is probably not the initially—sometimes controlled me- with stabilization of the lung injury, I
right approach, because it could lead chanical ventilation—the idea being think providing some additional load-
to further atrophy of the respiratory that these muscles have really been ing makes some sense—ideally a near-
muscles. You want to challenge the beaten and battered and we need to normal kind of workload is probably
respiratory muscles a bit, without unload them. So I start with a fairly the right way to go. Now the obvious
overloading them, so how do you high level of support—though I question is, how in the heck do you
titrate ventilator support in the ab- wouldn’t use intermittent mandatory figure out what a near-normal work-
sence of esophageal-pressure mea- ventilation on them—a high level of load is? You can insert an esophageal
surements? either volume- or pressure-assist con- balloon and measure the patient work,
848 RESPIRATORY CARE • AUGUST 2006 VOL 51 NO 8
MUSCLE DYSFUNCTION ASSOCIATED WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE
as you and probably others here have with acute respiratory failure? The di- cles. Breathing through a T-piece for
done. But I think that you can do it aphragm has a very high oxygen con- an hour or two is still an attempt to
without such a monitor, by simply sumption, and often in respiratory fail- recondition the muscles.
looking at the patient. The patient’s ure there is an ATP [adenosine
own sensors, which Josh Benditt de- triphosphate] or oxygen deficit. I’ve MacIntyre: You’re right, although
scribed,1 are actually pretty good load read that, not so much in COPD but in I look at the spontaneous breathing
indicators. other conditions, it can take 24 to 48 trial more as an assessment than as a
If you get the patient on a level of hours to restore the ATP reserves, so weaning technique. Maybe I’m just ar-
ventilatory support where they’re com- we’re doing them a disservice if we guing semantics here. What I was try-
fortable, they’re triggering and in syn- push them very hard at the beginning. ing to get across is that when I used to
chrony with the ventilator, the respi- How do you decide clinically how to make rounds and I saw a patient on
ratory rate is not particularly high, ventilate them? pressure-support of, say, 16 cm H2O,
they’re not diaphoretic, and they’re not I would say, “Let’s go to 14 cm H2O.”
fighting the ventilator, then that’s MacIntyre: Geeta, you’re exactly Today I’m not sure that’s worth the
probably where you want to be. I’m right. I think a high level of support, trouble. I think you need to assess the
sorry I have to leave this conference particularly over the first 24 to 48 patient every day, but in between the
early and will miss the discussion hours, is important. But I don’t think assessments I think it makes more
about trying to gradually reduce sup- controlled ventilation is where we sense to leave them where they are,
port and increase loading versus sim- want to be. Perhaps that’s more opin- with some comfortable, near-normal
ply leaving the patient alone on a com- ion than evidence-based, but I like the kind of load pattern.
fortable interactive ventilatory support idea that the patient is still at least
mode (weaning versus not-weaning). getting a neural stimulus on the dia- Jubran: The problem is that we
I admit that I used to be a real phragm, and having some contrac- don’t know what is the ideal load for
“weaner” (some say I still am); I was tions, even though it’s a very unloaded a patient on the ventilator in the in-
turning the knobs daily— hourly contraction. Amal, please chirp in here,
tensive care unit. What Neil is sug-
even!—trying to get this or that level because I don’t want to be blindsided
down. As I get older and more crotch- gesting is probably all we can do at
by your paper tomorrow.
ety, I’ve come to believe that maybe this stage; that is, “eyeball” the pa-
all this knob-twirling really isn’t worth tient and see how much work they
Jubran: I agree with Neil that pa-
the trouble. The available evidence appear to be doing. Alternatively, we
tients should not receive controlled
does not support knob-twirling over can insert an esophageal catheter and
ventilation.
simple stable ventilator settings and measure patient effort.
daily spontaneous breathing trials, in The problem is that when we get
MacIntyre: Yeah!
terms of improving outcomes. Yes, I a number for pressure-time product,
want to put them on an assisted mode. Jubran: Tomorrow I will present our index of patient effort, we don’t
Yes, I want them to be doing some- data from animal studies that show know how to interpret it. We can
thing. But rather than trying to adjust that ventilator-induced diaphragmatic compare it to that of a normal per-
that load on an hourly or some other dysfunction occurs during controlled son. For example, we know that a
regular basis, maybe you should just mechanical ventilation. So I agree with pressure-time product of
leave them alone and do a daily spon- Neil that we should use an assisted 100 cm H2O 䡠 s/L is a value reported
taneous breathing trial to see where ventilation mode, even during the first for normals. But is that the target we
they are. 24 hours of initiating ventilation. You should aim for in patients? Or should
want the patient to trigger the venti- we aim for a lower or higher value?
