Professional Documents
Culture Documents
Covid Rs Statement
Uploaded by
Mobile LegendsOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Covid Rs Statement
Uploaded by
Mobile LegendsCopyright:
Available Formats
See discussions, stats, and author profiles for this publication at: https://www.researchgate.
net/publication/372860807
Antipsychotic drug prescribing and mortality in people with dementia before
and during the COVID-19 pandemic: a retrospective cohort study in Wales, UK
Article in The Lancet Healthy Longevity · August 2023
DOI: 10.1016/S2666-7568(23)00105-8
CITATION READS
1 179
13 authors, including:
Christian Schnier Daniel R Morales
The University of Edinburgh University of Dundee
100 PUBLICATIONS 911 CITATIONS 168 PUBLICATIONS 3,032 CITATIONS
SEE PROFILE SEE PROFILE
Ashley Akbari Caroline Dale
Swansea University London School of Hygiene and Tropical Medicine
375 PUBLICATIONS 3,317 CITATIONS 57 PUBLICATIONS 4,094 CITATIONS
SEE PROFILE SEE PROFILE
All content following this page was uploaded by Ashley Akbari on 03 August 2023.
The user has requested enhancement of the downloaded file.
Articles
Antipsychotic drug prescribing and mortality in people with
dementia before and during the COVID-19 pandemic:
a retrospective cohort study in Wales, UK
Christian Schnier, Aoife McCarthy, Daniel R Morales, Ashley Akbari, Reecha Sofat, Caroline Dale, Rohan Takhar, Mamas A Mamas,
Kamlesh Khunti, Francesco Zaccardi, Cathie LM Sudlow, Tim Wilkinson, on behalf of the CVD-COVID-UK/COVID-IMPACT Consortium
Summary
Background Concerns have been raised that antipsychotic drug prescribing, which has been associated with increased Lancet Healthy Longev 2023;
mortality in people with dementia, might have increased during the COVID-19 pandemic due to social restrictions 4: e421–30
imposed to limit the spread of SARS-CoV-2. We used multisource, routinely collected health-care data from Wales, UK See Comment page e366
to investigate prescribing and mortality variations in people with dementia before and during the COVID-19 The Royal (Dick) School of
pandemic. Veterinary Studies
(C Schnier PhD), Edinburgh
Medical School
Methods In this retrospective cohort study, we used individual-level, anonymised, population-scale linked health data (A McCarthy MRes), Usher
to identify adults aged 60 years and older with a diagnosis of dementia in Wales, UK. We used the CVD-COVID-UK Institute
initiative to access Welsh routinely collected electronic health record data from the Secure Anonymised Information (Prof C L M Sudlow DPhil), and
Centre for Clinical Brain
Linkage (SAIL) Databank. Patients who were alive and registered with a SAIL general practice on Jan 1, 2016, and who
Sciences UK (Prof C L M Sudlow,
received a dementia diagnosis before the age of 60 years and before or during the study period were included. We T Wilkinson PhD), University of
explored antipsychotic drug prescribing rate changes over 67 months, between Jan 1, 2016, and Aug 1, 2021, overall Edinburgh, Edinburgh, UK;
and stratified by age and dementia subtype. We used time-series analyses to examine all-cause and myocardial Division of Population Health
and Genomics, University of
infarction and stroke mortality over the study period and identified the leading causes of death in people with Dundee, Dundee, UK
dementia between Jan 1, 2020, and Aug 1, 2021. (D R Morales PhD); Department
of Public Health, University of
Findings Of 3 106 690 participants in SAIL between Jan 1, 2016 and Aug 1, 2021, 57 396 people (35 148 [61·2%] women Southern Denmark, Odense,
Denmark (D R Morales);
and 22 248 [38·8%] men) met inclusion criteria for this study and contributed 101 428 person-years of follow-up. Of Swansea University Medical
the 57 396 people with dementia, 11 929 (20·8%) were prescribed an antipsychotic drug at any point during follow-up. School, Swansea University,
Accounting for seasonality, antipsychotic drug prescribing increased during the second half of 2019 and Swansea, UK (A Akbari MSc);
throughout 2020. However, the absolute difference in prescribing rates was small, ranging from 1253 prescriptions Department of Pharmacology
