You might also like
- Síndrome Hepatorrenal Cirrosis Eur Gast J 2021Document9 pagesSíndrome Hepatorrenal Cirrosis Eur Gast J 2021Anabel GonzalezNo ratings yet
- Kidney Injury: AcuteDocument14 pagesKidney Injury: AcutealfredoibcNo ratings yet
- Essential Update: FDA Approves First Test To Predict AKI in Critically Ill PatientsDocument5 pagesEssential Update: FDA Approves First Test To Predict AKI in Critically Ill PatientsRika Ariyanti SaputriNo ratings yet
- 1866-Jepson - ACUTE KIDNEY INJURY EARLY IDENTIFICATION FOR PROMPT MANAGEMENTDocument3 pages1866-Jepson - ACUTE KIDNEY INJURY EARLY IDENTIFICATION FOR PROMPT MANAGEMENTYaiza Garcia CasadoNo ratings yet
- Acute Kidney FailureDocument8 pagesAcute Kidney Failureanimesh pandaNo ratings yet
- AKI Case Discussion 2.0Document3 pagesAKI Case Discussion 2.0Mary Dominique RomoNo ratings yet
- Acute Kidney InjuryDocument17 pagesAcute Kidney InjuryCha-cha UzumakiNo ratings yet
- Acute Kidney InjuryDocument2 pagesAcute Kidney InjuryMariel GamaloNo ratings yet
- Gagal Ginjal Akut - Bhs InggrisDocument27 pagesGagal Ginjal Akut - Bhs InggrisAgustinusNo ratings yet
- Diagnostic Criteria For Acute Kidney Injury: Present and FutureDocument12 pagesDiagnostic Criteria For Acute Kidney Injury: Present and FutureTony Gomez Luna LeyvaNo ratings yet
- ACUTE RENAL FAILURE DIAGNOSIS & MANAGEMENTDocument2 pagesACUTE RENAL FAILURE DIAGNOSIS & MANAGEMENTSetiya Dini LarasatiNo ratings yet
- Coursematerial 136Document13 pagesCoursematerial 136Nyj QuiñoNo ratings yet
- Acute Kidney Injury An UpdateDocument9 pagesAcute Kidney Injury An Updatekarol fernandezNo ratings yet
- Chronic Kidney Disease in Small Animals1Document16 pagesChronic Kidney Disease in Small Animals1ZiedTrikiNo ratings yet
- Acute Kidney Injury: Current Concepts and New Insights: Key WordsDocument5 pagesAcute Kidney Injury: Current Concepts and New Insights: Key WordsIHNo ratings yet
- Jurnal CKDDocument7 pagesJurnal CKDJuni ClaudiaNo ratings yet
- Canine Chronic Kidney Disease Current Diagnostics & Goals For Long-Term ManagementDocument7 pagesCanine Chronic Kidney Disease Current Diagnostics & Goals For Long-Term ManagementJuni ClaudiaNo ratings yet
- Acute Kidney Injury. Pediatrics in Review-2014-Selewski-30-41Document14 pagesAcute Kidney Injury. Pediatrics in Review-2014-Selewski-30-41Mc WarsameNo ratings yet
- Chronic Kidney Disease in Dogs and Cats: Joseph W. BartgesDocument24 pagesChronic Kidney Disease in Dogs and Cats: Joseph W. BartgesDany CamposNo ratings yet
- Acute Kidney InjuryDocument15 pagesAcute Kidney Injurykuchaibaru90No ratings yet
- Acute Renal Failure in The ICU PulmCritDocument27 pagesAcute Renal Failure in The ICU PulmCritchadchimaNo ratings yet
- Acute Kidney Injury Causes and TypesDocument9 pagesAcute Kidney Injury Causes and TypesKacey MandNo ratings yet
- Lecture 2. Acute Renal FailureDocument85 pagesLecture 2. Acute Renal FailurePharmswipe KenyaNo ratings yet
- Acute Kidney Injury: On Completion of This Chapter, The Learner Will Be Able ToDocument9 pagesAcute Kidney Injury: On Completion of This Chapter, The Learner Will Be Able TojhcacbszkjcnNo ratings yet
- Aetiology: Save Time & Improve Your PDP On Patient - Co.ukDocument9 pagesAetiology: Save Time & Improve Your PDP On Patient - Co.ukBaihaqi SaharunNo ratings yet
- Renal Disease: Acute Kidney Injury (AKI)Document5 pagesRenal Disease: Acute Kidney Injury (AKI)api-142637023No ratings yet
- CKDDDocument11 pagesCKDDAnaNo ratings yet
- Joacp 28 386Document11 pagesJoacp 28 386KrisztinaNo ratings yet
- Renal Failure: An OverviewDocument28 pagesRenal Failure: An OverviewaburisyaNo ratings yet
- Acute Renal FailureDocument12 pagesAcute Renal FailureRifa Aprillia CahyaniNo ratings yet
