You might also like
- The Biology of HomosexualityDocument201 pagesThe Biology of HomosexualityIsis Bugia100% (1)
- 974-0753 Onan RDJC RDJF Diesel Engine Service Manual (09-1984)Document64 pages974-0753 Onan RDJC RDJF Diesel Engine Service Manual (09-1984)Leo BurnsNo ratings yet
- Georgia Habitats Lesson PlansDocument5 pagesGeorgia Habitats Lesson PlansBecky BrownNo ratings yet
- The Moral Imperative of Reproductive Rights, Health, and JusticeDocument8 pagesThe Moral Imperative of Reproductive Rights, Health, and JusticeKepa NeritaNo ratings yet
- Sexual and Gender IdentityDocument28 pagesSexual and Gender IdentityCaroline AlagadmoNo ratings yet
- Practice Writing Effective SentencesDocument5 pagesPractice Writing Effective SentencesHaekal FarabyNo ratings yet
- Heat Sink Capacity Mesurment in Inservice PipelineDocument13 pagesHeat Sink Capacity Mesurment in Inservice PipelineSomeshNo ratings yet
- Enough Is Enough - Tackling Sexism Sexual Harassment - 2023 - The Lancet RegioDocument3 pagesEnough Is Enough - Tackling Sexism Sexual Harassment - 2023 - The Lancet RegioGraziellia Bianca Huamani MartinezNo ratings yet
- Perceptions of Anal Intercourse Among Heterosexual Women: A Pilot Qualitative StudyDocument9 pagesPerceptions of Anal Intercourse Among Heterosexual Women: A Pilot Qualitative Studyyohelio sibuNo ratings yet
- J Terry Lesbians Under The Medical GazeDocument24 pagesJ Terry Lesbians Under The Medical GazeJillian Grace HurtNo ratings yet
- Female Genital Mutilation - Health Consequences and Complications-A Short Literature Review PDFDocument7 pagesFemale Genital Mutilation - Health Consequences and Complications-A Short Literature Review PDFYushlihah RofiatiNo ratings yet
- Maternal Nursing Care - CHPT 6 Human Sexuality and FertilityDocument28 pagesMaternal Nursing Care - CHPT 6 Human Sexuality and Fertilitythubtendrolma100% (1)
- Genital Injuries: Are They Telling Us Something About Sexual Violence?Document8 pagesGenital Injuries: Are They Telling Us Something About Sexual Violence?Scott PymNo ratings yet
- Mary Sexual BehaviourDocument11 pagesMary Sexual BehaviourAlade Temitayo100% (1)
- 1 s2.0 S1752928X15000335 PDFDocument4 pages1 s2.0 S1752928X15000335 PDFDhyo Asy-shidiq HasNo ratings yet
- Research Paper On FGMDocument7 pagesResearch Paper On FGMtgyuhdvkg100% (2)
- Medical Advances in Transsexualism and The Legal ImplicationsDocument6 pagesMedical Advances in Transsexualism and The Legal ImplicationsAle Mujica RodríguezNo ratings yet
- Gender Identity Disorder - General Overview and Surgical Treatment For Vaginoplasty in Male To Female TranssexualsDocument11 pagesGender Identity Disorder - General Overview and Surgical Treatment For Vaginoplasty in Male To Female TranssexualsJulián David Ríos ZuluagaNo ratings yet
- Abortion Literature ReviewDocument7 pagesAbortion Literature Reviewea8m12sm100% (1)
- Vulnerable Population ProjectDocument6 pagesVulnerable Population Projectapi-739007989No ratings yet
- Conceptulising StigmaDocument16 pagesConceptulising StigmaRitesh kumarNo ratings yet
- Ebook PDF Childbirth Vulnerability and Law Exploring Issues of Violence and Control PDFDocument41 pagesEbook PDF Childbirth Vulnerability and Law Exploring Issues of Violence and Control PDFmike.casteel807100% (35)
- Physicians Use of Inclusive Sexual Orientation Language During Teenage Annual VisitsDocument9 pagesPhysicians Use of Inclusive Sexual Orientation Language During Teenage Annual VisitsTherese Berina-MallenNo ratings yet
- Ambiguous Genitalia in ChildrenDocument8 pagesAmbiguous Genitalia in ChildrenEmmanuel NwosuNo ratings yet
- ForensikDocument34 pagesForensikPutri Juwita DharmaliaNo ratings yet
- Female Circumcision Literature ReviewDocument8 pagesFemale Circumcision Literature Reviewaflspwxdf100% (1)
- Statement of The ProblemDocument9 pagesStatement of The ProblemTrisha MilesNo ratings yet
- SOSC 3169 EXAM PREP BY Muhammed SyedDocument8 pagesSOSC 3169 EXAM PREP BY Muhammed SyedmuhammedNo ratings yet
- Dutton, Koenig, & Fennie, 2008Document7 pagesDutton, Koenig, & Fennie, 2008Anonymous 75M6uB3OwNo ratings yet