and Therapeutics, University of
per 10 000 person-months in March, 2019, to 1305 per 10 000 person-months in September, 2020. All-cause mortality Liverpool, Liverpool, UK
and stroke mortality increased throughout 2020, while myocardial infarction mortality declined. From Jan 1, 2020, to (Prof R Sofat PhD, C Dale PhD,
Aug 1, 2021, 1286 (17·1%) of 7508 participants who died had COVID-19 recorded as the underlying cause of death. R Takhar MSc); British Heart
Foundation Data Science
Centre, Health Data Research
Interpretation During the COVID-19 pandemic, antipsychotic drug prescribing in people with dementia in the UK UK, London, UK (Prof R Sofat,
increased slightly; however, it is unlikely that this was solely related to the pandemic and this increase was unlikely to Prof C L M Sudlow); Keele
be a major factor in the substantial increase in mortality during 2020. The long-term increase in antipsychotic drug Cardiovascular Research Group,
prescribing in younger people and in those with Alzheimer’s disease warrants further investigation using resources Keele University, Stoke-on-
Trent, UK
with access to more granular clinical data. Although deprescribing antipsychotic medications remains an essential (Prof M A Mamas DPhil);
aspect of dementia care, the results of this study suggest that changes in prescribing and deprescribing practices as a Diabetes Research Centre and
result of the COVID-19 pandemic are not required. Real World Evidence Unit,
University of Leicester,
Leicester, UK (Prof K Khunti MD,
Funding British Heart Foundation (via the British Heart Foundation Data Science Centre led by Health Data Research F Zaccardi PhD); Sunnybrook
UK), and the Scottish Neurological Research Fund. Research Institute, University
of Toronto, Toronto, ON,
Canada (T Wilkinson)
Copyright © 2023 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license.
Correspondence to:
Dr Tim Wilkinson, Centre for
Introduction Antipsychotic medications can be used to treat Clinical Brain Sciences, University
An estimated 57 million people worldwide live with symptoms of agitation, aggression, distress, and of Edinburgh,
dementia.1 The COVID-19 pandemic has dispro psychosis in people with dementia. However, anti Edinburgh EH16 4SB, UK
tim.wilkinson@ed.ac.uk
portionately affected people with dementia, who are psychotic use has been associated with an increased risk
more likely than people without dementia to be infected of adverse outcomes, such as stroke,5,6 myocardial
by SARS-CoV-2 and develop severe disease.2,3 In addition, infarction,7,8 and death.9,10 As a result, many countries
social restrictions imposed to limit the spread of have restrictions on the use of these drugs in people with
SARS-CoV-2 might be associated with a worsening of dementia.11,12 The UK National Institute for Health and
neuropsychiatric symptoms in people with dementia.4 Care Excellence’s clinical guidance states that
www.thelancet.com/healthy-longevity Vol 4 August 2023 e421
Articles
Research in context
Evidence before this study Wales, UK. By accounting for seasonal variations in prescribing
We searched Ovid MEDLINE with no language restrictions for and mortality, we showed that the absolute increase in
studies describing antipsychotic drug prescribing changes in antipsychotic drug prescribing in people with dementia of any
people with dementia during the COVID-19 pandemic, cause during the COVID-19 pandemic was small. By contrast,
published between Jan 1, 2020, and March 22, 2022. The antipsychotic drug prescribing in the youngest age group
following search terms were used: (exp Antipsychotic Agents/ (60–64 years) and in people with a subtype diagnosis of
OR antipsychotic.mp OR neuroleptic.mp OR risperidone.mp Alzheimer’s disease increased throughout the 5-year study
OR exp Risperidone/ OR quetiapine.mp OR exp Quetiapine period. Accounting for seasonal variation, all-cause mortality
Fumarate/ OR olanzapine.mp OR exp Olanzapine/ OR exp rates in people with dementia began to increase in late 2019
Psychotropic Drugs/ or psychotropic.mp) AND (exp and increased sharply during the COVID-19 pandemic.