- Recognition and Management of Acute Kidney Injury: Thomas Oates and Shabbir MoochhalaDocument5 pagesRecognition and Management of Acute Kidney Injury: Thomas Oates and Shabbir MoochhalaIntan NoaNo ratings yet
- Diagnostic Approach To The Patient With Newly Identified Chronic Kidney DiseaseDocument1 pageDiagnostic Approach To The Patient With Newly Identified Chronic Kidney DiseaseLauraNo ratings yet
- Subclinical Celiac Disease and Crystal-Induced Kidney Disease Following Kidney TransplantDocument6 pagesSubclinical Celiac Disease and Crystal-Induced Kidney Disease Following Kidney TransplantsigmundmaharajanNo ratings yet
- Inter'Medic CKDDocument31 pagesInter'Medic CKDMAHEJS HD100% (1)
- 2016 AJKD Volume 67 Issue 2 February (33) HepatorenalDocument11 pages2016 AJKD Volume 67 Issue 2 February (33) HepatorenalAnonymous Yo0mStNo ratings yet
- Global Epidemiology and Outcomes of Acute Kidney InjuryDocument19 pagesGlobal Epidemiology and Outcomes of Acute Kidney Injuryredouane bennaiNo ratings yet
- Chronic Kidney DiseaseDocument55 pagesChronic Kidney DiseaseBentoys Street100% (1)
- Acute InjuryDocument1 pageAcute InjuryJesell France PlanaNo ratings yet
- Causes of Acute Deterioration in Chronic Kidney DiseaseDocument3 pagesCauses of Acute Deterioration in Chronic Kidney DiseaseSitLus ChannelNo ratings yet
- Feline Kidney Disease at a GlanceDocument2 pagesFeline Kidney Disease at a GlanceShar ThornNo ratings yet
- Injuria Renală Acută CorectatDocument6 pagesInjuria Renală Acută CorectatCaraiman LarisaNo ratings yet
- Renal Hypouricemia with Exercise Induced Acute Kidney Injury-A Case Report - PMCDocument6 pagesRenal Hypouricemia with Exercise Induced Acute Kidney Injury-A Case Report - PMCYogesh GaurNo ratings yet
- Pharmacotherapy of Renal DisordersDocument231 pagesPharmacotherapy of Renal DisordersTewodros GetahunNo ratings yet
- SX Hepatorrenal 2020Document14 pagesSX Hepatorrenal 2020AlexisBallénNo ratings yet
- Diagnosis and Management of Acute Kidney Injury, Acute on CKD and CKD Stage 5Document39 pagesDiagnosis and Management of Acute Kidney Injury, Acute on CKD and CKD Stage 5Ely Kartika100% (1)
- Acute Kidney Injury-PROBINMABA ENGDocument2 pagesAcute Kidney Injury-PROBINMABA ENGnuke primaestiNo ratings yet
- HTTPDocument10 pagesHTTPkasmiatiNo ratings yet
- Hepatorenal SyndromeDocument14 pagesHepatorenal SyndromeVerónica Duménez JofréNo ratings yet
- Acute Kidney Injury LANCETDocument11 pagesAcute Kidney Injury LANCETJessica AdvínculaNo ratings yet
- Acute Kidney Injury and Chronic Kidney DiseaseDocument44 pagesAcute Kidney Injury and Chronic Kidney DiseaseshihochanNo ratings yet
- AKI Perioperatif 3Document6 pagesAKI Perioperatif 3Kevin JohanesNo ratings yet
- Renal EmergenciesDocument93 pagesRenal EmergenciesShubham gaurNo ratings yet
- Renal Failure: Prepare by Mohammed Sahman Basees Alsharari - 391110030Document31 pagesRenal Failure: Prepare by Mohammed Sahman Basees Alsharari - 391110030jsksNo ratings yet
- Acute Chronic Renal FailureDocument43 pagesAcute Chronic Renal FailureHigh Education100% (1)
- Fluid and Electrolyte Problems in Renal DysfunctionDocument5 pagesFluid and Electrolyte Problems in Renal Dysfunctionfachrudin arNo ratings yet
- Low-Flow Acute Kidney InjuryDocument11 pagesLow-Flow Acute Kidney InjuryJuan Manuel Lopez VargasNo ratings yet
- Renal Biopsy of Dogs and CatsDocument12 pagesRenal Biopsy of Dogs and CatsfrankyNo ratings yet
- Restoring Chronic Kidney Disease : Restoring, Preserving, and Improving CKD to Avoid DialysisFrom EverandRestoring Chronic Kidney Disease : Restoring, Preserving, and Improving CKD to Avoid DialysisNo ratings yet
- Polycystic Kidneys, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandPolycystic Kidneys, A Simple Guide To The Condition, Treatment And Related DiseasesNo ratings yet
