Professional Documents
Culture Documents
AI Interpretation of Medical Images - NEJM
Uploaded by
Adrian H. AguileraOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
AI Interpretation of Medical Images - NEJM
Uploaded by
Adrian H. AguileraCopyright:
Available Formats
The n e w e ng l a n d j o u r na l of m e dic i n e
Review Article
AI in Medicine
Jeffrey M. Drazen, M.D., Editor, Isaac S. Kohane, M.D., Ph.D., Guest Editor,
and Tze‑Yun Leong, Ph.D., Guest Editor
The Current and Future State of AI
Interpretation of Medical Images
Pranav Rajpurkar, Ph.D., and Matthew P. Lungren, M.D., M.P.H.
T
he interpretation of medical images — a task that lies at the From the Department of Biomedical In‑
heart of the radiologist’s work — has involved the growing adoption of formatics, Harvard Medical School, Bos‑
ton (P.R.); the Center for Artificial Intelli‑
artificial intelligence (AI) applications in recent years. This article reviews gence in Medicine and Imaging, Stanford
progress, challenges, and opportunities in the development of radiologic AI models University, Stanford, and the Department
and their adoption in clinical practice. We discuss the functions that AI-based of Radiology and Biomedical Imaging, Uni‑
versity of California, San Francisco, San
algorithms serve in assisting radiologists, including detection, workflow triage, Francisco — both in California (M.P.L.);
and quantification, as well as the emerging trend of the use of medical-imaging and Microsoft, Redmond, Washington
AI by clinicians who are not radiologists. We identify the central challenge of (M.P.L.). Dr. Rajpurkar can be contacted
at pranav_rajpurkar@hms.harvard.edu.
generalization in the use of AI algorithms in radiology and the need for validation
safeguards that encompass clinician–AI collaboration, transparency, and post Drs. Rajpurkar and Lungren contributed
equally to this article.
deployment monitoring. Finally, we discuss the rapid progress in developing multi-
modal large language models in AI; this progress represents a major opportunity N Engl J Med 2023;388:1981-90.
DOI: 10.1056/NEJMra2301725
for the development of generalist medical AI models that can tackle the full spec- Copyright © 2023 Massachusetts Medical Society.
trum of image-interpretation tasks and more. To aid readers who are unfamiliar
with terms or ideas used for AI in general or AI in image interpretation, a Glos-
sary is included with this article.
In recent years, AI models have been shown to be remarkably successful in
interpretation of medical images.1 Their use has been extended to various medical-
imaging applications, including, but not limited to, the diagnosis of dermatologic
conditions2 and the interpretation of electrocardiograms,3 pathological slides,4 and
ophthalmic images.5 Among these applications, the use of AI in radiology has
shown great promise in detecting and classifying abnormalities on plain radio-
graphs,6 computed tomographic (CT) scans,7 and magnetic resonance imaging
(MRI) scans,8 leading to more accurate diagnoses and improved treatment decisions.
Even though the Food and Drug Administration (FDA) has approved more than
200 commercial radiology AI products, substantial obstacles must be overcome
before we are likely to see widespread successful clinical use of these products.
The incorporation of AI in radiology poses both potential benefits and challenges
for the medical and AI communities. We expect that the eventual resolution of
these issues and more comprehensive solutions, including the development of new
foundation models, will lead to broader adoption of AI within this health care
sector.
A I Use in R a diol o gy
Radiology as a specialty is well positioned for the application and adoption of AI
because of several key factors. First, AI excels in analyzing images,9 and unlike
other specialties that use imaging, radiology has an established digital workflow
and universal standards for image storage, so that it is easier to integrate AI.10
n engl j med 388;21 nejm.org May 25, 2023 1981
The New England Journal of Medicine
Downloaded from nejm.org by Adrian H. Aguilera on August 24, 2023. For personal use only. No other uses without permission.
Copyright © 2023 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
Glossary
Continual learning: A process in which an AI model learns from new data over time while retaining previously acquired
knowledge.
Data set shift: The shift from data used to train a machine-learning model to data encountered in the real world. This
shift can cause the model to perform poorly when used in the real world, even if it performed well during training.
Federated learning: A distributed machine-learning approach that enables multiple devices or nodes to collaboratively
train a shared model while keeping their individual data local, thereby preserving privacy and reducing data commu‑
nication overhead.
Foundation models: AI models that serve as a starting point for developing more specific AI models. Foundation mod‑
els are trained on large amounts of data and can be fine-tuned for specific applications, such as detecting lesions or
segmenting anatomical structures.
Generalist medical AI models: A class of advanced medical foundation models that can be used across various medical
applications, replacing task-specific models. Generalist medical AI models have three key capabilities that distinguish
them from conventional medical AI models. They can adapt to new tasks described in plain language, without re‑
quiring retraining; they can accept inputs and produce outputs using various combinations of data types; and they
are capable of logically analyzing unfamiliar medical content.
Large language models: AI models consisting of a neural network with billions of weights or more, trained on large amounts
of unlabeled data. These models have the ability to understand and produce human language and may also apply to
images and audio.
Multimodal models: AI models that can understand and combine different types of medical data, such as medical im‑
ages and electronic health records. Multimodal models are particularly useful in medicine for tasks that require a
comprehensive understanding of the patient, such as diagnosis and individualized treatment planning.
Self-supervised models: AI models that can learn from medical data without the need for explicit annotations. These
models can be used to learn representations of medical data that are useful for a wide range of tasks, such as di‑
agnosis and patient monitoring. Self-supervised models are particularly useful in medicine when labeled data are
scarce or expensive to obtain.
Zero-shot learning: The capability of an AI model to perform a task or solve a problem for which it has not been explicitly
trained, without the need for any additional training data. In medicine, this can be particularly useful when there is a
shortage of labeled data available for a specific medical task.
Furthermore, AI fits naturally in the workflow pulmonary nodules and breast abnormalities. In
of image interpretation and can replicate well- addition, AI algorithms enhance preinterpretive
defined interpretive tasks effectively.11 processes, including image reconstruction, image
acquisition, and mitigation of image noise.17
AI Use for Radiologists There is promise in exploring radiologic AI
AI can be used in the field of radiology to ana- models that can expand interpretive capabilities
lyze images from a wide range of techniques, beyond those of human experts. For instance, AI
including radiography, CT, ultrasonography, and algorithms can accurately predict clinical out-
MRI. Radiologic AI algorithms serve a number comes on the basis of CT data in cases of trau-
of narrow image-analysis functions to assist radi- matic brain injury21 and cancer.22 In addition, AI-
ologists, such as quantification, workflow triage, derived imaging biomarkers can help to quickly
and image enhancement (Fig. 1).1,12-17 Quantifica- and objectively assess structures and pathologi-
tion algorithms perform segmentation and mea- cal processes related to body composition, such
surements of anatomical structures or abnor- as bone mineral density, visceral fat, and liver fat,
malities. Common examples include measuring which can be used to screen for various health
breast density, identifying anatomical structures conditions.23 When applied to routine CT imag-
in the brain, quantitating cardiac flow,18 and as- ing, these AI-derived biomarkers are proving
sessing local lung-tissue density. Workflow triage useful in predicting future adverse events.24
involves flagging and communicating suspected Moreover, recent research has shown that coro-
positive findings, including, but not limited to, nary-artery calcium scores, which are typically
intracranial hemorrhage, intracranial large-vessel obtained on the basis of CT scanning, can be de-
occlusion,19 pneumothorax,20 and pulmonary em- termined by means of cardiac ultrasonography.25
bolism. AI is also used for the detection, local- These findings point to the value of radiologic
ization, and classification of conditions such as AI models for patients (e.g., no radiation exposure).
1982 n engl j med 388;21 nejm.org May 25, 2023
The New England Journal of Medicine
Downloaded from nejm.org by Adrian H. Aguilera on August 24, 2023. For personal use only. No other uses without permission.
Copyright © 2023 Massachusetts Medical Society. All rights reserved.
000000100011100001110011010110110000110101111010111011111001110101110001
111001001000000000010000100111000000110111001001001111110111010000000001
Using AI to Interpret Medical Images
100000011001000101101111101110010111111011110011000100111101100000100010
101100111111101110110011111100010100010111001111111101111100001101010000
101101010100100011011100111000101010110110000101101001011000111010110000
001101110000111001110111001000001011010110011111111010110111100001101011
111100111011000000110001111001000001001001101100000111000000000111110010
001101100000001101100110111010110100010011110001100111111101001100101100
110100101011110111100101001000100101001010001000101010111101111100110001
111011101110101001110100001011001111100100110011100010011110101101010000
001011010000110000110000111100101000100100111100111001001000001011001101
110110110101101010100101001010011011100011111100100111101000011100110100
000000100000000100100000101010010101111000111011011000100010101001110001
101011111011100111000110111101111000101111000100011001110010111111000010
Detection and Diagnosis
Type of Imaging Output Results
011100100001000011000100111010011000111101111111101001001111100010000111
100101011000100101100100111111110110011011010010010000110011001001001101
101100000000000000111111011110100101100101010101111000000110011111001001
101000110100011000110101101111110001010100001110101010111011101000010111
by AI Algorithms
000011010110010101010110100011000111001101111001110101011001110111100110
001101000110010010111110110101001010100001111010010101011101101100000111
111001101111101001110100100011010011010100110101011101100010100011001110
110100110110111000001010011011101111101100000011001000101101100100110110
101011011000111010010101100001001010010010110010100110101011110101110010
100000101010000110110110010010000011101000010110110001011101011100000000
000001110110110001011111000011100000000000000101100000100100110111001000
011010110100101001000100110100101100100010001100001011011111111110101001
111111100101100011001000010110110000101000111101110110010000110101110101
010101001110001000111101110011011001000001010000010010010100010100100110 Triage of positive
!