Dementia/ OR exp Alzheimer Disease/ or Alzheimer.mp) AND COVID-19 became the leading non-dementia cause of death in
(prescri*.mp OR exp Prescriptions/ OR exp Electronic people with dementia from 2020 to 2021. Stroke mortality
Prescribing/ OR trend*.mp OR time series.mp). The search increased during the pandemic, following a similar pattern to
identified 128 published studies, of which three were eligible that of all-cause mortality, whereas myocardial infarction rates
for inclusion. Two studies, based on data from England and decreased. Our study identified that the increase in
the USA, compared antipsychotic drug prescribing in people antipsychotic drug prescribing in the UK during the COVID-19
with dementia before and during the COVID-19 pandemic. pandemic was smaller than suggested by previous studies, and
Both reported an increase in the proportion of patients was unlikely to be solely due to the pandemic.
prescribed an antipsychotic drug after the onset of the
Implications of all the available evidence
COVID-19 pandemic. A third study, from the Netherlands,
During the COVID-19 pandemic, we observed a large increase in
reported antipsychotic drug prescription changes in nursing
all-cause and stroke mortality in people with dementia. When
home residents with dementia during the first 4 months of
seasonal variations are accounted for, antipsychotic drug
the COVID-19 pandemic, comparing prescribing rates to the
prescribing rates in all-cause dementia increased by a small
timings of lifting social restrictions, showing that
amount before and during the pandemic in the UK, which is
antipsychotic drug prescribing rates remained constant
unlikely to have been responsible for the large mortality
throughout this period.
increases seen during the same period. Our results suggest that
Added value of this study significant changes in antipsychotic drug prescribing practices
We did age-standardised time-series analyses using as a result of the pandemic are not required. The increased
comprehensive, linked, anonymised, individual-level, routinely prescribing rates in younger age groups and in people with
collected, population-scale health data for the population of Alzheimer’s disease warrants further investigation.
antipsychotic medications should only be used when COVID-19 pandemic. We also aimed to investigate the
alternative approaches have failed, and if the patient is in potential impact of the COVID-19 pandemic on people
severe distress or at risk of harming themselves or with dementia and explore changes in all-cause, myocardial
others.13 infarction, and stroke mortality over the same period.
Concerns have been raised that rates of antipsychotic
drug prescribing for people with dementia might have Methods
increased in the UK during the early months of the Study design and participants
COVID-19 pandemic.14,15 The National Health We did a retrospective cohort study using routinely
Service (NHS) England reports monthly on the proportion collected linked health data from Wales, UK. We pre-
For the pre-published protocol of people with dementia who are prescribed an published the protocol with disease phenotyping codes.
see https://github.com/BHFDSC/ antipsychotic drug—a proportion that remained stable The CVD-COVID-UK Consortium is a UK-wide
CCU016_01
in 2018–19 but that appeared to increase in March, 2020, initiative established to accelerate research on COVID-19
For more on the CVD-COVID-UK
around the time social restrictions were introduced in and cardiovascular disease by facilitating access to linked,
Consortium see https://www.
hdruk.ac.uk/projects/cvd-covid- England to reduce the spread of SARS-CoV-2.14 Although routinely collected, electronic health record data from
uk-project/ such group-level data are useful for the understanding of England, Scotland, and Wales.16 For this study, we used
overall variations, they do not provide detailed information the CVD-COVID-UK initiative to access Welsh routinely
For the SAIL Databank see on the demographic details, seasonal variation, and linked collected electronic health record data from the Secure
https://saildatabank.com health outcomes associated with medication use in this Anonymised Information Linkage (SAIL) Databank.
population. In this study, we used individual-level, SAIL contains anonymised, individual-level, population-
routinely collected, linked health data from Wales, UK, and scale, linked, routinely collected electronic health record
aimed to investigate changes in antipsychotic drug and social care data sources for the population of
prescribing in people with dementia before and during the approximately 3 million people in Wales, UK, who
e422 www.thelancet.com/healthy-longevity Vol 4 August 2023
Articles
receive much of their health care through the NHS.17 The North East–Newcastle and North Tyneside 2
Primary care data are available in SAIL for approximately research ethics committee provided ethical approval for
86% of the Welsh population. Data are accessed via a the CVD-COVID-UK research programme. In
remotely accessible, privacy-protecting, trusted research accordance with Data Protection Act and the
environment. UK General Data Protection Regulation, individual
We created a population-based cohort of people with participant consent was not required for this study
dementia using linked, individual-level, anonymised data because the data were anonymised.
