You might also like
- Pediatric Restorative DentistryFrom EverandPediatric Restorative DentistrySoraya Coelho LealNo ratings yet
- Dental workforce attitudes on hygienist employment and scopeDocument7 pagesDental workforce attitudes on hygienist employment and scopetea metaNo ratings yet
- Attitudes To and Knowledge About Oral Health Care Among Nursing Home Personnel - An Area in Need of ImprovementDocument6 pagesAttitudes To and Knowledge About Oral Health Care Among Nursing Home Personnel - An Area in Need of ImprovementSaravanan ThangarajanNo ratings yet
- Working Practices and Job Satisfaction of Victorian Dental HygienistsDocument6 pagesWorking Practices and Job Satisfaction of Victorian Dental Hygieniststea metaNo ratings yet
- Specialist and Transitional Care Provision For Amelogenesis Imperfecta - A UK-wide SurveyDocument5 pagesSpecialist and Transitional Care Provision For Amelogenesis Imperfecta - A UK-wide SurveyMohammad Abdulmon’emNo ratings yet
- 1.1 Original ResearchDocument8 pages1.1 Original ResearchNovita RNo ratings yet
- 10 33631-Sabd 1055376-2182384Document10 pages10 33631-Sabd 1055376-2182384rose1999.rjNo ratings yet
- s41415 021 3130 9 PDFDocument12 pagess41415 021 3130 9 PDFrasiNo ratings yet
- Complete Article Apc Jisppd-1Document17 pagesComplete Article Apc Jisppd-1Nishant MehtaNo ratings yet
- Safeguarding Children in Dentistry: 2. Do Paediatric Dentists Neglect Child Dental Neglect?Document6 pagesSafeguarding Children in Dentistry: 2. Do Paediatric Dentists Neglect Child Dental Neglect?bkprosthoNo ratings yet
- Promoting Oral Health in Older PeopleDocument2 pagesPromoting Oral Health in Older PeopleatikramadhaniNo ratings yet
- Attitude ArticleDocument9 pagesAttitude Articlemeena syedNo ratings yet
- Title: Children's Oral Health Strategy in The UKDocument8 pagesTitle: Children's Oral Health Strategy in The UKshahryar eskandarzadeNo ratings yet
- Oral Health PromotionDocument29 pagesOral Health PromotionRob21aNo ratings yet
- Effective Interventions To Prevent Dental Caries in Preschool ChildrenDocument56 pagesEffective Interventions To Prevent Dental Caries in Preschool ChildrenDiego AzaedoNo ratings yet
- Trends in Paediatric First Dental Visit A RetrospeDocument6 pagesTrends in Paediatric First Dental Visit A RetrospeData VaksinNo ratings yet
- Version of Record Doi: 10.1111/IPD.12599Document10 pagesVersion of Record Doi: 10.1111/IPD.12599AndreBarrancoNo ratings yet
- 03 Knowledge Attitudes and Behavior Towards Oral Health Among A Group of Staff Caring For Elderly People in Long Term Care Facilities in Bangkok ThailandDocument16 pages03 Knowledge Attitudes and Behavior Towards Oral Health Among A Group of Staff Caring For Elderly People in Long Term Care Facilities in Bangkok ThailandFadli AlwiNo ratings yet
- 98c458e29834139d9bd40f4a84411bc2Document9 pages98c458e29834139d9bd40f4a84411bc2andres.ft12345No ratings yet
- Foreign LiteratureDocument13 pagesForeign LiteratureJm. n BelNo ratings yet
- 2 Master Article 2Document5 pages2 Master Article 2neetika guptaNo ratings yet
- AAPD Policy on Workforce Issues and Delivery of Oral Health Care Services in a Dental HomeDocument5 pagesAAPD Policy on Workforce Issues and Delivery of Oral Health Care Services in a Dental HomefaizahNo ratings yet