101100010101101000100101100010001000111111111100101101000000010011001010
001000010100011110000100011111000110110011000100101011101010000000011000
010100100011100010100010001011011010000111010010010000010001011111000011 films to top of
111111000010111110001010000100000001011110110010101100001111000101110000
Right-side
01 0 01 01 0 0 1 01 01 0 1 10 1 0 01 0 01 1 10 10 01 01 10 1 01 10 01 1 10 0 10 1 01 0 01 01 10 1 01 1 0 1 1 1 1 01 10 0 1 10 1 0 1 1 10 1 1 01 0 1 10 1 01 1 01 10 10 1 01 0 01 1 radiology worklist
1 1 10 0 0 10 0 0 10 01 0 01 0 01 0 0 01 0 0 1 0 01 01 0 1 0 0 10 1 10 0 0 0 0 0 01 10 1 0 10 10 1 01 0 10 01 0 1 0 01 1 10 1 1 1 1 01 1 10 10 01 1 0 01 0 01 0 0 01 0 0 10
pneumothorax
11 00 00 00 00 01 01 10 10 00 00 11 01 01 00 11 00 10 10 00 10 11 10 11 11 01 10 10 10 00 01 11 01 11 11 11 10 11 11 01 11 11 10 11 01 01 10 11 01 00 01 1000 00 01 01 01 01 10 01 01 00 10 10 10 00 01 00 00 10 11 10
10 0 1 1 0 01 10 1 1 10 1 1 10 0 10 10 1 01 10 1 0 01 1 1 1 10 1 10 01 01 01 10 01 1 01 01 01 10 0 1 1 1 0 01 10 1 1 1 10 10 10 1 01 1 1 10 10 1 0 0 01 0 10 10 0 10 0 10 0 0 0 01
10 0 10 10 01 10 0 1 01 1 0 0 10 0 0 0 1 1 0 1 1 1 0 0 1 10 10 01 0 0 1 01 1 01 1 01 10 1 01 1 10 01 0 0 0 10 0 10 10 0 10 01 01 10 0 10 10 0 0 01 1 10 10 01 10 0 10 1 0 01 01 0 !
01 01 1 1 01 10 1 1 01 0 0 01 10 1 1 01 01 1 1 10 01 1 1 1 0 0 1 01 0 0 0 01 10 0 1 1 01 1 0 1 1 0 0 10 10 10 1 10 10 10 1 0 1 0 1 1 0 10 1 1 1 01 01 01 01 10 1 01 1 0 1 1
10 10 1 1 01 01 1 1 10 0 10 1 0 01 0 0 0 01 10 1 01 01 0 10 1 1 1 01 01 1 01 01 0 01 01 1 01 01 10 0 0 10 1 01 10 1 0 01 0 0 0 10 1 10 01 01 0 01 0 01 0 01 0 10 1 10 10 10 01 01 10 01 !
01 01 10 10 01 1 1 0 0 0 01 0 01 0 1 10 01 1 10 01 01 10 10 0 10 1 10 01 1 0 1 10 0 1 0 01 01 10 0 0 1 1 1 10 01 0 01 1 10 0 0 10 10 10 1 1 10 1 01 1 0 0 10 10 01 01 1 0 10 1 01 01
10 1 01 1 0 0 1 0 10 0 10 10 1 10 01 1 10 1 10 01 01 10 0 1 01 01 1 01 01 01 1 0 01 10 01 1 0 01 1 01 1 0 0 0 10 01 01 0 1 0 1 01 1 01 1 1 10 10 01 1 1 10 1 1 0 0 10 10 0 0 01 1
10 10 10 01 1 1 1 0 10 1 10 0 10 0 10 01 0 10 1 10 0 1 01 0 01 01 10 0 10 10 0 01 1 1 10 10 10 0 0 10 0 0 10 1 01 01 1 1 10 0 01 0 10 0 01 1 10 1 1 0 10 0 10 10 0 10 01 1 0 01 01 0
0 01 1 0 1 1 01 10 01 0 01 01 10 1 0 0 0 01 10 10 01 01 01 01 10 10 10 1 01 0 10 01 1 01 01 01 1 01 0 1 0 0 1 1 10 10 01 0 1 1 10 0 01 1 0 01 10 0 01 0 01 0 1 01 1 1 0 01 1 1 01 10
10 1 0 1 10 0 1 10 0 10 01 10 10 01 10 01 10 0 1 0 01 10 0 10 01 0 10 0 1 0 01 10 1 0 1 1 1 01 0 01 1 1 1 1 10 10 01 01 10 0 0 1 1 1 1 0 1 01 01 0 01 1 1 10 01 0 1 10 0 1 01 01
0 01 0 0 0 0 1 0 01 01 0 0 01 01 01 1 01 0 10 01 0 0 01 01 10 0 1 01 1 0 0 10 01 10 0 1 1 1 1 0 01 0 1 1 10 01 10 1 0 10 10 0 0 0 1 0 01 01 10 01 10 0 10 0 01 1 10 10 0 0 01 1
10 0 10 0 1 1 1 1 10 0 1 10 1 0 0 10 1 10 0 01 0 10 1 01 1 1 10 10 01 1 1 10 10 01 0 0 1 0 10 10 10 10 01 0 01 1 0 0 01 1 10 01 01 1 10 1 01 0 1 01 10 1 10 1 1 10 01 0 01 0 1 0
0 1 10 1 0 0 1 0 01 0 0 1 01 0 01 01 1 10 0 0 01 1 01 01 1 1 10 0 1 0 0 1 1 01 01 0 1 10 10 10 0 1 1 1 10 10 1 1 10 01 10 0 0 10 0 0 10 10 1 10 10 0 0 0 10 0 0 01 0 10 1 10
10 0 0 10 01 10 01 10 1 0 0 01 10 01 0 1 01 1 1 0 0 10 01 01 1 10 1 1 10 1 1 10 0 10 1 0 0 10 1 0 1 10 01 10 0 01 1 01 0 10 0 01 01 0 1 10 01 01 1 1 01 0 1 01 01 10 0 01 1 1 0 10
101100000000000000111111011110100101100101010101111000000110011111001001
Chest Radiograph 101000110100011000110101101111110001010100001110101010111011101000010111
000011010110010101010110100011000111001101111001110101011001110111100110
001101000110010010111110110101001010100001111010010101011101101100000111
111001101111101001110100100011010011010100110101011101100010100011001110
110100110110111000001010011011101111101100000011001000101101100100110110
101011011000111010010101100001001010010010110010100110101011110101110010
100000101010000110110110010010000011101000010110110001011101011100000000
000001110110110001011111000011100000000000000101100000100100110111001000
011010110100101001000100110100101100100010001100001011011111111110101001
111111100101100011001000010110110000101000111101110110010000110101110101
010101001110001000111101110011011001000001010000010010010100010100100110
Detection and
!