sources. The Welsh Longitudinal General Practice dataset
was used to obtain primary care diagnoses and Procedures and outcomes
prescriptions. The Patient Episode Database for Wales We defined exposure to antipsychotic medications during
provided diagnostic information arising from hospital the study window using prescription data, which are part
admissions. The Annual District Death Extract, Annual of primary care data (appendix p 5). We also identified
District Death Daily, and Consolidated Death Data Source exposure to benzodiazepines, an alternative class of
were combined for mortality data. The Lower-layer Super drugs used to treat agitation or distress in people with
Output Area of residence and associated Welsh Index of dementia, to investigate whether any change seen in
Multiple Deprivation (Welsh Demographic Service antipsychotic drug prescribing was specific to that
Dataset) were used for demographic information. The medication class or reflected changes in prescribing rates
Care Home Dataset was used for care home information. across all psychotropic medications.
Sex data were collected via a combination of medical For descriptive purposes, we estimated frailty in
records from birth, and self-reported from patients if participants with a minimum of 5 years of available
registering with a new general practice. primary care data before the study start date using the
We defined the study period from Jan 1, 2016, to electronic Frailty Index,21 which uses primary care data to
Aug 1, 2021 (67 months). Follow-up for each participant estimate an individual participant’s frailty (defined as fit,
started at the earliest date of dementia diagnosis or, if a or mild, moderate, or severe frailty). We used the
participant received a dementia diagnosis before the preceding 5 years of primary care data to calculate the
study start date, on Jan 1, 2016. Follow-up for each electronic Frailty Index.
participant ended at the date of death, deregistration with We used mortality data to describe changes in all-cause
a SAIL general practice, or Aug 1, 2021, whichever was mortality and mortality due to myocardial infarction or
earliest. For reference, the first case of COVID-19 in ischaemic stroke over the study period. We used fatal
the UK was recorded in January, 2020, and the UK’s first ischaemic stroke to investigate cerebrovascular outcomes
nationwide lockdown to mitigate the spread of the virus and myocardial infarction to investigate cardiovascular
began in March, 2020. outcomes, to avoid the uncertainty of whether repeated
We included all patients who were alive and registered non-fatal stroke or myocardial infarction codes, such as
with a SAIL general practice on Jan 1, 2016, and who those identified in hospital admissions data, represent
received a dementia diagnosis before (using all available recurrent events or the same event coded multiple times.
previous data) or during the study period. We excluded We used the code lists for stroke and myocardial
people who received a diagnosis of dementia before age infarction that were developed during the creation of the
60 years due to the low rates of dementia and dementia- SAIL Dementia electronic cohort (appendix p 6).17
related mortality and low accuracy of dementia diagnostic To identify causes of death, we grouped International
coding before this age.18,19 Classification of Diseases codes using the same method
We used a validated list of codes, namely Read Codes used by the Office for National Statistics when collating
(version 2) for primary care and International Classification UK mortality figures, with the addition of the new
of Diseases (tenth revision) for hospital admissions, to COVID-19 codes (U07.1 and U07.2).22
identify people with all-cause dementia (appendix pp 2–4).20 See Online for appendix
We defined dementia as the presence of at least Statistical analysis
one dementia code in either data source, using the date of We calculated the age-standardised monthly rate of
the first dementia code as the date of diagnosis. We did not antipsychotic and benzodiazepine prescribing between
use a prescription of a dementia medication (ie, donepezil, Jan 1, 2016, and Aug 1, 2021 (67 months) in people with
rivastigmine, galantamine, or memantine) to identify dementia. We also stratified antipsychotic drug
dementia cases but, for people with a prescription for a prescribing by age (in 5-year intervals). We used an
dementia medication before the date of their first dementia autoregressive integrated moving average model to
diagnostic code, we used the date of the first prescription conduct time-series analyses. This model involves
as the date of dementia diagnosis. We defined dementia decomposing the raw data into seasonal, trend and
subtypes (eg, Alzheimer’s disease or vascular dementia) as random and residual components using a moving
the presence of one or more subtype codes at any point average with a symmetric window (6 months on either
(appendix p 2). Dementia subtype categories were not side of the month under study, for a total of 13 months)
mutually exclusive. and an additive decomposition model. We standardised
www.thelancet.com/healthy-longevity Vol 4 August 2023 e423
Articles
ages on the basis of the age distribution of the study We counted the underlying causes of death in people
cohort in January, 2020 (the month in which the with dementia who died between Jan 1, 2020, and
first COVID-19 case was identified in the UK), to account Aug 1, 2021 (end of follow-up) to only assess the period
for changes in the age distribution of the cohort over the after the onset of COVID-19. We compared the number
study period. We also stratified the study sample by sex of participants for whom COVID-19 was listed as the
and dementia subtype. We could not stratify by care underlying cause of death with the number in whom
home versus community residence due to the risk of COVID-19 was listed anywhere on the death certificate
participant identification in groups with a small number (underlying and secondary).