- DCO VS ETCDocument34 pagesDCO VS ETCSebastian MihardjaNo ratings yet
- BurnDocument13 pagesBurniheanachomeviaNo ratings yet
- And Protection of Renal Function in The Intensive Care Unit - Update 2017Document20 pagesAnd Protection of Renal Function in The Intensive Care Unit - Update 2017Edson MarquesNo ratings yet
- Intravenous Fluid Therapy For Adults in Hospital Clinical GuidelineDocument10 pagesIntravenous Fluid Therapy For Adults in Hospital Clinical GuidelinePremaKurniaNo ratings yet
- Nor (2018) Ischaemic Haemorrhagic Stroke in A ChildDocument3 pagesNor (2018) Ischaemic Haemorrhagic Stroke in A ChildFelicia HarsonoNo ratings yet
- Kabilyte FinalDocument42 pagesKabilyte Finaldrchelluri100% (1)
- Oral rehydration therapy for diarrheaDocument16 pagesOral rehydration therapy for diarrheaNedelcu MirunaNo ratings yet
- Eba Guidelines Burn Care Version 1Document49 pagesEba Guidelines Burn Care Version 1mrizkidm2301No ratings yet
- I.V. Fluid Therapy IDocument4 pagesI.V. Fluid Therapy IPrabath ChinthakaNo ratings yet
- TNSOP 6 Clinical GuidelinesDocument14 pagesTNSOP 6 Clinical Guidelinesazar103No ratings yet
- Evidenced-Based Nursing I. Clinical QuestionDocument3 pagesEvidenced-Based Nursing I. Clinical QuestionLemuel Glenn BautistaNo ratings yet
- Burns An Introduction To Burns and Basic Wound - 2023 - Physician Assistant CliDocument11 pagesBurns An Introduction To Burns and Basic Wound - 2023 - Physician Assistant CliJose AnaconaNo ratings yet
- CH 14 Test BankDocument21 pagesCH 14 Test BankKrestine MolleNo ratings yet
- IV Fluid Therapy in Adults: National Clinical Guideline CentreDocument270 pagesIV Fluid Therapy in Adults: National Clinical Guideline CentreYanti YantiNo ratings yet
- Pediatric BurnsDocument9 pagesPediatric BurnsManoj KumarNo ratings yet
- Burns ActvityDocument5 pagesBurns ActvityJoshua TercenoNo ratings yet
- Medication AdministrationDocument34 pagesMedication AdministrationSarie Levita100% (2)
- Comparison of Clinical Outcomes Between Aggressive and Non AggressiveDocument11 pagesComparison of Clinical Outcomes Between Aggressive and Non Aggressivecheve glzNo ratings yet
- Introduction To Critical Care Nursing 6th Edition Sole Test BankDocument38 pagesIntroduction To Critical Care Nursing 6th Edition Sole Test Bankgabrielnt3me100% (15)
- COMPILATION OF SAUNDERS 4 Ed., LIPPINCOTT 8th Ed. & MOSBYDocument260 pagesCOMPILATION OF SAUNDERS 4 Ed., LIPPINCOTT 8th Ed. & MOSBYRaffy75% (12)
- General Surgery: Aiims MedeasyDocument19 pagesGeneral Surgery: Aiims Medeasyvk100% (2)
- Burn Lecture NotesDocument5 pagesBurn Lecture NotesJerlyn Lopez100% (1)
- 3.2 Guiding Principle For Subcutaneous TherapyDocument8 pages3.2 Guiding Principle For Subcutaneous TherapyAda EzeNo ratings yet
- Fluid Management in The Critically Ill: Jean-Louis VincentDocument6 pagesFluid Management in The Critically Ill: Jean-Louis VincentFlorentina NadisaNo ratings yet
- Mihi Catalog 01 2022 enDocument33 pagesMihi Catalog 01 2022 enmaci74No ratings yet
- Initial Assessment of A Major Burn: Table 1Document29 pagesInitial Assessment of A Major Burn: Table 1Nylia AtibiNo ratings yet
- Fluids and ElectrolytesDocument48 pagesFluids and ElectrolytesDoha EbedNo ratings yet
- Intravenous Fluid Therapy - Knowledge For Medical Students and PhysiciansDocument6 pagesIntravenous Fluid Therapy - Knowledge For Medical Students and PhysiciansNafiul IslamNo ratings yet
- Oral Ondansetron For Paediatric Gastroenteritis in Primary Care A Randomised Controlled TrialDocument8 pagesOral Ondansetron For Paediatric Gastroenteritis in Primary Care A Randomised Controlled TrialAssyifa LunaNo ratings yet
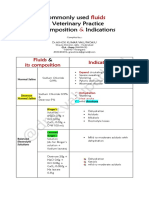
- Common IV Fluids at Composition & IndicationsDocument2 pagesCommon IV Fluids at Composition & IndicationsNilesh SuryawanshiNo ratings yet