101100010101101000100101100010001000111111111100101101000000010011001010
001000010100011110000100011111000110110011000100101011101010000000011000
010100100011100010100010001011011010000111010010010000010001011111000011 localization
111111000010111110001010000100000001011110110010101100001111000101110000
101100111010101011001101101100011011011101111100101011011101011110011011 Left upper-lobe
01 01 00 00 00 00 10 00 00 01 10 11 10 01 00 00 01 10 10 11 00 01 11 10 01 10 00 10 11 00 10 10 00 00 00 01 10 11 00 10 00 11 11 10 10 01 10 01 10 11 11 00 11 11 11 11 11 01 00 10 11 11 00 11 00 11 10 10 01 00 00 10
of abnormalities
solid nodule
11 10 10 00 00 11 01 00 10 00 00 01 01 01 00 01 00 00 00 10 00 01 00 01 11 01 00 10 10 10 01 01 01 01 01 01 10 11 01 11 11 11 00 01 11 01 00 11 01 00 11 1001 01 01 01 00 01 11 01 00 01 10 10 10 00 00 00 00 10 10 11
01 00 10 10 00 10 00 11 11 00 10 11 00 00 00 01 10 11 01 10 01 11 11 11 11 00 11 01 11 10 10 01 10 11 11 11 11 01 01 10 11 11 01 11 00 10 11 11 00 00 00 11 10 10 11 01 01 11 00 01 11 00 00 00 00 00 01 00 00 00 01 10
01 00 01 01 10 00 01 11 11 11 01 01 01 00 01 01 11 10 01 11 10 10 01 01 11 01 01 11 00 00 10 11 10 11 10 10 00 11 10 11 01 11 00 00 01 01 01 01 01 01 01 11 10 01 01 01 01 01 00 10 10 00 01 11 00 01 00 11 00 10 10 00
11 01 11 11 01 10 01 11 01 10 00 01 10 01 01 01 11 11 01 10 11 11 01 01 10 10 11 01 00 00 10 01 10 00 11 01 11 11 00 11 11 00 00 00 00 10 01 10 10 00 11 00 01 10 01 11 10 00 01 01 11 11 11 01 11 00 11 11 01 00 01 01
00 00 11 11 01 11 11 11 00 00 00 01 10 11 10 00 00 11 10 11 01 11 10 10 01 01 11 01 01 01 01 01 10 01 11 11 01 11 00 10 10 00 01 11 10 11 10 11 10 10 10 00 11 00 11 11 00 11 10 11 10 01 00 00 01 10 10 00 11 01 10 11
11 11 10 10 01 01 11 10 10 00 11 10 01 00 01 00 01 01 10 11 01 00 00 10 10 11 10 01 01 10 01 00 00 01 00 11 01 00 10 00 01 11 11 00 11 10 01 01 00 00 00 10 10 10 01 01 00 01 01 01 00 00 00 10 11 11 11 10 00 01 11 01
00 10 11 11 00 01 11 00 00 00 00 00 10 00 11 11 00 11 01 10 10 01 01 10 11 11 11 10 11 10 11 01 10 01 10 10 00 11 10 10 11 01 01 01 00 10 10 01 11 00 10 11 11 11 11 11 01 01 10 11 10 00 11 11 00 00 01 00 01 01 10 10
01 01 00 11 10 10 11 00 01 10 01 01 01 01 00 11 01 01 11 00 00 11 10 01 10 10 01 00 00 00 01 10 10 11 00 01 00 00 01 00 01 00 00 10 11 10 10 10 01 00 11 00 01 00 11 11 01 11 10 01 01 01 01 01 00 00 11 11 00 10 10 01
01 11 11 00 11 11 11 00 11 01 11 10 01 10 01 00 00 11 01 01 10 11 10 10 00 00 01 10 11 01 00 10 11 11 11 11 11 10 00 11 00 00 11 11 00 00 11 01 11 10 00 00 11 10 00 11 01 01 11 00 11 00 11 11 10 11 00 11 10 10 10 00 Mass: 13 mm
00 10 01 10 01 01 10 01 00 00 10 00 01 11 00 10 00 00 11 01 10 00 00 00 11 01 01 01 10 00 11 00 11 00 10 10 11 10 00 11 10 10 11 11 01 01 10 10 01 01 01 10 10 11 10 00 11 10 10 00 10 10 11 00 11 01 10 00 01 11 10 11
01 11 00 01 01 00 11 01 10 11 00 01 11 10 11 10 11 00 01 10 00 01 10 11 00 00 11 10 11 00 00 01 11 00 01 11 11 10 10 00 11 01 11 11 01 11 00 10 01 00 00 01 01 01 11 00 11 10 00 10 00 01 01 01 10 10 01 01 00 01 10 10 Characteristics: Solid
00 00 00 00 10 10 11 10 00 00 10 00 10 00 00 01 10 00 01 10 00 00 10 10 11 10 01 00 11 10 10 01 00 11 00 01 11 01 01 00 00 00 11 01 11 10 01 01 10 11 01 10 10 10 01 10 10 00 11 10 01 10 01 10 10 01 11 01 10 00 10 01
01 10 01 10 01 01 11 01 11 00 01 11 11 00 10 11 11 01 00 00 10 11 11 10 11 11 01 01 10 01 01 11 11 10 10 00 11 00 01 01 01 11 10 10 00 01 10 10 00 11 01 00 00 01 01 01 00 00 11 00 01 01 01 01 01 01 00 10 00 00 11 00
00 10 10 10 01 00 11 00 01 00 00 11 00 01 00 01 11 11 01 00 00 10 01 01 11 10 11 01 10 01 01 10 10 00 01 00 10 10 11 10 01 10 11 10 10 11 11 11 10 00 10 01 01 10 01 00 11 11 11 11 11 00 01 01 11 00 00 01 01 11 10 10
Change: +20%
Chest CT Scan 100101011000100101100100111111110110011011010010010000110011001001001101
101100000000000000111111011110100101100101010101111000000110011111001001
101000110100011000110101101111110001010100001110101010111011101000010111
000011010110010101010110100011000111001101111001110101011001110111100110
001101000110010010111110110101001010100001111010010101011101101100000111
111001101111101001110100100011010011010100110101011101100010100011001110
110100110110111000001010011011101111101100000011001000101101100100110110
101011011000111010010101100001001010010010110010100110101011110101110010
100000101010000110110110010010000011101000010110110001011101011100000000
000001110110110001011111000011100000000000000101100000100100110111001000
011010110100101001000100110100101100100010001100001011011111111110101001
111111100101100011001000010110110000101000111101110110010000110101110101
!
010101001110001000111101110011011001000001010000010010010100010100100110
101100010101101000100101100010001000111111111100101101000000010011001010
001000010100011110000100011111000110110011000100101011101010000000011000
Localization and
010100100011100010100010001011011010000111010010010000010001011111000011
111111000010111110001010000100000001011110110010101100001111000101110000 Spiculated mass, quantification of
101100111010101011001101101100011011011101111100101011011101011110011011
110000000101010010010110100010000001010001100101011011111100110101001000
mid-right breast abnormalities
1 0 0 0 0 1 1 0 0 0 0 1 1 1 0 1 0 0 0 0 0 1 0 1 1 1 0 0 0 0 1 1 1 1 1 1 0 1 1 1 1 1 0 1 1 1 0 1 1 0 1 00 0 0 0 0 0 1 0 0 0 1 1 1 0 0 0 0 1 1 1
001101011011000011010111101011101111100111010111000111100100100000000001
000010011100000011011100100100111111011101000000000110000001100100010110
111110111001011111101111001100010011110110000010001010110011111110111011
001111110001010001011100111111110111110000110101000010110101010010001101
110011100010101011011000010110100101100011101011000000110111000011100111
011100100000101101011001111111101011011110000110101111110011101100000011
000111100100000100100110110000011100000000011111001000110110000000110110
011011101011010001001111000110011111110100110010110011010010101111011110
010100100010010100101000100010101011110111110011000111101110111010100111
010000101100111110010011001110001001111010110101000000101101000011000011
000011110010100010010011110011100100100000101100110111011011010110101010
Mass: 4 cm2
010100101001101110001111110010011110100001110011010000000010000000010010
000010101001010111100011101101100010001010100111000110101111101110011100 Characteristics:
Mammogram Spiculated solid mass
Microcalcifications present
Architectural distortion present
Likelihood of cancer: 7 in 10
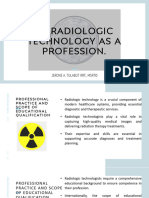
Figure 1. Current Uses of Artificial Intelligence (AI) in Radiology.
Shown are common clinical AI solutions for the functions of triage, detection, and diagnosis with CADt (computer-aided detection for
triage), CADe (computer-aided detection for characterizing abnormalities), and CADx (computer-aided detection for diagnosis). Other
AI applications for radiology include image reconstruction and noise reduction. Applications for nonimaging tasks are not shown. CT
denotes computed tomography.
Radiologic AI has attracted global interest, patients. However, radiologists have expressed
and commercial AI algorithms have been devel- concerns about lack of knowledge, lack of trust,
oped by companies based in more than 20 coun- and changes in professional identity and auton-
tries. Studies have shown that some hospitals, as omy.26 Local champions of AI, education, train-
well as other point-of-care centers, already use ing, and support can help overcome these con-
AI products successfully, and larger practices are cerns. The majority of radiologists and residents
more likely than smaller practices to use AI cur- expect substantial changes in the radiology pro-
rently. Radiologists who use AI in their practices fession within the next decade and believe that
are generally satisfied with their experience and AI should have a role as a “co-pilot,” acting as a
find that AI provides value to them and their second reader and improving workflow tasks.27
n engl j med 388;21 nejm.org May 25, 2023 1983
The New England Journal of Medicine
Downloaded from nejm.org by Adrian H. Aguilera on August 24, 2023. For personal use only. No other uses without permission.
Copyright © 2023 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
Although the penetration of AI in the U.S. mar- phones in AI-enabled applications can be used
ket is currently estimated to be only 2%, the to obtain diagnostic information even by users
readiness of radiologists and the potential of the without formal training in echocardiography or
technology indicate that further translation into the use of ultrasound in obstetrical care.37 Over-
clinical practice is likely to occur. all, although the use of medical-imaging AI by
nonradiologist clinicians is still in the early
Emerging Uses for Nonradiologists stages, it has the potential to revolutionize ac-
Although many current radiologic AI applica- cess to medical imaging and improve patient
tions are designed for radiologists, there is a outcomes.
small but emerging trend globally toward the
use of medical-imaging AI for nonradiologist S a fegua r ds for Effec t i v e
clinicians and other stakeholders (i.e., health care Gener a l i z at ion
providers and patients). This trend presents an
opportunity for improving access to medical In considering the widespread adoption of AI
imaging and reducing common diagnostic er- algorithms in radiology, a critical question aris-
rors28 in low-resource settings and emergency es: Will they work for all patients? The models
departments, where there is often a lack of underlying specific AI applications are often not
around-the-clock radiology coverage.29 For in- tested outside the setting in which they were
stance, one study showed that an AI system for trained, and even AI systems that receive FDA
chest radiograph interpretation, when combined approval are rarely tested prospectively or in
with input from a nonradiology resident, had multiple clinical settings.38 Very few random-
performance values that were similar to those ized, controlled trials have shown the safety and
for board-certified radiologists.30 A popular AI effectiveness of existing AI algorithms in radiol-
application that is targeted for use by nonradi- ogy, and the lack of real-world evaluation of AI
ologist clinicians for detecting large-vessel oc- systems can pose a substantial risk to patients
clusions in the central nervous system has re- and clinicians.39
sulted in a significant reduction in time to Moreover, studies have shown that the per-
intervention and improved patient outcomes.31 formance of many radiologic AI models worsens
Moreover, AI has been shown to accelerate when they are applied to patients who differ
medical-imaging acquisition outside traditional from those used for model development, a phe-
referral workflows with new, clinician-focused nomenon known as “data set shift.”40-44 In inter-
mobile applications for notifications of AI re- pretation of medical images, data set shift can
sults.32 This trend, although not well estab- occur as a result of various factors, such as dif-
lished, has been cited as a potential long-term ferences in health care systems, patient popula-
threat to radiology as a specialty because ad- tions, and clinical practices.45 For instance, the
vanced AI models may reduce the complexity of performance of models for brain tumor segmen-
technical interpretation so that a nonradiologist tation and chest radiograph interpretation wors-
clinician could use imaging without relying on a ens when the models are validated on external
radiologist.33,34 data collected at hospitals other than those used
Portable and inexpensive imaging techniques for model training.46,47 In another example, a ret-
are frequently supported by AI and have served rospective study showed that the performance of
to lower the barrier for more widespread clinical a commercial AI model in detecting cervical spine
use of AI in medical imaging outside the tradi- fractures was worse in real-world practice than
tional radiology workflow.35,36 For example, the the performance initially reported to the FDA.48
Swoop portable MRI system, a point-of-care de- Patient age, fracture characteristics, and degen-
vice that addresses existing limitations in forms erative changes in the spine affected the sensi-
of imaging technology, provides accessibility tivity and false positive rates to an extent that
and maneuverability for a range of clinical ap- limited the clinical usefulness of the AI model
plications. The system plugs into a standard and aroused concerns about the generalization
electrical outlet and is controlled by an Apple of radiologic AI algorithms across clinical envi-
iPad. Portable ultrasound probes and smart- ronments.