lator; you want them to do a little bit Is the target different for patients
REFERENCE
of work. with COPD than for those with acute
1. Benditt JO. The neuromuscular respiratory respiratory distress syndrome? We
To follow up on what Neil said,
system: physiology, pathophysiology, and
that he’s not a “weaner,” I disagree simply don’t know.
a respiratory care approach to patients. Re-
spir Care 2006;51(8):829–837. with that statement. Neil is still “wean- On another subject, regarding
ing” patients from the ventilator. Daily lung-volume-reduction surgery
Hill: Sounds like you’re describing spontaneous breathing trials are a form [LVRS]? Were you surprised by the
noninvasive ventilation. of weaning. The purpose of a weaning negative results of the NETT [Na-
trial is to reload the respiratory mus- tional Emphysema Treatment Trial],
Mehta: Can we talk more about that cles for a brief period, as a way of that mortality did not decrease with
first day when the patient comes in reconditioning the respiratory mus- LVRS?1
RESPIRATORY CARE • AUGUST 2006 VOL 51 NO 8 849
MUSCLE DYSFUNCTION ASSOCIATED WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE
REFERENCE in the medical arm died, so at 5 years MacIntyre: I’m not sure it is pos-
1. Fishman A, Martinez F, Naunheim K, Pi- the study is now apparently positive. sible, because these patients are al-
antadosi S, Wise R, Ries A, et al; National But, as Neil said, there is a subgroup most universally “contaminated” with
Emphysema Treatment Trial Research of patients who does much better. I steroid therapy, so sorting those out
Group. A randomized trial comparing lung- think the reason for that is that there could be quite problematic.
volume-reduction surgery with medical
therapy for severe emphysema. N Engl
are a lot of effects from LVRS. It would
J Med 2003;348(21):2059–2073. be great if we could just reduce the Deem: Are there any animal-model
volume, and have the effect on the studies that help?
MacIntyre: I should ask Josh Ben- breathing muscles, which I think there
ditt for help on this, since he was also is, without affecting the pulmonary MacIntyre: Animal models of em-
one of the investigators, along with vasculature or other parts of lung func- physema are always kind of short-term
my institution. Now that it’s all said tion, because I think that it has a lot of things. They throw elastase down the
and done, I’m not surprised. There was effects, some of which are not neces- trachea, create an injury, and then
a subgroup of patients who did ex- sarily good. For instance, there are peo- study them over a matter of weeks
tremely well with LVRS. These were ple who develop hypertension after and months. Yes, you can see muscle
patients with very obvious heteroge- LVRS. effects of the systemic inflammation
neous emphysema, primarily if it was independent of the corticosteroids, but
upper-lobe predominant, and who it’s hard to sort those out.1
were very disabled. And that would REFERENCE
make some sense. These are horribly REFERENCE
1. Naunheim KS, Wood DE, Krasna MJ, De-
hyperinflated patients, and LVRS re- Camp MM Jr, Ginsburg ME, McKenna RJ 1. MacIntyre NR. Corticosteroids and chronic
lieves the over-inflation, which puts Jr, et al; National Emphysema Treatment obstructive lung disease. Respir Care 2006;
the diaphragm in a better position. Trial Research Group. Predictors of oper- 51(3):289–296.
And, sure enough, those patients’ mor- ative mortality and cardiopulmonary mor-
tality, exercise tolerance, and quality bidity in the National Emphysema Treat- Mehta: What’s the drive for this
ment Trial. J Thorac Cardiovasc Surg 2006;
of life were improved by LVRS. chronic inflammatory state? Is it hy-
131(1):43–53.
Now, having said that, those patients poxemia, hypercapnia? Can you dis-
were a small minority of the patients tinguish between those 2 populations?