of individuals. We described the prescribing patterns for We used structured query language for data manage
all antipsychotic drugs combined and for the top three ment and R (version 4.1.2) for statistical analysis. The
most commonly prescribed antipsychotic drugs statistical code is publicly available in the aforementioned
(risperidone, olanzapine, and quetiapine). To identify pre-published protocol.
potential associations between the start of the COVID-19
pandemic in 2020 and changes in antipsychotic drug Role of the funding source
prescribing, we conducted a prespecified outlier analysis The funders of the study had no role in study design,
in the seasonal autoregressive integrated moving data collection, data analysis, data interpretation, or
average models based on the method described by writing of the report.
Chen and Liu.23 We identified additive outliers, level
shifts, or transitory changes using the R package tsoutlier,24 Results
with timepoints identified as outliers if the t-statistic Of 3 106 690 participants included in SAIL between
exceeded 3·5. We presented demographic data with Jan 1, 2016, and Aug 1, 2021, 350 553 (11·3%) did not have
absolute values and percentages and medians with primary care data available and 2 696 232 (86·8%) did not
IQRs. have a dementia diagnosis before Aug 1, 2021. A
We conducted an age-standardised time-series analysis further 2509 (<0·1%) were then excluded for being
to investigate changes in all-cause mortality, fatal stroke, younger than 60 years at the time of dementia diagnosis,
and fatal myocardial infarction between Jan 1, 2016, and resulting in a final study cohort of 57 396 (1·8%) individuals
Aug 1, 2021. We compared mortality rates in which stroke (figure 1), who contributed 101 428 person-years of follow-
or myocardial infarction were listed as the primary cause up. 35 148 (61·2%) of 57 396 participants were women
on the death certificate with rates of these diagnoses and 22 248 (38·8%) were men. The median observation
listed anywhere on the death certificate. As with time per person was 32 months (IQR 12–66) and the
antipsychotic drug prescribing variations, we also median age at study start date was 82 years (76–87).
stratified all-cause mortality analysis by sex and dementia Participant demographics are displayed in the table. Data
subtype and conducted automated outlier detection. on race and ethnicity, which are poorly coded within UK
primary routinely collected datasets, were not collected.
3 106 690 participants in SAIL between
Of the 57 396 participants, 11 929 (20·8%) were
Jan 1, 2016, and Aug 1, 2021 prescribed an antipsychotic drug at any point during
follow-up. The median age of patients who received an
antipsychotic drug (80 years [IQR 64–86]) was lower than
350 553 excluded (primary care data not
available) that of patients who did not (82 years [76–87]), and a
higher proportion of patients who received an
antipsychotic drug were care-home residents at the study
2 756 137 with available primary care data start date (18·5% vs 14·4% of those who did not receive
included
antipsychotic medication; table).
The age-standardised prescribing rates for benzo
2 696 232 excluded (no dementia diagnosis diazepines, the three most prescribed antipsychotic
before Aug 1, 2021)
drugs (olanzapine, quetiapine, and risperidone), and
total antipsychotic medications are shown in figure 2.
59 905 with a dementia diagnosis before Risperidone and olanzapine prescribing rates increased
Aug 1, 2021 included
steadily throughout the study period, whereas quetiapine
prescribing reduced (appendix p 8). Age-stratified
2509 excluded (dementia diagnosis before antipsychotic drug prescribing rates appeared relatively
the age of 60 years)
static over the entire study period, except for the youngest
age group (60–64 years), in whom prescribing rates
57 396 included in study population doubled over the 5 years of the study (appendix p 10).