1984 n engl j med 388;21 nejm.org May 25, 2023
The New England Journal of Medicine
Downloaded from nejm.org by Adrian H. Aguilera on August 24, 2023. For personal use only. No other uses without permission.
Copyright © 2023 Massachusetts Medical Society. All rights reserved.
Using AI to Interpret Medical Images
There is a pressing need for the development
of methods that improve the generalization of
algorithms in new settings.49-51 As the field ma-
tures, better generalization checks based on ac-
ta
cepted standards must be established before the da Fa
cto
Re
of
algorithms are widely applied. These checks en- rs
al-
se
Cli
wo
nic
ea
sts
compass three related areas: clinician–AI collabo-
aff
i
rel
rld
kli
ec
c
lic
an
eva
ti
cy
ration, transparency, and monitoring (Fig. 2).
he
ng
–A
pub
en
gc
luat
dec
r
IC
spa
rtin
and
ion
olla
ision
Tran
Repo
Clinician–AI Collaboration
borat
Curation
making
The successful use of AI in radiology depends on
ion
Safeguards for
effective clinician–AI collaboration. In theory, Effective
the use of AI algorithms to assist radiologists Generalization
allows for a human–AI collaboration workflow,
with humans and AI leveraging complementary
strengths.52 Studies have shown that AI assis-
tance in interpretation of medical images is more
Po
useful to some clinicians than to others and std
e p lo y o ri n
g
m e n t M o nit
generally provides more benefit to less experi-
enced clinicians.53,54 C o n ti n
u al le a r n in g
Despite some evidence that clinicians receiv- C li n i ci a n f e e d b a c k
ing AI assistance can achieve better performance
than unassisted clinicians,53,55,56 the body of re-
search on human–AI collaboration for image Figure 2. Generalization Checks for AI Systems in Radiology.
interpretation offers mixed evidence regarding The three essential components of generalization checks for radiologic AI
the value of such a collaboration. Results vary systems are clinician–AI collaboration, transparency, and postdeployment
according to particular metrics, tasks, and the monitoring. Clinician–AI collaboration reflects the need to move from eval‑
study cohorts in question, with studies showing uations of the stand-alone performance of AI models to evaluations of
that although AI can improve the performance their value as assistive tools in real-world clinical workflows. Transparency
with regard to lack of information about an AI model requires greater rigor
of radiologists, sometimes AI alone performs through the use of checklists and public release of medical-imaging data
better than a radiologist using AI.57,58 sets. Postdeployment monitoring involves mechanisms to incorporate
Many AI methods are “black boxes,” meaning feedback from clinicians and continual learning strategies for regular up‑
that their decision-making processes are not dating of the models.
easily interpretable by humans; this can pose
challenges for clinicians trying to understand
and trust the recommendations of AI.59 Studies medical imaging. Scientific, peer-reviewed evi-
of the potential for explainable AI methods to dence of efficacy is lacking for most commer-
build trust in clinicians have shown mixed re- cially available AI products.38 Many published
sults.59,60 Therefore, there is a need to move from
reports on FDA-cleared devices omit informa-
evaluations centered on the stand-alone perfor- tion on sample size, demographic characteristics
mance of models to evaluations centered on the of patients, and specifications of the equipment
outcomes when these algorithms are used as used to acquire the images to be interpreted. In
assistive tools in real-world clinical workflows.
addition, only a fraction of device studies offer
This approach will enable us to better under- data on the specific demographic subgroups
stand the effectiveness and limitations of AI inused during algorithm training, as well as the
clinical practice and establish safeguards for diagnostic performance of these algorithms
effective clinician–AI collaboration. when applied to patients from underrepresented
demographic subgroups. This lack of informa-
Transparency tion makes it difficult to determine the general-
Transparency is a major challenge in evaluating izability of AI and machine-learning algorithms
the generalization behavior of AI algorithms in across different patient populations.
n engl j med 388;21 nejm.org May 25, 2023 1985
The New England Journal of Medicine
Downloaded from nejm.org by Adrian H. Aguilera on August 24, 2023. For personal use only. No other uses without permission.
Copyright © 2023 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
The limited independent validation of these Gener a l is t Medic a l A I Model s
models has generated a call for greater transpar- for R a diol o gy
ency and rigor with the use of checklists to ver-
ify the proper implementation of AI models in The current generation of AI models in radiol-
medical imaging and to ensure adequate repro- ogy can handle only a limited set of interpreta-
ducibility and clinical effectiveness.61-63 One solu- tion tasks, and they rely heavily on curated data
tion for transparency is the curation and public that have been specifically labeled and catego-
release of medical-imaging data sets to serve as rized.81 Although focusing on the image as an
a common benchmark and show algorithm per- isolated model input has some value, it does
formance.64-67 The availability of publicly re- not reflect the true cognitive work of radiology,
leased chest radiograph data sets has already which involves interpreting medical-imaging
provided support for marked advances in im- examinations comprehensively, comparing cur-
proving AI validation.68,69 However, there are rent and previous examinations,82 and synthe-
challenges in curating public medical-imaging sizing this information with clinical contextual
data sets, including privacy concerns about shar- data to make diagnostic and management rec-
ing data,70 costs of data infrastructure,71 and over- ommendations.83,84 The narrow focus of exist-
representation of data from academic medical ing AI solutions on interpretation of individual
centers with substantial resources.72 Federated images in isolation has contributed to the limit-
learning, another approach to data sharing, in- ed penetration of radiologic AI applications in
volves training an AI model on decentralized practice.
data sources without transferring the data to a However, there is a trend toward a more com-
central repository.73,74 Streamlined processes for prehensive approach to the development of ra-
curating and sharing diverse medical data sets diologic AI, with the aim of providing more
are necessary for transparency in establishing value than simply automating individual inter-
clinical usefulness. pretation tasks. Recently developed models can
identify dozens or even hundreds of findings on
Postdeployment Monitoring chest radiographs and brain CT scans obtained
Even after a model is deployed, its performance without contrast material,85 and they can provide
in the real world may degrade over time. In inter- radiologists with specific details about each
pretation of medical images, these shifts can finding. More and more companies are offering
occur as a result of various factors such as AI solutions that address the entire diagnostic
changes in disease prevalence, advances in med- and clinical workf low for conditions such as
ical technology, and alterations in clinical prac- stroke and cancer, from screening to direct
tices.38,75-77 Failure to update the model to reflect clinical referrals and follow-up. Although these
these changes can lead to poor model perfor- comprehensive AI solutions may make it easier
mance and misuse. However, regulatory require- for medical professionals to implement and use
ments may restrict updating of models after they the technology, the issues of validation and trans-
have been approved. parency remain a concern.
Continuous monitoring of model performance A new generation of generalist medical AI
and proactive measures to address data set shifts models with the potential to tackle the entire
over time can improve the accuracy and reliabil- task of radiologic image interpretation and more
ity of AI models in medical-imaging interpreta- is on the horizon.86 These models will be capa-
tion. Regular updates of the training data and ble of accurately generating the full radiologic
retraining of the model on new data through report by interpreting a wide range of findings
continual learning can help maintain model per- with degrees of uncertainty and specificity based
formance over time.78 In addition, incorporating on the image, by fusing the clinical context with
feedback from clinicians can help improve the the imaging data, and by leveraging previous
performance of the model by providing real- imaging in the decision of the model.84,87-91 This
world insights and identifying areas for im- comprehensive approach is more closely aligned
provement. Ultimately, postdeployment monitor- with the overall cognitive work in radiology.
ing is essential to ensure that AI models remain Early studies of such models have shown that
effective and reliable in clinical settings.79,80 they can detect several diseases on images at an
1986 n engl j med 388;21 nejm.org May 25, 2023
The New England Journal of Medicine
Downloaded from nejm.org by Adrian H. Aguilera on August 24, 2023. For personal use only. No other uses without permission.
Copyright © 2023 Massachusetts Medical Society. All rights reserved.
Using AI to Interpret Medical Images
Nonimaging Data
E.g., sensor data, omics data, test results
Radiologist
Medical Imaging
E.g., radiograph, CT scan, mammogram
Customized
Generalist
Interactive
Medical AI
Reports
Model
Physician
Clinical History
Patient
Figure 3. Potential of Generalist Medical AI Models in Radiology.