- Ejpd 2018 19 3 3Document6 pagesEjpd 2018 19 3 3Javier Cabanillas ArteagaNo ratings yet
- Review On Infant Oral HealthDocument11 pagesReview On Infant Oral HealthIJAR JOURNALNo ratings yet
- Direct Pulp Capping in Priamry Teeth A Systematic ReviewDocument11 pagesDirect Pulp Capping in Priamry Teeth A Systematic ReviewDaniel Pierre DyotteNo ratings yet
- Public Health Dentistry Thesis TopicsDocument5 pagesPublic Health Dentistry Thesis Topicss0kuzej0byn2100% (2)
- Oral Health in Institutionalised Elderly People in Oslo, Norway and Its Relationship With Dependence and Cognitive ImpairmentDocument8 pagesOral Health in Institutionalised Elderly People in Oslo, Norway and Its Relationship With Dependence and Cognitive ImpairmentTria Sesar AprianiNo ratings yet
- Erosion Guidelines - 2021 - V4 - MJDocument32 pagesErosion Guidelines - 2021 - V4 - MJAARON DIAZ RONQUILLONo ratings yet
- CBOHMaindocument JUNE2014Document66 pagesCBOHMaindocument JUNE2014fashuanmi ibukunNo ratings yet
- Impact of Regular Professional Toothbrushing On Oral Health, Related Quality of Life, and Nutritional and Cognitive Status in Nursing Home ResidentsDocument13 pagesImpact of Regular Professional Toothbrushing On Oral Health, Related Quality of Life, and Nutritional and Cognitive Status in Nursing Home ResidentsMarco Antonio García LunaNo ratings yet
- Using Oral Hygiene Education in Schools To Tackle Child Tooth Decay A Mixed Methods Study With Children and Teachers in EnglandDocument16 pagesUsing Oral Hygiene Education in Schools To Tackle Child Tooth Decay A Mixed Methods Study With Children and Teachers in EnglandDiandra Sariarum DjajakusumahNo ratings yet
- Development of A Model of Care For Dental and Mouth Health in Toddlers With The Game "Ma'Boy" As An Alternative Change in Mother's Behavior and Formation of Children's Teeth-Brushing SkillsDocument9 pagesDevelopment of A Model of Care For Dental and Mouth Health in Toddlers With The Game "Ma'Boy" As An Alternative Change in Mother's Behavior and Formation of Children's Teeth-Brushing SkillsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Hill Adult Dental Health SurveyDocument8 pagesHill Adult Dental Health Surveydesy purnama sariNo ratings yet
- Oral Health Promotion and Intervention Activities Carried Out in Rural Areas of Davangere DistrictDocument49 pagesOral Health Promotion and Intervention Activities Carried Out in Rural Areas of Davangere DistrictShabby PoetNo ratings yet
- NHS England Paediatric DentistryDocument15 pagesNHS England Paediatric DentistryDina ElkharadlyNo ratings yet
- Oral Health ProgramDocument8 pagesOral Health Programapi-292263050No ratings yet
- The Shortened Dental Arch Concept Awareness and Opinion of Dentists in Australia PDFDocument8 pagesThe Shortened Dental Arch Concept Awareness and Opinion of Dentists in Australia PDFKarina OjedaNo ratings yet
- Community Project 1Document10 pagesCommunity Project 1Scott Michael SonnierNo ratings yet
- Assessment of Knowledge Attitude and Perception of Dental Students Towards Obesity in Kanpur CityDocument6 pagesAssessment of Knowledge Attitude and Perception of Dental Students Towards Obesity in Kanpur CityAdvanced Research PublicationsNo ratings yet