- Looking Out Project Is Gender/Sexuality Something You're Born With or Taught ?Document16 pagesLooking Out Project Is Gender/Sexuality Something You're Born With or Taught ?api-300936219No ratings yet
- Bodkin Et Al, 2019Document11 pagesBodkin Et Al, 2019calebdcarr628No ratings yet
- SOCIOLOGY ASSIGNMENT MainDocument8 pagesSOCIOLOGY ASSIGNMENT MainParth GuptaNo ratings yet
- Sex LectureDocument10 pagesSex LectureJpt YapNo ratings yet
- Trastorno SexualDocument7 pagesTrastorno SexualDylan Steven Correa FernándezNo ratings yet
- Module 4: How Should Life and Its Extension Be Ethically Viewed?Document4 pagesModule 4: How Should Life and Its Extension Be Ethically Viewed?livNo ratings yet
- HannahDocument47 pagesHannahapi-460767991No ratings yet
- SexualfunctionDocument9 pagesSexualfunctionGiray TaraktaşNo ratings yet
- The Revised Report From The National Task Force On Juvenile Sexu 1993Document116 pagesThe Revised Report From The National Task Force On Juvenile Sexu 1993AltaicaNo ratings yet
- The Effect of Religious Background On The Attitude Towards Sex SelectionDocument5 pagesThe Effect of Religious Background On The Attitude Towards Sex SelectionLorena RodríguezNo ratings yet
- LIv 082Document6 pagesLIv 082Ujjwal MaharjanNo ratings yet
- Do Women Pretend Orgasm To Retain A Mate?Document5 pagesDo Women Pretend Orgasm To Retain A Mate?Csanyi EditNo ratings yet
- WHO RHR 18.15 EngDocument24 pagesWHO RHR 18.15 EngsofiabloemNo ratings yet
- Trends Urol Men S Health - 2016 - Winder - The Management of Hypersexuality in MenDocument4 pagesTrends Urol Men S Health - 2016 - Winder - The Management of Hypersexuality in MenCAS EnglishNo ratings yet
- Quantitative Research On Sexual Abuse PDFDocument22 pagesQuantitative Research On Sexual Abuse PDFDivine GraceNo ratings yet
- Female Homosexual DevelopmentDocument4 pagesFemale Homosexual Developmentpleasure masangoNo ratings yet
- Primeras Experiencias Sexuales en Adolescentes Inhaladores de Solventes, de La Genitalidad Al ErotismoDocument14 pagesPrimeras Experiencias Sexuales en Adolescentes Inhaladores de Solventes, de La Genitalidad Al ErotismoIván SaucedoNo ratings yet
- CIA Trans SecurityDocument7 pagesCIA Trans SecuritySydney BloomNo ratings yet
- Female Orgasm and Overall Sexual Function and Habits: A Descriptive Study of A Cohort of U.S. WomenDocument12 pagesFemale Orgasm and Overall Sexual Function and Habits: A Descriptive Study of A Cohort of U.S. Womenkerebo NgwenyaNo ratings yet
- Sexual Behavior of LesbiansDocument5 pagesSexual Behavior of LesbiansHervis FantiniNo ratings yet
- Literature Review AbortionDocument8 pagesLiterature Review Abortionafmacaewfefwug100% (1)
- Exploring The Sexual and Reproductive Health Issues of Visually Impaired Women in Ghana (2017)Document7 pagesExploring The Sexual and Reproductive Health Issues of Visually Impaired Women in Ghana (2017)Helena CarimánNo ratings yet
- Cutting Off The Defective Germ-Plasm in The American PopulationDocument6 pagesCutting Off The Defective Germ-Plasm in The American PopulationAli LaldinNo ratings yet
- Experiences and Impact of Mistreatment and Obstetric Violence On Women During Childbearing: A Systematic Review ProtocolDocument8 pagesExperiences and Impact of Mistreatment and Obstetric Violence On Women During Childbearing: A Systematic Review ProtocolNathaly MorenoNo ratings yet
- Transsexual Attractions and Sexual Reassignment SuDocument14 pagesTranssexual Attractions and Sexual Reassignment SuFavour EbubechiNo ratings yet
- PsychologyDocument14 pagesPsychologyJyoti ChaudharyNo ratings yet
- Genetic Research Among The Havasupai: A Cautionary Tale: Robyn L. Sterling, JD, MPHDocument10 pagesGenetic Research Among The Havasupai: A Cautionary Tale: Robyn L. Sterling, JD, MPHMin KyuNo ratings yet
- Fredrickson1997 PDFDocument34 pagesFredrickson1997 PDFFlorencia RiveroNo ratings yet
- Gender Vs FavorabiltyDocument3 pagesGender Vs FavorabiltyMia SantiagoNo ratings yet
- Offenders: Characteristics and TreatmentDocument22 pagesOffenders: Characteristics and TreatmentKiana TehraniNo ratings yet