Generalist medical AI models have great potential for transforming radiology. These models can produce complete
radiologic reports containing interpretive and descriptive findings derived from various sources such as imaging,
clinical context, and previous imaging. They could also potentially link specific image regions with language descrip‑
tions, adjust to end users, and generate findings within an interpretive context. In addition, these models may pos‑
sess the ability to adapt to new environments and technological advancements. “Omics” data are derived from studies
such as genomics, epigenomics, proteomics, and metabolomics.
expert level without requiring further annotation, specific needs of various end users, and will en-
a capability known as zero-shot learning.92 able personalized recommendations and natural-
Rapid developments in AI models, including language interactions on the imaging study. For
self-supervised models,92,93 multimodal models,82 instance, given a medical image and relevant
foundation models, and particularly large lan- clinical information, the model will produce a
guage models for text data and for combined complete radiologic report for the radiologist,98
image and text data,94,95 have the potential to a patient-friendly report with easy-to-understand
accelerate progress in this area. Large language descriptions in the preferred language for the
models are AI models consisting of a neural net- patient, recommendations regarding a surgical
work with billions of weights or more, trained approach that are based on best practices for the
on large amounts of unlabeled data. Early studies surgeon, and evidence-based follow-up sugges-
of large language models for text-based tasks in tions and tests for the primary care provider —
medicine have included chatbots such as GPT-4 all derived from the imaging and clinical data by
(Generative Pre-trained Transformer 4) and have a single generalist model (Fig. 3). In addition,
shown that these models are capable of clinical these models may be able to generalize easily to
expert–level medical note-taking, question an- new geographic locations, patient populations,
swering, and consultation.96,97 We anticipate that disease distributions, and changes in imaging
future AI models will be able to process imaging technology without requiring substantial engineer-
data, speech, and medical text and generate out- ing effort or more than a handful of new data.99
puts such as free-text explanations, spoken rec- Given the capabilities of large language mod-
ommendations, and image annotations that re- els, training new multimodal large language
flect advanced medical reasoning. These models models with large quantities of real-world medi-
will be able to generate tailored text outputs cal imaging and clinical text data, although
based on medical-image inputs, catering to the challenging, holds promise in ushering in trans-
n engl j med 388;21 nejm.org May 25, 2023 1987
The New England Journal of Medicine
Downloaded from nejm.org by Adrian H. Aguilera on August 24, 2023. For personal use only. No other uses without permission.
Copyright © 2023 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
formative capabilities of radiologic AI. However,Radiology has witnessed the adoption of these
the extent to which such models can exacerbate tools in everyday clinical practice, albeit with a
the extant problems with widespread validation modest impact thus far. The discrepancy be-
remains unknown and is an important area for tween the anticipated and actual impact can be
study and concern. Overall, the potential for attributed to various factors, such as the absence
generalist medical AI models to provide compre- of data from prospective real-world studies, lim-
hensive solutions to the task of interpretation of
ited generalizability, and the scarcity of compre-
radiologic images and beyond is likely to trans- hensive AI solutions for image interpretation. As
form not only the field of radiology but also health care professionals increasingly use radio-
health care more broadly. logic AI and as large language models continue
to evolve, the future of AI in medical imaging
appears bright. However, it remains uncertain
C onclusions
whether the traditional practice of radiology, in its
AI is a prime instance of a technological break- current form, will share this promising outlook.
through that has widespread current and future Disclosure forms provided by the authors are available with
possibilities in the field of medical imaging. the full text of this article at NEJM.org.
References
1. Rajpurkar P, Chen E, Banerjee O, think: radiology’s next frontier. Radiology 21. Pease M, Arefan D, Barber J, et al.
Topol EJ. AI in health and medicine. Nat 2017;285:713-8. Outcome prediction in patients with se-
Med 2022;28:31-8. 12. European Society of Radiology (ESR). vere traumatic brain injury using deep
2. Jones OT, Matin RN, van der Schaar Current practical experience with artifi- learning from head CT scans. Radiology
M, et al. Artificial intelligence and ma- cial intelligence in clinical radiology: 2022;304:385-94.
chine learning algorithms for early detec- a survey of the European Society of Radi- 22. Jiang Y, Zhang Z, Yuan Q, et al. Pre-
tion of skin cancer in community and ology. Insights Imaging 2022;13:107. dicting peritoneal recurrence and disease-
primary care settings: a systematic re- 13. Allen B, Agarwal S, Coombs L, Wald free survival from CT images in gastric
view. Lancet Digit Health 2022;4(6):e466- C, Dreyer K. 2020 ACR Data Science Insti- cancer with multitask deep learning:
e476. tute artificial intelligence survey. J Am a retrospective study. Lancet Digit Health
3. Siontis KC, Noseworthy PA, Attia ZI, Coll Radiol 2021;18:1153-9. 2022;4(5):e340-e350.
Friedman PA. Artificial intelligence- 14. Yuba M, Iwasaki K. Systematic analy- 23. Lee MH, Zea R, Garrett JW, Graffy
enhanced electrocardiography in cardio- sis of the test design and performance PM, Summers RM, Pickhardt PJ. Abdomi-
vascular disease management. Nat Rev of AI/ML-based medical devices approved nal CT body composition thresholds us-
Cardiol 2021;18:465-78. for triage/detection/diagnosis in the USA ing automated AI tools for predicting
4. Lu MY, Chen TY, Williamson DFK, and Japan. Sci Rep 2022;12:16874. 10-year adverse outcomes. Radiology 2023;
et al. AI-based pathology predicts origins 15. Tariq A, Purkayastha S, Padmanaban 306(2):e220574.
for cancers of unknown primary. Nature GP, et al. Current clinical applications of 24. Pickhardt PJ, Graffy PM, Perez AA,
2021;594:106-10. artificial intelligence in radiology and Lubner MG, Elton DC, Summers RM. Op-
5. Abràmoff MD, Cunningham B, Patel their best supporting evidence. J Am Coll portunistic screening at abdominal CT:
B, et al. Foundational considerations for Radiol 2020;17:1371-81. use of automated body composition bio-
artificial intelligence using ophthalmic 16. Richardson ML, Garwood ER, Lee Y, markers for added cardiometabolic value.
images. Ophthalmology 2022;129(2):e14- et al. Noninterpretive uses of artificial in- Radiographics 2021;41:524-42.
e32. telligence in radiology. Acad Radiol 2021; 25. Yuan N, Kwan AC, Duffy G, et al. Pre-
6. Nam JG, Hwang EJ, Kim J, et al. AI 28:1225-35. diction of coronary artery calcium using
improves nodule detection on chest radio- 17. Wang G, Ye JC, De Man B. Deep learn- deep learning of echocardiograms. J Am
graphs in a health screening population: ing for tomographic image reconstruc- Soc Echocardiogr 2022 December 23
a randomized controlled trial. Radiology tion. Nat Mach Intell 2020;2:737-48. (Epub ahead of print).
2023;307(2):e221894. 18. Tao Q, Yan W, Wang Y, et al. Deep 26. Huisman M, Ranschaert E, Parker W,
7. Eng D, Chute C, Khandwala N, et al. learning-based method for fully automat- et al. An international survey on AI in ra-
Automated coronary calcium scoring us- ic quantification of left ventricle function diology in 1041 radiologists and radiol-
ing deep learning with multicenter exter- from cine MR images: a multivendor, ogy residents part 2: expectations, hurdles
nal validation. NPJ Digit Med 2021;4:88. multicenter study. Radiology 2019;290: to implementation, and education. Eur
8. Astuto B, Flament I, K Namiri N, et al. 81-8. Radiol 2021;31:8797-806.
Automatic deep learning-assisted detec- 19. Elijovich L, Dornbos Iii D, Nickele C, 27. Strohm L, Hehakaya C, Ranschaert
tion and grading of abnormalities in knee et al. Automated emergent large vessel oc- ER, Boon WPC, Moors EHM. Implemen-
MRI studies. Radiol Artif Intell 2021;3(3): clusion detection by artificial intelligence tation of artificial intelligence (AI) appli-
e200165. improves stroke workflow in a hub and cations in radiology: hindering and fa-
9. LeCun Y, Bengio Y, Hinton G. Deep spoke stroke system of care. J Neurointerv cilitating factors. Eur Radiol 2020; 30:
learning. Nature 2015;521:436-44. Surg 2022;14:704-8. 5525-32.
10. Brady AP. The vanishing radiologist 20. Hillis JM, Bizzo BC, Mercaldo S, et al. 28. Yang D, Fineberg HV, Cosby K. Diag-
— an unseen danger, and a danger of Evaluation of an artificial intelligence nostic excellence. JAMA 2021;326:1905-6.
being unseen. Eur Radiol 2021;31:5998- model for detection of pneumothorax and 29. Schwalbe N, Wahl B. Artificial intel-
6000. tension pneumothorax in chest radiographs. ligence and the future of global health.
11. Dreyer KJ, Geis JR. When machines JAMA Netw Open 2022;5(12):e2247172. Lancet 2020;395:1579-86.
1988 n engl j med 388;21 nejm.org May 25, 2023
The New England Journal of Medicine
Downloaded from nejm.org by Adrian H. Aguilera on August 24, 2023. For personal use only. No other uses without permission.
Copyright © 2023 Massachusetts Medical Society. All rights reserved.
Using AI to Interpret Medical Images
30. Rudolph J, Huemmer C, Ghesu F-C, with multi-site imaging data: an empiri- 56. Ahn JS, Ebrahimian S, McDermott S,
et al. Artificial intelligence in chest radi- cal study on the impact of scanner effects. et al. Association of artificial intelligence-
ography reporting accuracy: added clini- In:Proceedings and abstracts of the Med- aided chest radiograph interpretation
cal value in the emergency unit setting ical Imaging Meets NeurIPS Workshop, with reader performance and efficiency.
without 24/7 radiology coverage. Invest December 14, 2019. Vancouver:Neural JAMA Netw Open 2022;5(8):e2229289.