- Keywords:-Data Collection and Evaluation, UKGSDocument11 pagesKeywords:-Data Collection and Evaluation, UKGSInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Oral Health Education Improved Oral Health KnowledgeDocument11 pagesOral Health Education Improved Oral Health KnowledgeGita PratamaNo ratings yet
- Adj 12749Document10 pagesAdj 12749Irfan HussainNo ratings yet
- Application of Machine Learning For Diagnostic Prediction of Root CariesDocument10 pagesApplication of Machine Learning For Diagnostic Prediction of Root CariesHarisankar BNo ratings yet
- International Association of Dental Traumatology Guidelines For The Management of Traumatic Dental Injuries: 3. Injuries in The Primary DentitionDocument44 pagesInternational Association of Dental Traumatology Guidelines For The Management of Traumatic Dental Injuries: 3. Injuries in The Primary DentitionaNo ratings yet
- Index for Interceptive ReferralDocument22 pagesIndex for Interceptive Referral강북다인치과No ratings yet
- Longetivity of DentureDocument9 pagesLongetivity of DentureShyam DangarNo ratings yet
- Thesis Topics Public Health DentistryDocument5 pagesThesis Topics Public Health DentistryKristen Flores100% (2)
- Oral Health Coalition: Knowledge, Attitude, Practice Behaviours Among Gynaecologists and Dental PractitionersDocument8 pagesOral Health Coalition: Knowledge, Attitude, Practice Behaviours Among Gynaecologists and Dental PractitionersIndah AmaliaNo ratings yet
- 40368_2022_Article_721Document8 pages40368_2022_Article_721cosadedubsNo ratings yet
- Attitudes and Lifestyle Factors in Relation To Oral Health and Dental Care in Sweden A Cross Sectional StudyDocument9 pagesAttitudes and Lifestyle Factors in Relation To Oral Health and Dental Care in Sweden A Cross Sectional Studyasem sardyNo ratings yet
- Healthcare 10 00406Document12 pagesHealthcare 10 00406AamirNo ratings yet
- Desai 2001Document11 pagesDesai 2001Layal J. AlQahtaniNo ratings yet
- Analysis of Oral Hygiene Education in Obese Children in Local Population of PakistanDocument5 pagesAnalysis of Oral Hygiene Education in Obese Children in Local Population of PakistaniajpsNo ratings yet
- Jurnal Kedokteran Gigi TerindeksDocument5 pagesJurnal Kedokteran Gigi TerindeksALFEARA YUNIARNo ratings yet
- HSDC QuintesenceDocument6 pagesHSDC QuintesenceDavid CasaverdeNo ratings yet
- P DentalhomeDocument5 pagesP Dentalhomemehta15drishaNo ratings yet
- 6 - Original Article PDFDocument7 pages6 - Original Article PDFIna BogdanNo ratings yet
- Policy On Model Dental Benefits For InfantsDocument4 pagesPolicy On Model Dental Benefits For InfantsمعتزباللهNo ratings yet
- Examining The Oral Health of Filipinos: Policy Analysis: Original ArticleDocument7 pagesExamining The Oral Health of Filipinos: Policy Analysis: Original ArticleTimothy LimaNo ratings yet
- Booklet - e 1 - 2013Document101 pagesBooklet - e 1 - 2013Dani AedoNo ratings yet
- Measurement and Correlates of Family Caregiver Self-Efficacy For Managing DementiaDocument9 pagesMeasurement and Correlates of Family Caregiver Self-Efficacy For Managing DementiariskhawatiNo ratings yet
- Borderline Personality DisorderDocument7 pagesBorderline Personality DisorderleaNo ratings yet
- Chapter 1 2 3Document77 pagesChapter 1 2 3Ferissa MohammadNo ratings yet
- Should Homework Be Banned From School?Document7 pagesShould Homework Be Banned From School?Chuyên ĐỗNo ratings yet