Jubran: For whom would you rec-
who were studied, and you’re quite Is one more inflammatory than the
ommend surgery?
right that most of the patients did not other? Is it intercellular acidosis?
see those kinds of results. Indeed, in
Benditt: We have a little group of
some patient groups, LVRS actually MacIntyre: Well, you’re getting
surgeons and pulmonologists who re-
gave worse results, which, in the mid- into the pathogenesis of COPD. It’s a
view each case that comes up for that.
dle of the trial, prompted taking out chronic inflammatory state of the air-
We suggest surgery for those individ-
those patients from being further ran- ways, potentiated by external stimuli
domized. These were the patients with uals with upper lobe emphysema and (ie, tobacco smoke), repeated infec-
homogenous emphysema and really low exercise capacity. This was the tions, perhaps environmental factors
bad lung function. subgroup that showed clear benefit. involving multiple cells, the CD-8
LVRS is not for everybody. But I We certainly have not been recom- family of lymphocytes, macrophages,
think now that if we go back and think mending it for people with homoge- neutrophils. I’m not sure I can sepa-
about this, we probably saw what neous disease or very severe disease. rate all those things out. Rajiv, you’ve
should have been expected. The pa- And with those other people, who are done a lot of work in this area.
tients who should get LVRS are those kind of in the middle, we have not
with grossly regional over-inflation been pushing them in any way, and Rajiv Dhand: We do studies on ela-
that’s easy to get at surgically, and the actually try to avoid it. stase-induced emphysema, and one of
potential to reduce the over-inflation. the things that we are really intrigued
Josh, do you have anything to add to Deem: Neil, I was interested in your by is that we give a single instillation
that? comment on how systemic inflamma- of elastase, and then we sacrifice the
tion may affect skeletal muscle in animals after 7 days, 14 days, or 21
Benditt: A recent paper by Naun- COPD, because corticosteroids have days. We’ve found that there’s a pro-
heim et al1 found that at 5 years the similar effects on muscle proteolysis. gressive increase in the amount of em-
mortality for the overall group was Is it possible to separate out the ef- physema that’s produced, so a single
actually lower in the LVRS group. fects of inflammation from corticoste- instillation leads to a sort of repetitive
That is, as time went on, more people roids in those patients? injury, and it’s very intriguing what is
850 RESPIRATORY CARE • AUGUST 2006 VOL 51 NO 8
MUSCLE DYSFUNCTION ASSOCIATED WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE
the source of that injury. One of the of retraining of the other diaphragm, It’s always been my concept, and
possibilities is that this is the release and the tidal volumes remained flat, my argument to the house staff, that
of elastin fragments that causes im- no matter what stimulus we used. we need not necessarily wean levels
mune-mediated injury to the lung. So it appeared that a mere 30 min- of pressure support—that, in fact,
utes a day of stimulation preserved we’re using those periods that we eu-
Brown: Neil, with regard to wean- the function of that hemidiaphragm. It phemistically refer to as “sprints” as
ing, I think you made one error. You’re makes you wonder whether diaphragm exercise periods for those children, and
not getting older and more crotchety, atrophy occurs in our intensive-care- then allow them to rest once they’re
you’re getting older and wiser! unit patients. We know that even when back on ventilatory support. Am I to-
they’re ventilated they contract their tally off the wall?
MacIntyre: I can only hope! diaphragms, and it appears that it
doesn’t take much to preserve dia- MacIntyre: How long are your
Brown: With regard to diaphragm phragmatic function. sprints?
dysfunction in these various disorders,
another approach to take would be to Panitch: They can go hours.
REFERENCE
ask the question, how much stimula-
tion does the diaphragm require to 1. Ayas NT, McCool FD, Gore R, Lieberman MacIntyre: I said I’m no longer a
avoid atrophy? We have published one SL, Brown R. Prevention of human dia-
phragm atrophy with short periods of elec-
“weaner” in the intensive care unit,
sort of anecdotal paper in that regard.1 trical stimulation. Am J Respir Crit Care but I want to differentiate the inten-
We had a patient years ago who Med 1999;159(6):2018–2020. sive-care-unit population from the pa-
had bilateral diaphragm dysfunction tients who require prolonged mechan-
from C1–C2 neurologically complete MacIntyre: I would agree that it ical ventilation and patients who
tetraplegia, and he had bilateral may not be very much, but it’s gotta require more than 21 days of support.