Radiol 2022;57:90-8. Information Processing Systems, 2019. 57. Seah JCY, Tang CHM, Buchlak QD,
31. Karamchandani RR, Helms AM, Saty- 43. Koh PW, Sagawa S, Marklund H, et al. et al. Effect of a comprehensive deep-
anarayana S, et al. Automated detection of WILDS: a benchmark of in-the-wild dis- learning model on the accuracy of chest
intracranial large vessel occlusions using tribution shifts. In:Proceedings of the x-ray interpretation by radiologists: a ret-
Viz.ai software: experience in a large, inte- 38th International Conference on Ma- rospective, multireader multicase study.
grated stroke network. Brain Behav 2023; chine Learning, July 18–24, 2021. Virtual: Lancet Digit Health 2021;3(8):e496-e506.
13(1):e2808. International Conference on Machine 58. Rajpurkar P, O’Connell C, Schechter
32. Mazurek MH, Cahn BA, Yuen MM, Learning, 2021. A, et al. CheXaid: deep learning assis-
et al. Portable, bedside, low-field mag- 44. Hsu W, Hippe DS, Nakhaei N, et al. tance for physician diagnosis of tubercu-
netic resonance imaging for evaluation of External validation of an ensemble model losis using chest x-rays in patients with
intracerebral hemorrhage. Nat Commun for automated mammography interpreta- HIV. NPJ Digit Med 2020;3:115.
2021;12:5119. tion by artificial intelligence. JAMA Netw 59. Saporta A, Gui X, Agrawal A, et al.
33. Brink JA, Hricak H. Radiology 2040. Open 2022;5(11):e2242343. Benchmarking saliency methods for chest
Radiology 2023;306:69-72. 45. Wynants L, Van Calster B, Collins GS, X-ray interpretation. Nat Mach Intell 2022;
34. Lee HW, Jin KN, Oh S, et al. Artificial et al. Prediction models for diagnosis and 4:867-78.
intelligence solution for chest radiographs prognosis of covid-19: systematic review 60. Gaube S, Suresh H, Raue M, et al.
in respiratory outpatient clinics: multi- and critical appraisal. BMJ 2020; 369: Non-task expert physicians benefit from
center prospective randomized study. Ann m1328. correct explainable AI advice when review-
Am Thorac Soc 2022 December 12 (Epub 46. AlBadawy EA, Saha A, Mazurowski ing X-rays. Sci Rep 2023;13:1383.
ahead of print). MA. Deep learning for segmentation of 61. Mongan J, Moy L, Kahn CE Jr. Check-
35. Narang A, Bae R, Hong H, et al. Util- brain tumors: impact of cross-institu- list for Artificial Intelligence in Medical
ity of a deep-learning algorithm to guide tional training and testing. Med Phys Imaging (CLAIM): a guide for authors and
novices to acquire echocardiograms for 2018;45:1150-8. reviewers. Radiol Artif Intell 2020; 2(2):
limited diagnostic use. JAMA Cardiol 47. Rajpurkar P, Joshi A, Pareek A, Ng AY, e200029.
2021;6:624-32. Lungren MP. CheXternal: generalization 62. Liu X, Rivera SC, Moher D, Calvert
36. Pokaprakarn T, Prieto JC, Price JT, et al. of deep learning models for chest X-ray MJ, Denniston AK. Reporting guidelines
AI estimation of gestational age from interpretation to photos of chest X-rays for clinical trial reports for interven-
blind ultrasound sweeps in low-resource and external clinical settings. In:Pro- tions involving artificial intelligence: the
settings. NEJM Evid 2022; 1(5). DOI: ceedings of the Conference on Health, CONSORT-AI Extension. BMJ 2020;370:
10.1056/EVIDoa2100058. Inference, and Learning, April 8–10, 2021. m3164.
37. Baribeau Y, Sharkey A, Chaudhary O, New York:Association for Computing 63. Cruz Rivera S, Liu X, Chan A-W, et al.
et al. Handheld point-of-care ultrasound Machinery, 2021. Guidelines for clinical trial protocols for
probes: the new generation of POCUS. 48. Voter AF, Larson ME, Garrett JW, Yu interventions involving artificial intelli-
J Cardiothorac Vasc Anesth 2020;34:3139- JJ. Diagnostic accuracy and failure mode gence: the SPIRIT-AI extension. Nat Med
45. analysis of a deep learning algorithm for 2020;26:1351-63.
38. Wu E, Wu K, Daneshjou R, Ouyang D, the detection of cervical spine fractures. 64. Irvin J, Rajpurkar P, Ko M, et al.
Ho DE, Zou J. How medical AI devices are AJNR Am J Neuroradiol 2021;42:1550-6. CheXpert: a large chest radiograph data-
evaluated: limitations and recommenda- 49. Guan H, Liu M. Domain adaptation set with uncertainty labels and expert
tions from an analysis of FDA approvals. for medical image analysis: a survey. IEEE comparison. In:Proceedings and abstracts
Nat Med 2021;27:582-4. Trans Biomed Eng 2022;69:1173-85. of the 33rd AAAI Conference on Artificial
39. Plana D, Shung DL, Grimshaw AA, 50. Castro DC, Walker I, Glocker B. Cau- Intelligence, January 27–February 1, 2019.
Saraf A, Sung JJY, Kann BH. Randomized sality matters in medical imaging. Nat Honolulu:Association for the Advance-
clinical trials of machine learning inter- Commun 2020;11:3673. ment of Artificial Intelligence, 2019.
ventions in health care: a systematic re- 51. Feng Y, Xu X, Wang Y, et al. Deep su- 65. Johnson AEW, Pollard TJ, Berkowitz
view. JAMA Netw Open 2022;5(9):e2233946. pervised domain adaptation for pneumo- SJ, et al. MIMIC-CXR, a de-identified pub-
40. Pooch EHP, Ballester PL, Barros RC. nia diagnosis from chest X-ray images. licly available database of chest radio-
Can we trust deep learning models diag- IEEE J Biomed Health Inform 2022;26: graphs with free-text reports. Sci Data
nosis? The impact of domain shift in 1080-90. 2019;6:317.
chest radiograph classification. In:Pro- 52. Langlotz CP. Will artificial intelli- 66. Bustos A, Pertusa A, Salinas J-M, de la
ceedings and abstracts of the Second In- gence replace radiologists? Radiol Artif Iglesia-Vayá M. PadChest: a large chest
ternational Workshop on Thoracic Image Intell 2019;1(3):e190058. x-ray image dataset with multi-label an-
Analysis, October 8, 2020. Lima, Peru: 53. Park A, Chute C, Rajpurkar P, et al. notated reports. Med Image Anal 2020;
Medical Image Computing and Computer Deep learning-assisted diagnosis of cere- 66:101797.
Assisted Intervention Society, 2020. bral aneurysms using the HeadXNet model. 67. Nguyen HQ, Lam K, Le LT, et al. VinDr-
41. Cohen JP, Hashir M, Brooks R, Ber- JAMA Netw Open 2019;2(6):e195600. CXR: an open dataset of chest X-rays with
trand H. On the limits of cross-domain 54. Tschandl P, Rinner C, Apalla Z, et al. radiologist’s annotations. Sci Data 2022;
generalization in automated X-ray predic- Human-computer collaboration for skin 9:429.
tion. In:Proceedings and abstracts of the cancer recognition. Nat Med 2020; 26: 68. Larrazabal AJ, Nieto N, Peterson V,
Third Conference on Medical Imaging 1229-34. Milone DH, Ferrante E. Gender imbalance
with Deep Learning, July 6–8, 2020. Mon- 55. Bien N, Rajpurkar P, Ball RL, et al. in medical imaging datasets produces bi-
treal:Medical Imaging with Deep Learn- Deep-learning-assisted diagnosis for knee ased classifiers for computer-aided diag-
ing Foundation, 2020. magnetic resonance imaging: develop- nosis. Proc Natl Acad Sci U S A 2020;117:
42. Glocker B, Robinson R, Castro DC, ment and retrospective validation of 12592-4.
Dou Q, Konukoglu E. Machine learning MRNet. PLoS Med 2018;15(11):e1002699. 69. Seyyed-Kalantari L, Zhang H, McDer-
n engl j med 388;21 nejm.org May 25, 2023 1989
The New England Journal of Medicine
Downloaded from nejm.org by Adrian H. Aguilera on August 24, 2023. For personal use only. No other uses without permission.
Copyright © 2023 Massachusetts Medical Society. All rights reserved.
Using AI to Interpret Medical Images
mott MBA, Chen IY, Ghassemi M. Under- 80. Pianykh OS, Langs G, Dewey M, et al. 90. Kather JN, Ghaffari Laleh N, Foersch
diagnosis bias of artificial intelligence Continuous learning AI in radiology: im- S, Truhn D. Medical domain knowledge in
algorithms applied to chest radiographs plementation principles and early applica- domain-agnostic generative AI. NPJ Digit
in under-served patient populations. Nat tions. Radiology 2020;297:6-14. Med 2022;5:90.
Med 2021;27:2176-82. 81. Willemink MJ, Koszek WA, Hardell C, 91. Huang S-C, Pareek A, Zamanian R,
70. Seastedt KP, Schwab P, O’Brien Z, et al. et al. Preparing medical imaging data for Banerjee I, Lungren MP. Multimodal fu-
Global healthcare fairness: we should be machine learning. Radiology 2020; 295: sion with deep neural networks for lever-
sharing more, not less, data. PLOS Digit 4-15. aging CT imaging and electronic health
Health 2022;1(10):e0000102. 82. Acosta JN, Falcone GJ, Rajpurkar P. record: a case-study in pulmonary embo-
71. Panch T, Mattie H, Celi LA. The “in- The need for medical artificial intelli- lism detection. Sci Rep 2020;10:22147.
convenient truth” about AI in healthcare. gence that incorporates prior images. Ra- 92. Tiu E, Talius E, Patel P, Langlotz CP,
NPJ Digit Med 2019;2:77. diology 2022;304:283-8. Ng AY, Rajpurkar P. Expert-level detection
72. Kaushal A, Altman R, Langlotz C. 83. Larson DB, Froehle CM, Johnson ND, of pathologies from unannotated chest
Geographic distribution of US cohorts Towbin AJ. Communication in diagnostic X-ray images via self-supervised learning.
used to train deep learning algorithms. radiology: meeting the challenges of com- Nat Biomed Eng 2022;6:1399-406.