- Intrathecal MTX & Cytarabine & Hydrocortisone V4 2.15Document2 pagesIntrathecal MTX & Cytarabine & Hydrocortisone V4 2.15GabrielNo ratings yet
- Question and AnswerDocument4 pagesQuestion and AnswerShaf AbubakarNo ratings yet
- TC Elastomeric Tapes SDS Rev 3, 2-19 - 1 PDFDocument6 pagesTC Elastomeric Tapes SDS Rev 3, 2-19 - 1 PDFEbondNo ratings yet
- Nelson Textbook of Pediatrics (2-Volume Set) by Robert M. Kliegman, Bonita F. Stanton, Joseph W. ST Geme III, Nina F. SchorDocument312 pagesNelson Textbook of Pediatrics (2-Volume Set) by Robert M. Kliegman, Bonita F. Stanton, Joseph W. ST Geme III, Nina F. SchorFaisal MomenNo ratings yet
- Tung DocumentreviewDocument8 pagesTung DocumentreviewRodrigo Bittencourt100% (3)
- Perioperative Concepts and Nursing ManagementDocument107 pagesPerioperative Concepts and Nursing ManagementHarley Justiniani Dela CruzNo ratings yet
- SIP Physical SCiDocument8 pagesSIP Physical SCiShane Catherine BesaresNo ratings yet
- Introduction of Online Basic First Aid Course - For Circulation April 2021Document39 pagesIntroduction of Online Basic First Aid Course - For Circulation April 2021Yuwaraj NaiduNo ratings yet
- Pathology of the EndocardiumDocument31 pagesPathology of the EndocardiumAlexe VladNo ratings yet
- Acute Respiratory Distress Syndrome: Jason D. Sciarretta, M.D. Critical Care Conference October 13, 2010Document24 pagesAcute Respiratory Distress Syndrome: Jason D. Sciarretta, M.D. Critical Care Conference October 13, 2010JelenaNo ratings yet
- Small-Sided Games and Integrating Physical PreparationDocument196 pagesSmall-Sided Games and Integrating Physical Preparationbolebs1475% (4)
- BCS Class of DrugsDocument45 pagesBCS Class of DrugsLionO50% (2)
- Amway ProductDocument9 pagesAmway ProductAbu Sayed Md. RashedNo ratings yet
- Mercury in The MistDocument2 pagesMercury in The MistAnand BhagwaniNo ratings yet
- AOTA Statement On Role of OT in NICUDocument9 pagesAOTA Statement On Role of OT in NICUMapi RuizNo ratings yet
- Grain Legumes/Pulses Introduction and ImportanceDocument5 pagesGrain Legumes/Pulses Introduction and ImportancesumandhakalNo ratings yet
- Health Information Technology-HISMLSDocument1 pageHealth Information Technology-HISMLSJanela Escalante TaboraNo ratings yet
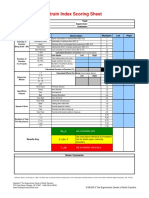
- Strain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorDocument1 pageStrain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorUdaydeep SinghNo ratings yet
- Effects of Energy Gel Ingestion On Blood Glucose, Lactate, and Performance Measures During Prolonged CyclingDocument9 pagesEffects of Energy Gel Ingestion On Blood Glucose, Lactate, and Performance Measures During Prolonged Cyclingjose david HerreraNo ratings yet
- Project ProposalDocument16 pagesProject ProposalMashaal FasihNo ratings yet
- ICICI Bank Mortgage - HS360 Product FinalDocument29 pagesICICI Bank Mortgage - HS360 Product FinalRishu GiriNo ratings yet
- Veteran Resource Guide For Congressional District 9Document27 pagesVeteran Resource Guide For Congressional District 9RepSinemaNo ratings yet
- Babu Jagjivan RamDocument24 pagesBabu Jagjivan RamAnonymous qFWInco8cNo ratings yet
- Change Your Life in 7 Days With NLP - Paul Mckenna BrochureDocument2 pagesChange Your Life in 7 Days With NLP - Paul Mckenna Brochureapi-385316675% (4)
- HRM Case StudyDocument21 pagesHRM Case StudyNabil Eyg Iakini100% (1)