phrenic pacemakers, one of which got be something. If you put them down The patients might be quite different
infected and had to be removed. The completely, so that they’re not doing in the world of long-term assisted care
red tape at the hospital led to 3 months anything, that could lead to diaphragm and long-term acute care facilities,
before a new pacemaker could be ob- dysfunction. I think Amal Jubran’s go- where patients are on ventilators for
tained for him, and during that 3 ing to discuss that issue more tomor- weeks or months. In that population—
months we stimulated the intact hemi- row. though it hasn’t been studied in a ran-
diaphragm for 30 minutes a day, with domized controlled trial—the results
a phrenic-nerve pacemaker. Then af- Brown: I agree completely. I just from multiple observational trials ar-
ter 3 months, when the new pacemak- suspect that it doesn’t take much. gue strongly that the kind of weaning
ers were put in, we monitored the tidal strategy you just mentioned makes
volume and diaphragm thickness on MacIntyre: Doesn’t take much; that sense. Almost universally, those cli-
the side that had been stimulated for may be true. nicians use progressive reduction of
30 minutes a day, and on the side that
support, at least initially. However, al-
had not been stimulated at all for 3 Panitch: In infant and toddler pedi- most every one of them, when they
months. atrics, the analogy to COPD is bron- get to a certain level of support— be
What we found was the typical out- chopulmonary dysplasia. We fre-
it 30% or 50% of total support—they’ll
come—that with retraining the dia- quently take care of infants who
start doing spontaneous breathing tri-
phragm that had not been stimulated require prolonged mechanical ventila-
als for ventilator-discontinuation as-
developed larger and larger and larger tory support, and our practice, typi-
sessment. So maybe there is a role for
tidal volumes at a given stimulus in- cally, is to give them at least a low
that kind of weaning with more long-
tensity, and then reached a plateau. rate of mandatory breaths and allow
term patients.1
That diaphragm hypertrophied. The them to breathe spontaneously with
evidence for that was that it got thicker pressure-support. And then in the pro-
and thicker; we were able to estimate cess of liberating them from support,
REFERENCE
its thickness with ultrasonographic we use longer and longer periods of
techniques. On the other hand, the di- time off mechanical ventilation. In ad- 1. MacIntyre NR, Epstein SK, Carson S,
aphragm that had been stimulated for dition to worrying about gas exchange, Scheinhorn D, Christopher K, Muldoon S,
National Association for Medical Direction
only 30 minutes a day, albeit via elec- we also have to worry about growth
of Respiratory Care. Management of pa-
trophrenic stimulation, probably en- and development in these children, and tients requiring prolonged mechanical ven-
gaging all of the fibers, did not in- that often dictates the speed with which tilation: report of a NAMDRC consensus
crease in thickness during the period we can withdraw support. conference. Chest 2005;128(6):3937–3954.
RESPIRATORY CARE • AUGUST 2006 VOL 51 NO 8 851
MUSCLE DYSFUNCTION ASSOCIATED WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE
Lechtzin: I have a question about Panitch: Hayot et al1 looked at the REFERENCES
peripheral muscle involvement. I’ve tension-time index of children with 1. Garrod R, Mikelsons C, Paul EA, Wedzicha
seen literature1–3 on relatively young cystic fibrosis who had mild-to-mod- JA. Randomized controlled trial of domi-
patients with cystic fibrosis who have erate obstructive disease but were ciliary noninvasive positive pressure ven-
reasonably good lung function, who clearly abnormal, compared with tilation and physical training in severe
are still active (compared to age- healthy controls. It seemed that the chronic obstructive pulmonary disease.
matched controls); they have fairly diaphragm may not be working as well, Am J Respir Crit Care Med 2000;162(4 Pt
1):1335–1341.
pronounced arm and leg weakness, but even in children with mild-to-moder-
2. Bianchi L, Foglio K, Pagani M, Vitacca M,
still have preserved abdominal-mus- ate obstructive disease. Rossi A, Ambrosino N. Effects of propor-
cle strength, presumably because tional-assist ventilation on exercise toler-
they’ve had a daily cough all their lives REFERENCE ance in COPD patients with chronic hyper-
and therefore use their abdominal mus- 1. Hayot M, Guillaumont S, Ramonatxo M, capnia. Eur Respir J 1998;11(2):422–427.
cles so much. I don’t know if there’s Voisin M, Prefaut C. Determinants of the
similar literature on COPD patients, tension-time index of inspiratory muscles MacIntyre: Both of those concepts
in children with cystic fibrosis. Pediatr Pul- make some sense. The nocturnal strat-
but I wonder what implications this
monol 1997;23(5):336–343.
has for strength training in those pa- egy, however, is a little confusing to
tients, and should we be starting re- me. It is unclear whether unloading
Hill: Regarding rehabilitation and
habilitation much earlier than we typ- the muscles at night translates into an
what limits exercise capacity, you
ically do with these patients? outcome benefit during the day, as you
showed some data that suggested there
are probably several mechanisms that know better than any of us. Some stud-
REFERENCES contribute to functional-exercise- ies suggest that can happen, 1 but
capacity limitation in these patients, what’s sort of depressing is that in
1. Pinet C, Scillia P, Cassart M, Lamotte M, those studies the patients generally
Knoop C, Melot C, Estenne M. Preferential and it probably varies from patient to
reduction of quadriceps over respiratory patient, and maybe over time within chose not to continue using the device
muscle strength and bulk after lung trans- individual patients. Investigators have at night. So whatever benefit they got
plantation for cystic fibrosis. Thorax 2004; taken different approaches to how to wasn’t enough for them to think that
59(9):783–789. it was a good idea to continue.