JAMA 2020;324:1212-3. plexity. AJR Am J Roentgenol 2014;203: 93. Krishnan R, Rajpurkar P, Topol EJ.
73. Sheller MJ, Edwards B, Reina GA, et al. 957-64. Self-supervised learning in medicine and
Federated learning in medicine: facilitat- 84. Huang S-C, Pareek A, Seyyedi S, Baner healthcare. Nat Biomed Eng 2022;6:1346-
ing multi-institutional collaborations with- jee I, Lungren MP. Fusion of medical im- 52.
out sharing patient data. Sci Rep 2020;10: aging and electronic health records using 94. Fei N, Lu Z, Gao Y, et al. Towards ar-
12598. deep learning: a systematic review and tificial general intelligence via a multi-
74. Pati S, Baid U, Edwards B, et al. Feder- implementation guidelines. NPJ Digit Med modal foundation model. Nat Commun
ated learning enables big data for rare 2020;3:136. 2022;13:3094.
cancer boundary detection. Nat Commun 85. Guo Y, He Y, Lyu J, et al. Deep learn- 95. Zhang S, Xu Y, Usuyama N, et al.
2022;13:7346. ing with weak annotation from diagnosis Large-scale domain-specific pretraining
75. Harvey HB, Gowda V. How the FDA reports for detection of multiple head dis- for biomedical vision-language process-
regulates AI. Acad Radiol 2020;27:58-61. orders: a prospective, multicentre study. ing. March 2, 2023 (http://arxiv.org/abs/
76. Lacson R, Eskian M, Licaros A, Ka- Lancet Digit Health 2022;4(8):e584-e593. 2303.00915). preprint.
poor N, Khorasani R. Machine learning 86. Moor M, Banerjee O, Abad ZSH, et al. 96. Singhal K, Azizi S, Tu T, et al. Large
model drift: predicting diagnostic imag- Foundation models for generalist medical language models encode clinical knowl-
ing follow-up as a case example. J Am Coll artificial intelligence. Nature 2023;616: edge. December 26, 2022 (http://arxiv.org/
Radiol 2022;19:1162-9. 259-65. abs/2212.13138). preprint.
77. Feng J, Phillips RV, Malenica I, et al. 87. Ramesh V, Chi NA, Rajpurkar P. Im- 97. Lee P, Bubeck S, Petro J. Benefits, lim-
Clinical artificial intelligence quality im- proving radiology report generation sys- its, and risks of GPT-4 as an AI chatbot
provement: towards continual monitor- tems by removing hallucinated referenc- for medicine. N Engl J Med 2023; 388:
ing and updating of AI algorithms in es to non-existent priors. October 13, 1233-9.
healthcare. NPJ Digit Med 2022;5:66. 2022 (http://arxiv.org/abs/2210.06340). pre- 98. Jeong J, Tian K, Li A, et al. Multimodal
78. Yao H, Choi C, Cao B, Lee Y, Koh PW, print. image-text matching improves retrieval-
Finn C. Wild-time: a benchmark of in-the- 88. Endo M, Krishnan R, Krishna V, Ng based chest X-ray report generation.
wild distribution shift over time. In:Pro- AY, Rajpurkar P. Retrieval-based chest March 29, 2023 (http://arxiv.org/abs/2303
ceedings and abstracts of the ICML 2022 x-ray report generation using a pre- .17579). preprint.
Shift Happens Workshop, July 22, 2022. trained contrastive language-image model. 99. Brown TB, Mann B, Ryder N, et al.
Baltimore:International Conference on PMLR 2021;158:209-19 (https://proceedings Language models are few-shot learners.
Machine Learning, 2022. .mlr.press/v158/endo21a.html). In:Proceedings and abstracts of the 2020
79. Soin A, Merkow J, Long J, et al. 89. Bannur S, Hyland S, Liu Q, et al. Conference on Neural Information Pro-
CheXstray: real-time multi-modal data Learning to exploit temporal structure cessing Systems, December 6–12, 2020.
concordance for drift detection in medi- for biomedical vision-language process- Virtual:Neural Information Processing
cal imaging AI. March 17, 2022 (http:// ing. March 16, 2023 (http://arxiv.org/abs/ Systems Foundation, 2020.
arxiv.org/abs/2202.02833). preprint. 2301.04558). preprint. Copyright © 2023 Massachusetts Medical Society.
1990 n engl j med 388;21 nejm.org May 25, 2023
The New England Journal of Medicine
Downloaded from nejm.org by Adrian H. Aguilera on August 24, 2023. For personal use only. No other uses without permission.
Copyright © 2023 Massachusetts Medical Society. All rights reserved.
You might also like
- JPNR - 2022 - S08 - 17Document8 pagesJPNR - 2022 - S08 - 17gta game playNo ratings yet
- Bjro 20190037Document8 pagesBjro 20190037GPTV AdmissionsNo ratings yet
- Artificial Intelligence and Machine Learning For Medical ImagingDocument15 pagesArtificial Intelligence and Machine Learning For Medical ImagingHeriberto AguirreNo ratings yet
- AI en Medicina-NEJM 2023Document2 pagesAI en Medicina-NEJM 2023Walter ReyesNo ratings yet
- documentDocument3 pagesdocumentsankalan.sarkarNo ratings yet
- Research PaperDocument7 pagesResearch Papersanveerkatriyar46No ratings yet
- Deep Learning Applications in Medical Image AnalysDocument16 pagesDeep Learning Applications in Medical Image AnalysPurav PillaiNo ratings yet
- Integrating AI and human intelligence for biomedical innovationDocument18 pagesIntegrating AI and human intelligence for biomedical innovationmaitrayee karNo ratings yet
- 12 II February 2024Document7 pages12 II February 2024Swapna PujariNo ratings yet
- MET REV1 DOC st13Document9 pagesMET REV1 DOC st13Karnam SirishaNo ratings yet
- Arti Ficial Intelligence in MedicineDocument8 pagesArti Ficial Intelligence in MedicineSAMUEL ESCARESNo ratings yet
- Savadjiev2018 Article DemystificationOfAI-drivenMediDocument9 pagesSavadjiev2018 Article DemystificationOfAI-drivenMediAnna LeeNo ratings yet
- Articulo 2Document4 pagesArticulo 2JULISSA MARIN VASQUEZNo ratings yet
- AI in Medical Field ApplicationsDocument8 pagesAI in Medical Field ApplicationsShree krishana ShresthaNo ratings yet
- Nejme 2206291 T 999 T 99 T 9Document2 pagesNejme 2206291 T 999 T 99 T 9Adrian Dacosta LazeraNo ratings yet
- Applications of Deep Learning in Healthcare: Sai MannamDocument3 pagesApplications of Deep Learning in Healthcare: Sai MannambashairNo ratings yet
- Med TechniqueDocument15 pagesMed TechniqueBHARGAVI DEVADIGANo ratings yet
- Applications of Machine Learning To Diagnosis and Treatment of Neurodegenerative DiseasesDocument17 pagesApplications of Machine Learning To Diagnosis and Treatment of Neurodegenerative DiseasesgcinarNo ratings yet
- AI and machine learning in medical imaging: Powerful computing required for potentialDocument3 pagesAI and machine learning in medical imaging: Powerful computing required for potentialsebampitako duncanNo ratings yet
- Artificial Intelegence in Biomedical EngineeringDocument34 pagesArtificial Intelegence in Biomedical EngineeringAsmaa Mohamed HassanNo ratings yet
- Assign 03Document14 pagesAssign 03Aleeza AnjumNo ratings yet
- A Novel Approach Towards Healthcare Using Identity Access Management and Machine LearningDocument23 pagesA Novel Approach Towards Healthcare Using Identity Access Management and Machine LearningIJRASETPublicationsNo ratings yet
- Jurinter 1Document12 pagesJurinter 1alvin 08No ratings yet
- Articulo Revista Artificial Intelligence in MedicineDocument8 pagesArticulo Revista Artificial Intelligence in MedicineAngelly TolozaNo ratings yet
- Artificial Intelligence in Radiology: From Image Processing To DiagnosisDocument4 pagesArtificial Intelligence in Radiology: From Image Processing To Diagnosispooja_44257392No ratings yet
- The Potential For Artificial Intelligence in Healthcare PDFDocument5 pagesThe Potential For Artificial Intelligence in Healthcare PDFCleberson MouraNo ratings yet
- Advancements in AI For Brain Tumor Detection and ClassificationDocument12 pagesAdvancements in AI For Brain Tumor Detection and ClassificationIJRASETPublicationsNo ratings yet
- Research PaperDocument9 pagesResearch PaperXB44.SouraTanay RoyNo ratings yet
- AI Practical 1Document3 pagesAI Practical 1prup06No ratings yet
- 1-s2.0-S0020025524001257-mainDocument17 pages1-s2.0-S0020025524001257-mainAbdullah AbdullahNo ratings yet
- College of Computer and Information Sciences: Polytechnic University of The UniversityDocument15 pagesCollege of Computer and Information Sciences: Polytechnic University of The UniversityRrjer Jahj Rollon CuevasNo ratings yet
- Fourcade 2019Document10 pagesFourcade 2019morganNo ratings yet
- The Role of Artificial Intelligence in Revolutionizing Healthcare A Comprehensive ReviewDocument11 pagesThe Role of Artificial Intelligence in Revolutionizing Healthcare A Comprehensive ReviewEditor IJTSRDNo ratings yet