- 1970 - Zuger Vs Money-A Critical Review of The Evidence From HermaphroditismDocument20 pages1970 - Zuger Vs Money-A Critical Review of The Evidence From HermaphroditismRafael FredaNo ratings yet
- "Hermaphrodites"?: So You Wanna Know AboutDocument1 page"Hermaphrodites"?: So You Wanna Know AboutMariana GentiliNo ratings yet
- 12.4.18 Final Revised 12.4.18 Joint Letter To HHS DOJ DOE Uphold Definition of SexDocument8 pages12.4.18 Final Revised 12.4.18 Joint Letter To HHS DOJ DOE Uphold Definition of SexShane Vander HartNo ratings yet
- Female Genital Mutilation Research Paper OutlineDocument8 pagesFemale Genital Mutilation Research Paper Outlinegz9p83dd100% (1)
- Unveiling the Hidden Risks: Exploring the Dangers of Anal Sex to WomenFrom EverandUnveiling the Hidden Risks: Exploring the Dangers of Anal Sex to WomenNo ratings yet
- QuizBowl QuestionsDocument84 pagesQuizBowl QuestionsJowel MercadoNo ratings yet
- CW9 Identifying Functions 5Document2 pagesCW9 Identifying Functions 5Xavier BurrusNo ratings yet
- Numerical WindingDocument12 pagesNumerical Windingsujal jhaNo ratings yet
- Smart Energy Meter and Monitoring System Using Iot IJERTCONV8IS14011Document4 pagesSmart Energy Meter and Monitoring System Using Iot IJERTCONV8IS14011Gurpreet SinghNo ratings yet
- Apple Computer Inc. v. Burst - Com, Inc. - Document No. 146Document39 pagesApple Computer Inc. v. Burst - Com, Inc. - Document No. 146Justia.comNo ratings yet
- Ecs C42iix Rev C Vit m2400 1Document36 pagesEcs C42iix Rev C Vit m2400 1Victor Pic100% (1)
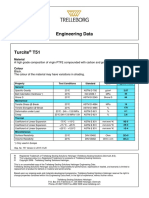
- Turcite T51 Engineering DataDocument1 pageTurcite T51 Engineering DataAntonio Rivera VillavicencioNo ratings yet
- Un EinsteinDocument22 pagesUn Einsteinapi-26005027No ratings yet
- Industrial Training Sample Report of Last YearDocument42 pagesIndustrial Training Sample Report of Last YearKetan NikamNo ratings yet
- The Mole ConceptDocument12 pagesThe Mole ConceptVictor OkosunNo ratings yet
- Outline On Dengue Fever - EDITEDDocument2 pagesOutline On Dengue Fever - EDITEDDavid Skeat0% (1)
- Numerology 666 Meaning: What Angel Number 666 REALLY Means!Document2 pagesNumerology 666 Meaning: What Angel Number 666 REALLY Means!LlNo ratings yet
- View Result - CUMS Comprehensive University Management System - M.K.Bhavnagar University Powered by AuroMeera A College Management System ProviderDocument1 pageView Result - CUMS Comprehensive University Management System - M.K.Bhavnagar University Powered by AuroMeera A College Management System ProviderKiaanNo ratings yet
- Compteur 7757 - A PDFDocument16 pagesCompteur 7757 - A PDFbromartNo ratings yet
- Business, Government & Society: Pawan Kumar N K 12301005Document8 pagesBusiness, Government & Society: Pawan Kumar N K 12301005Pawan NkNo ratings yet
- Lighting Movements-The Fox On The FairwayDocument1 pageLighting Movements-The Fox On The FairwayabneypaigeNo ratings yet
- Hasnain A KhanDocument2 pagesHasnain A KhanFatima ButtNo ratings yet
- ISO 8861 Blower Engine RoomDocument28 pagesISO 8861 Blower Engine Roommohammad choirul huda100% (1)
- Metal Roof Roll Forming MachineDocument6 pagesMetal Roof Roll Forming MachineDarío Fernando LemaNo ratings yet
- NUTRACEUTICALDocument8 pagesNUTRACEUTICALShubham GuptaNo ratings yet
- Grade 7-Advanced Science Environmental ScienceDocument8 pagesGrade 7-Advanced Science Environmental ScienceChrisel Luat LopezNo ratings yet
- Stresses in Large Horizontal Cylindrical Pressure Vessels On Two Saddle Supports - Zick (1951) OriginalDocument11 pagesStresses in Large Horizontal Cylindrical Pressure Vessels On Two Saddle Supports - Zick (1951) OriginalBryan Pérez PérezNo ratings yet
- How To Write A Research Paper With Parenthetical DocumentationDocument5 pagesHow To Write A Research Paper With Parenthetical Documentationc9spy2qzNo ratings yet
- Country Item Name Litre Quart Pint Nip 700 ML IndiaDocument17 pagesCountry Item Name Litre Quart Pint Nip 700 ML Indiajhol421No ratings yet
- BHHHJDocument10 pagesBHHHJAnonymous vLerKYANo ratings yet
- Installiation of Automatic Fire Sprinkler System and Design CalculationDocument8 pagesInstalliation of Automatic Fire Sprinkler System and Design CalculationSat AungNo ratings yet