2. Pinet C, Cassart M, Scillia P, Lamotte M,
deal with the respiratory-muscle con-
Knoop C, Casimir G, et al. Function and tribution, and one, of course, is mus- Regarding exercising with the ven-
bulk of respiratory and limb muscles in pa- cle training, and you showed some of tilator, I find that a very interesting
tients with cystic fibrosis. Am J Respir Crit that data. It doesn’t look terribly help- idea. I showed data on using oxygen
Care Med 2003;168(8):989–994. ful in improving function. to reduce the ventilatory load. It
3. Sahlberg ME, Svantesson U, Thomas EM,
Strandvik B. Muscular strength and func-
But another tack that you didn’t would be logical to extrapolate that
tion in patients with cystic fibrosis. Chest mention was noninvasive ventilation, to a mechanical device that could
2005;127(5):1587–1592. and there are a couple of studies, rep- somehow be rigged up to help you
resenting 2 different approaches; one during your exercise. You could
MacIntyre: If you’re asking me was by Garrod et al.1 They used non- hardly do it walking, but perhaps dur-
whether rehabilitation should be done invasive ventilation just for 2 hours at ing cycling or on a treadmill. It makes
sooner rather than later, I would sup- night and found a significant improve- some sense.
port “sooner” 100%. I think it’s silly ment in exercise capacity, measured
to wait for somebody to be horribly with the shuttle walk test. And the other
disabled before they finally go into a approach is to use noninvasive venti- REFERENCE
rehabilitation program. The time to lation during exercise.2 The idea was
1. Clinical indications for noninvasive posi-
start is at the earliest stages of func- that by permitting patients to exercise
tive-pressure ventilation in chronic respira-
tional impairment. What you said at a greater rate, noninvasive ventila- tory failure due to restrictive lung disease,
about cough is intriguing. I wasn’t tion would enhance the training effect COPD, and nocturnal hypoventilation: a
aware of that. That’s quite interesting, on peripheral muscles. What are your consensus conference report. Chest 1999;
and it makes sense. thoughts on these approaches? 116(2):521–534.
852 RESPIRATORY CARE • AUGUST 2006 VOL 51 NO 8
You might also like
- Principles of Exercise PhysiologyDocument8 pagesPrinciples of Exercise PhysiologyDaniel PachecoNo ratings yet
- Muscular System ReviewerDocument10 pagesMuscular System ReviewerGaille DacilloNo ratings yet
- US Army Medical Course MD0753-101 Book2 - Medical Records Administration BranchDocument101 pagesUS Army Medical Course MD0753-101 Book2 - Medical Records Administration BranchGeorgesNo ratings yet
- 7es Science Lesson Plan ExampleDocument9 pages7es Science Lesson Plan ExampleKing GarciaNo ratings yet
- SMCH 30Document15 pagesSMCH 30Cita BudiartiNo ratings yet
- Pathology of Skeletal SystemDocument65 pagesPathology of Skeletal SystemFirda S SalsabilaNo ratings yet
- ICD 10 Dalam ExcelDocument103 pagesICD 10 Dalam ExcelJumpa Utama AmrannurNo ratings yet
- AMBOSS 2021 ENAM Study GuideDocument49 pagesAMBOSS 2021 ENAM Study GuideMadeline DelgadoNo ratings yet
- Emergencies in Pediatric SurgeryDocument61 pagesEmergencies in Pediatric Surgeryapi-198361160% (1)
- Hypoxia: and Its Effects On HealthDocument36 pagesHypoxia: and Its Effects On HealthVeres András100% (2)
- Nutrition and Skeletal MuscleFrom EverandNutrition and Skeletal MuscleStéphane WalrandNo ratings yet
- Nursing Management of Patients WithDocument8 pagesNursing Management of Patients Withfunky goodNo ratings yet
- Lectire-Hypoxia 2020Document21 pagesLectire-Hypoxia 2020Bol Dhalbeny Malual100% (1)
- Dame HandbookDocument284 pagesDame Handbooktcalith100% (1)