- NEJM 2023. Where Medical Statistics Meets Artificial IntelligenceDocument9 pagesNEJM 2023. Where Medical Statistics Meets Artificial IntelligenceunidadmedicamazamitlaNo ratings yet
- Report - Artificial Intelligence Applications in MedicineDocument12 pagesReport - Artificial Intelligence Applications in Medicinekababey111No ratings yet
- Healthcare 11 00207 v2Document20 pagesHealthcare 11 00207 v2Uliyana KechikNo ratings yet
- Physica Medica: Review PaperDocument16 pagesPhysica Medica: Review PaperHenry Jose Izquierdo VillegasNo ratings yet
- Biomedical Texture Analysis: Fundamentals, Tools and ChallengesFrom EverandBiomedical Texture Analysis: Fundamentals, Tools and ChallengesAdrien DepeursingeNo ratings yet
- Jean - Paredes@udea - Edu.co Kevin - Caicedo@udea - Edu.co Luis - Mejia5@udea - Edu.coDocument4 pagesJean - Paredes@udea - Edu.co Kevin - Caicedo@udea - Edu.co Luis - Mejia5@udea - Edu.coJean CarlosNo ratings yet
- Depp Learning For Medical Image ProcessingDocument57 pagesDepp Learning For Medical Image Processingderricktab44No ratings yet
- NTTTTTDocument5 pagesNTTTTTDippal IsraniNo ratings yet
- 2020 Artificial Intelligence For Brain Diseases A Systematic ReviewDocument36 pages2020 Artificial Intelligence For Brain Diseases A Systematic ReviewMarcilio MeiraNo ratings yet
- 16 - Artificial Intelligence and Machine Learning in Pathology The Present Landscape of Supervised MethodsDocument17 pages16 - Artificial Intelligence and Machine Learning in Pathology The Present Landscape of Supervised MethodsOffice WorkNo ratings yet
- Theoretical Review On Artificial Intelligence Used in The Medical SectorDocument6 pagesTheoretical Review On Artificial Intelligence Used in The Medical SectorInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 2018 - Edoctor Machine Learning and The Future of Medicine - Handelman Et Al.Document17 pages2018 - Edoctor Machine Learning and The Future of Medicine - Handelman Et Al.A CNo ratings yet
- Review Paper On Artificial Intelligence in Medical & HealthcareDocument3 pagesReview Paper On Artificial Intelligence in Medical & HealthcareInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- AI in Different FormsDocument2 pagesAI in Different FormsMyla TolentinoNo ratings yet
- Futurehealth 9 1 75Document4 pagesFuturehealth 9 1 75christopher.lovejoy1No ratings yet
- AI Case Study FormatDocument8 pagesAI Case Study FormatSaumen DasNo ratings yet
- A Systematic Review On Artificial Intelligence ForDocument20 pagesA Systematic Review On Artificial Intelligence ForblueyoonvNo ratings yet
- Poster Presentation Template Horizontal 2Document1 pagePoster Presentation Template Horizontal 2Rahaf FaizNo ratings yet
- Emerging Applications of Artificial Intelligence in Neuro-OncologyDocument12 pagesEmerging Applications of Artificial Intelligence in Neuro-OncologyJeff RudieNo ratings yet
- Entendiendo Artifiestudios de Radiología Basados en Inteligencia Cial Qué EsencimafittingDocument4 pagesEntendiendo Artifiestudios de Radiología Basados en Inteligencia Cial Qué Esencimafittingsanya eusebia lupaca lupacaNo ratings yet
- Applications of Artificial Intelligence in HealthcareJournal of Experimental Biology and Agricultural SciencesDocument16 pagesApplications of Artificial Intelligence in HealthcareJournal of Experimental Biology and Agricultural SciencesAditya ShuklaNo ratings yet
- Data-Driven Healthcare: Revolutionizing Patient Care with Data ScienceFrom EverandData-Driven Healthcare: Revolutionizing Patient Care with Data ScienceNo ratings yet
- The Role of Generative Adversarial Networks in Brain MRI: A Scoping ReviewDocument15 pagesThe Role of Generative Adversarial Networks in Brain MRI: A Scoping ReviewAKASH KUMAR SINGH 201460No ratings yet
- 1 s2.0 S1507136720300444 MainDocument11 pages1 s2.0 S1507136720300444 MainAhmad RefaatNo ratings yet
- Artificial Intelligence - INFORMSDocument5 pagesArtificial Intelligence - INFORMSMiguel GarcíaNo ratings yet
- Survey of Explainable Artificial Intelligence Techniques For Biomedical Imaging With Deep Neural NetworksDocument29 pagesSurvey of Explainable Artificial Intelligence Techniques For Biomedical Imaging With Deep Neural Networkslenka14126No ratings yet
- From Blackbox To Explainable AI in Healthcare: Existing Tools and Case StudiesDocument20 pagesFrom Blackbox To Explainable AI in Healthcare: Existing Tools and Case StudiesStephanie Jane DacerNo ratings yet
- geospatial AIDocument9 pagesgeospatial AIAdrian H. AguileraNo ratings yet
- DM_AI_voice_predictionDocument11 pagesDM_AI_voice_predictionAdrian H. AguileraNo ratings yet
- 1 s2.0 S0965997822002381 MainDocument5 pages1 s2.0 S0965997822002381 Maindodol garutNo ratings yet
- AI US Delivery NEJMDocument11 pagesAI US Delivery NEJMAdrian H. AguileraNo ratings yet
- CLM PresentationDocument13 pagesCLM PresentationHSC UNITEDNo ratings yet
- Interconnection Between Moles On Face and Urine LeukocytesDocument3 pagesInterconnection Between Moles On Face and Urine LeukocytesMiddle East Journal of Applied Science & TechnologyNo ratings yet
- Acute Gastroenteritis (Age)Document37 pagesAcute Gastroenteritis (Age)Jay Ar SantiagoNo ratings yet
- Dance TherapyDocument2 pagesDance TherapyXimena OrdonezNo ratings yet
- Gestational Hypertension and Preeclampsia Causes of Maternal DeathDocument2 pagesGestational Hypertension and Preeclampsia Causes of Maternal DeathPrayoga SiraitNo ratings yet
- Top Knife PDFDocument238 pagesTop Knife PDFKristin Smith100% (2)
- PART X CNS StimulantsDocument10 pagesPART X CNS StimulantsmichaelcylNo ratings yet
- Mills 1975Document6 pagesMills 1975Nida AtmimNo ratings yet
- Dermoscopy of Inflamed Seborrheic KeratosisDocument9 pagesDermoscopy of Inflamed Seborrheic KeratosisFreddy RojasNo ratings yet
- DR - Hur Krok Pediatrics 2014 PDFDocument89 pagesDR - Hur Krok Pediatrics 2014 PDFAnasse Douma100% (1)
- Form 4A notifies TB diagnosis and treatmentDocument1 pageForm 4A notifies TB diagnosis and treatmentKim PeroNo ratings yet
- Intro To Rad MidtermDocument27 pagesIntro To Rad Midtermedenribalde3No ratings yet
- GP41A6 SampleDocument13 pagesGP41A6 SampleAndy BogardNo ratings yet
- Diagnostic Criteria For 298Document1 pageDiagnostic Criteria For 298Pradeep KumarNo ratings yet
- Pancreatite AgudaDocument8 pagesPancreatite AgudaGabriel MouraNo ratings yet
- Case PresentationDocument25 pagesCase PresentationGaurav TanwarNo ratings yet
- Cambridge English For Nursing Authentic Medical Forms and ChartsDocument11 pagesCambridge English For Nursing Authentic Medical Forms and ChartsAngela MercadoNo ratings yet
- Orthopedic AssessmentDocument4 pagesOrthopedic Assessmentkrissh20No ratings yet
- The Hall Technique 10 Years On: Questions and Answers: GeneralDocument6 pagesThe Hall Technique 10 Years On: Questions and Answers: GeneralamilescoNo ratings yet
- Globocan 2020Document2 pagesGlobocan 2020Dicky keyNo ratings yet
- Askep Emboli Paru - Edema Paru - Cor PulmonalDocument63 pagesAskep Emboli Paru - Edema Paru - Cor PulmonalDhevy Sa'PhuttRyyNo ratings yet
- Ingelvac Provenza: Description: Directions and DosageDocument2 pagesIngelvac Provenza: Description: Directions and DosageDrivailaNo ratings yet
- Ch2012.Decompressive Craniectomy - Operative TechniqueDocument22 pagesCh2012.Decompressive Craniectomy - Operative TechniqueKysy CodonNo ratings yet
- Or DR Nclex FormsDocument6 pagesOr DR Nclex FormsClarence MangíoNo ratings yet
- How to Write a SOAP NoteDocument13 pagesHow to Write a SOAP NotePhuong TranNo ratings yet
- MOCKBOARD Exam I QUISTION ONLYDocument14 pagesMOCKBOARD Exam I QUISTION ONLYRegine EncinadaNo ratings yet
- 15 - CCLS - PharmacologyDocument32 pages15 - CCLS - PharmacologyVENKATESH RAMSALINo ratings yet
- Effectiveness of TMS in Treatment Resistant Depression - EditedDocument13 pagesEffectiveness of TMS in Treatment Resistant Depression - EditedBandah Mwiti JosephNo ratings yet
- Dual Diagnostic PresentationDocument8 pagesDual Diagnostic PresentationMark H. StevensNo ratings yet
- Referensi No 7Document5 pagesReferensi No 7Bagus Wanda HabibullahNo ratings yet