- Respiratory Muscle Training in Chronic Obstructive Pulmonary Disease Antrenamentul Mușchilor Respiratori În Boala Pulm...Document4 pagesRespiratory Muscle Training in Chronic Obstructive Pulmonary Disease Antrenamentul Mușchilor Respiratori În Boala Pulm...Oana BătrînuNo ratings yet
- 24-Article File-62-1-10-20160916Document9 pages24-Article File-62-1-10-20160916jayasmanNo ratings yet
- FsaasfdDocument10 pagesFsaasfdzuliamNo ratings yet
- Peripheral Muscle Dysfunction in Chronic Obstructive Pulmonary DiseaseDocument14 pagesPeripheral Muscle Dysfunction in Chronic Obstructive Pulmonary DiseaseDaniel Tarride GonzalezNo ratings yet
- Art. Physiology of Respiratory Disturbances in Muscular DystrophiesDocument10 pagesArt. Physiology of Respiratory Disturbances in Muscular DystrophiesCïnthïa L. Natïvïdad PeñaNo ratings yet
- Pulmonary Rehabilitation For Management of Chronic Obstructive Pulmonary DiseaseDocument7 pagesPulmonary Rehabilitation For Management of Chronic Obstructive Pulmonary DiseaseArantxa BenitezNo ratings yet
- Respiratory Diseases and Muscle Dysfunction: ReviewDocument17 pagesRespiratory Diseases and Muscle Dysfunction: ReviewMatias Emilio BirknerNo ratings yet
- Adaptations in Training 1Document22 pagesAdaptations in Training 1raian claudeNo ratings yet
- Scott Warren 2016Document3 pagesScott Warren 2016MichaelJonatanNo ratings yet
- Chapter 5. Respir SysDocument36 pagesChapter 5. Respir SysKIDUS YAREDNo ratings yet
- 08 - Chapter 1Document12 pages08 - Chapter 1Nirmaljeet KaurNo ratings yet
- Impaired Muscle Oxygenation and Elevated Exercise Blood Pressure in Hypertensive PatientsDocument14 pagesImpaired Muscle Oxygenation and Elevated Exercise Blood Pressure in Hypertensive PatientsRachmat Wihandana AgasiNo ratings yet
- Part Vii. Hypoxia: Table 7-1. Classification of The HypoxiaDocument7 pagesPart Vii. Hypoxia: Table 7-1. Classification of The HypoxiaAlex HirschNo ratings yet
- Exercise COPD-342-355 SeparadoDocument14 pagesExercise COPD-342-355 SeparadoKuririn matiasNo ratings yet
- Forum Activity - 2 - Physiology of Performance and FatigueDocument5 pagesForum Activity - 2 - Physiology of Performance and Fatiguearvinp89No ratings yet
- Pan (2021)Document10 pagesPan (2021)Bruno TeixeiraNo ratings yet
- Fatiga Muscular en La LaringeDocument11 pagesFatiga Muscular en La Laringelina.m.castellanos.cNo ratings yet
- Fatigue AssignmentDocument9 pagesFatigue AssignmentRishbha TikuNo ratings yet
- Fast TwitchDocument18 pagesFast TwitchJohn BullNo ratings yet
- Reentrenamiento Muscular en Pacientes de UCIDocument5 pagesReentrenamiento Muscular en Pacientes de UCISandra GarciaNo ratings yet
- Respiratory DR - AntonioDocument3 pagesRespiratory DR - AntonioMonique Angela Turingan GanganNo ratings yet
- NIH Public Access: Author ManuscriptDocument12 pagesNIH Public Access: Author Manuscriptlie antoNo ratings yet
- Dr. Agussalim Bukhari, M.Med, PH.D, SP - GK (K)Document47 pagesDr. Agussalim Bukhari, M.Med, PH.D, SP - GK (K)Vika LeiwaNo ratings yet
- Wang (2021) Effects of Exercise-Induced ROS On The PathophysiologicalDocument5 pagesWang (2021) Effects of Exercise-Induced ROS On The PathophysiologicalBruno TeixeiraNo ratings yet
- 06-Fatigue, DOMS, OvertrainingDocument10 pages06-Fatigue, DOMS, OvertrainingSandiNo ratings yet
- Biomolecules 14 00050Document14 pagesBiomolecules 14 00050kqmeccaNo ratings yet
- Antioxidants 12 01576Document15 pagesAntioxidants 12 01576kiro123.sangminNo ratings yet
- Rhabdomyolysis of The Deltoid Muscle in A BodybuilDocument4 pagesRhabdomyolysis of The Deltoid Muscle in A Bodybuildalyashakir79No ratings yet
- Respiratory Physiology PDFDocument4 pagesRespiratory Physiology PDFDiego AristizabalNo ratings yet
- Metabolic Comunication ExerciseDocument12 pagesMetabolic Comunication ExerciseKevin VillaNo ratings yet
- Disfuncion Cardiada en La Sepsis Clin Chest Med Jun 2016Document10 pagesDisfuncion Cardiada en La Sepsis Clin Chest Med Jun 2016lizzie clavijoNo ratings yet
- Moylan 2007Document19 pagesMoylan 2007JFFNo ratings yet
- Brooks 2023 - Lactate As A Myokine and Exerkine Drivers and Signals of Physiology and MetabolismDocument20 pagesBrooks 2023 - Lactate As A Myokine and Exerkine Drivers and Signals of Physiology and MetabolismEduardo VieyraNo ratings yet
- Remodelacion Mitocondrial Musculoesqueletica en Ejercicio y Enfermedad.2018.Document12 pagesRemodelacion Mitocondrial Musculoesqueletica en Ejercicio y Enfermedad.2018.cristobalarancibia71No ratings yet
- GERIATRICSDocument10 pagesGERIATRICSariel dazaNo ratings yet
- Nrf2 Activation As Target To Implement Therapeutic Treatments 2015Document6 pagesNrf2 Activation As Target To Implement Therapeutic Treatments 2015Fabiana BelchiorNo ratings yet
- Review: Running Head: Nitric Oxide and Energy Balance in HypoxiaDocument70 pagesReview: Running Head: Nitric Oxide and Energy Balance in HypoxiaAprilihardini LaksmiNo ratings yet
- Exercise Physiology - UpToDateDocument29 pagesExercise Physiology - UpToDateVinicius CobelNo ratings yet
- Evaluacion de Los Musculos Respiratorios en La Practica ClinicaDocument9 pagesEvaluacion de Los Musculos Respiratorios en La Practica ClinicaDaniela CalleNo ratings yet
- IUBMB Life - 2008 - Vin A - Free Radicals in Exhaustive Physical Exercise Mechanism of Production and Protection byDocument7 pagesIUBMB Life - 2008 - Vin A - Free Radicals in Exhaustive Physical Exercise Mechanism of Production and Protection by4ymwg78wxcNo ratings yet
- Skeletal Muscle in The Fight Against Chronic Diseases: ExactaDocument4 pagesSkeletal Muscle in The Fight Against Chronic Diseases: ExactaAgustin LopezNo ratings yet
- Adaptations To ExerciseDocument15 pagesAdaptations To ExerciseDiany CéspedesNo ratings yet
- Consequences of Brief Ischemia Stunning, Preconditioning, and Their Clinical Implications PDFDocument10 pagesConsequences of Brief Ischemia Stunning, Preconditioning, and Their Clinical Implications PDFSol SolNo ratings yet
- NIH Public Access: Author ManuscriptDocument19 pagesNIH Public Access: Author ManuscriptdvenumohanNo ratings yet
- Mitochondrial Dysfunction in Intensive Care UnitAcquired Weakness and Critical Illness Myopathy A Narrative ReviewDocument27 pagesMitochondrial Dysfunction in Intensive Care UnitAcquired Weakness and Critical Illness Myopathy A Narrative ReviewJose EdgarNo ratings yet
- HHS Public Access: Myobolites: Muscle-Derived Metabolites With Paracrine and Systemic EffectsDocument12 pagesHHS Public Access: Myobolites: Muscle-Derived Metabolites With Paracrine and Systemic EffectsGabriela SolanoNo ratings yet
- Oxidative Stress and Antioxidants in Exercise: C. Leeuwenburgh and J. W. HeineckeDocument10 pagesOxidative Stress and Antioxidants in Exercise: C. Leeuwenburgh and J. W. HeineckeClara JensNo ratings yet
- HIF Hipoxia y Envejecimiento EuiJuYeo ExpMolMed2019Document15 pagesHIF Hipoxia y Envejecimiento EuiJuYeo ExpMolMed2019Luis CruzNo ratings yet
- Powers (2008) Exercise-Induced Oxidative Stress Cellular Mechanisms andDocument59 pagesPowers (2008) Exercise-Induced Oxidative Stress Cellular Mechanisms andBruno TeixeiraNo ratings yet
- Skeletal Muscle Fiber Type - Influence On Contractile and Metabolic PropertiesDocument5 pagesSkeletal Muscle Fiber Type - Influence On Contractile and Metabolic PropertiesQuintanaNo ratings yet
- Fisiologia FibramuscularDocument5 pagesFisiologia FibramuscularSilvanaGomesNo ratings yet
- Vascular Ischaemia and Reperfusion Injury: Holger K. Eltzschig and Charles D. CollardDocument16 pagesVascular Ischaemia and Reperfusion Injury: Holger K. Eltzschig and Charles D. CollardDuratul FahliaNo ratings yet
- Glycogen Storage Diseases of Muscle Chapter 39 PDFDocument26 pagesGlycogen Storage Diseases of Muscle Chapter 39 PDFIsaac Mackliz VillegasNo ratings yet
- Impact of Pneumococcal Conjugate Vaccine in At-Risk Adults 2022Document48 pagesImpact of Pneumococcal Conjugate Vaccine in At-Risk Adults 2022Rosi AmaliaNo ratings yet
- General Medicine PresentationDocument32 pagesGeneral Medicine PresentationKASATSANo ratings yet
- Dyspneabyahammednaseem 210628024048Document19 pagesDyspneabyahammednaseem 210628024048Naseem Bin YoosafNo ratings yet
- UntitledDocument1 pageUntitledShally ShalawatiNo ratings yet
- St. Paul University PhilippinesDocument6 pagesSt. Paul University PhilippinesAshley Dayag0% (1)
- NCM 112 Lecture Notes (Respiratory System and Its Diseases)Document9 pagesNCM 112 Lecture Notes (Respiratory System and Its Diseases)Kyle FernandezNo ratings yet
- Approach To Common Respiratory DiseaseDocument57 pagesApproach To Common Respiratory DiseaseRajhmuniran KandasamyNo ratings yet
- Chronic Obstructive Pulmonary DisorderDocument15 pagesChronic Obstructive Pulmonary Disordercrabby_chicNo ratings yet
- Chronic Obstructive Pulmonary Disease (Lancet)Document16 pagesChronic Obstructive Pulmonary Disease (Lancet)marcos gamboaNo ratings yet
- Soap Note CoughDocument19 pagesSoap Note CoughlameckwesiNo ratings yet
- Emphysema Research ReportDocument19 pagesEmphysema Research Reportحرا مغلNo ratings yet
- UCG 2023 Publication (Final PDF Version)Document1,158 pagesUCG 2023 Publication (Final PDF Version)paul okelloNo ratings yet
- Analysis in Nutrition Research Principles of Statistical Methodology and Interpretation of The Results 1St Edition George Pounis Full ChapterDocument52 pagesAnalysis in Nutrition Research Principles of Statistical Methodology and Interpretation of The Results 1St Edition George Pounis Full Chaptergloria.morales231100% (5)
- End Blok Respi SoalDocument6 pagesEnd Blok Respi Soalanz_4191No ratings yet
- Internet-Of-Things-Based Sensor Module For Respiratory Tracking SystemDocument11 pagesInternet-Of-Things-Based Sensor Module For Respiratory Tracking SystemAulia AgistaNo ratings yet
- Clinical Asthma Pathway: ED Phase 1a: Initial Assessment - 1st HourDocument2 pagesClinical Asthma Pathway: ED Phase 1a: Initial Assessment - 1st Hourd'Agung NugrohoNo ratings yet
- Pathology For The Health Professions 5Th Edition Damjanov Solutions Manual Full Chapter PDFDocument36 pagesPathology For The Health Professions 5Th Edition Damjanov Solutions Manual Full Chapter PDFcrastzfeiej100% (9)
- Jurnal RespirasiDocument5 pagesJurnal RespirasiRisyda Ma'rifatul Khoirot100% (1)
- Jurnal SOPT 4Document6 pagesJurnal SOPT 4Anonymous Skzf3D2HNo ratings yet
- ACSM S Exercise Management For Persons With Chronic Diseases and Disabilities 4th Edition American College of Sports MedicineDocument43 pagesACSM S Exercise Management For Persons With Chronic Diseases and Disabilities 4th Edition American College of Sports Medicineanthony.magera384100% (10)
- Nutrition and Respiratory Diseases PDFDocument53 pagesNutrition and Respiratory Diseases PDFliggiedy100% (1)
- Industry Profile Portea MedicalDocument48 pagesIndustry Profile Portea Medicalvanshika sharmaNo ratings yet
- Essentials of Medical Language 3rd Edition Allan Test Bank Full Chapter PDFDocument67 pagesEssentials of Medical Language 3rd Edition Allan Test Bank Full Chapter PDFMollyMoralescowyxefb100% (12)