In March, 2020 (early in the COVID-19 pandemic),
Figure 1: Study profile 12·9% of people with dementia were prescribed an
SAIL=Secure Anonymised Information Linkage Databank antipsychotic drug, compared with 12·5% in March, 2019.
e424 www.thelancet.com/healthy-longevity Vol 4 August 2023
Articles
Total cohort Subpopulation 1500
(n=57 396) exposed to
Number of prescriptions per 10 000 person-months
antipsychotic
drugs
(n=11 929)
Total observation time, 101 428 22 699 1000 Drug class
person-years All antipsychotic drugs
Age at study start date 82 (76–87) 80 (64–86) Benzodiazepines
Olanzapine
Sex
Quetiapine
Female 35 148 (61·2%) 7115 (59·6%) Risperidone
Male 22 248 (38·8%) 4814 (40·4%) 500
Deprivation, quintiles*
1 (most deprived) 10 624 (18·5%) 2375 (19·9%)
2 11 656 (20·3%) 2513 (21·1%)
3 11 091 (19·3%) 2200 (18·4%)
0
4 11 425 (19·9%) 2313 (19·4%) 2016 2018 2020
5 (least deprived) 12 600 (21·9%) 2528 (21·2%) Year
Resident in care home* 8271 (14·4%) 2206 (18·5%)
Figure 2: Antipsychotic drug prescribing rates
Dementia subtype†
Rates are age-standardised. Benzodiazepine prescribing is included for
Alzheimer’s disease 25 407 (44·3%) 5738 (48·1%) comparison. Dotted vertical line indicates March, 2020 (start of the first UK-wide
Vascular dementia 17 720 (30·9%) 4302 (36·1%) lockdown to reduce the spread of SARS-CoV-2).
Frontotemporal dementia 571 (0·9%) 183 (1·5%)
Dementia with Lewy bodies 1044 (1·8%) 388 (3·3%) with Alzheimer’s disease increased steadily throughout
Not specified 17 506 (30·5%) 2835 (23·8%) the entire study period, with a steep increase during the
Date of dementia diagnosis second half of 2019, peaking in mid-2020 (figure 3B).
Before Jan 1, 2016 35 940 (62·6%) 6580 (55·2%) Antipsychotic drug prescribing changes in the subgroup
Between Jan 1, 2016 and Aug 1, 21 456 (37·4%) 5349 (44·8%) with vascular dementia showed a similar pattern to that
2021 of all-cause dementia (figure 3C).
Electronic frailty index score* During the 5-year study period, 35 565 (62·0%)
Fit 12 255 (21·4%) 1771 (14·8%) participants died. The median age of death was 87 years
Mild frailty 11 857 (20·7%) 2017 (16·9%) (IQR 82–91). Age-standardised all-cause mortality
Moderate frailty 5240 (9·1%) 956 (8·0%) declined from 2018 until late 2019, then increased sharply
Severe frailty 576 (1·0%) 100 (0·8%) and continued to increase throughout early and mid-2020
Not assessable‡ 27 468 (47·9%) 7085 (59·4%) (figure 4A).
Previous stroke* 7213 (12·6%) 1441 (12·1%) The pattern of fatal stroke rates was similar to that of
Previous myocardial infarction* 6267 (10·9%) 1242 (10·4%) all-cause mortality, with rates declining during 2018 to
Data are n (%) or median (IQR), unless otherwise specified. Demographics of the
mid-2019, followed by an increase in the second half
whole cohort and subgroup who were prescribed an antipsychotic drug at any of 2019, which continued throughout 2020 (figure 4B).
point during follow-up. *Before or at the study start date (Jan 1, 2016). The peak in stroke mortality in August, 2020 (23 deaths
†Categories are not mutually exclusive apart from the not specified category,
which reflects the number of participants with no subtype code. ‡Electronic frailty
per 10 000 person-months) was similar to that in
index could only be calculated for participants with 5 years of available primary September, 2017 (24 per 10 000 person-months).
care data before the study start date. Two peaks in stroke mortality during the COVID-19
Table: Participant characteristics
pandemic were noted, coinciding with all-cause mortality
peaks. During these peaks, a smaller proportion of
strokes were recorded in the primary position of the
Accounting for seasonal changes, antipsychotic drug death certificate than in any position, showing a shift
prescribing in people with all-cause dementia fell towards stroke as a contributing (rather than underlying)
between 2017 and 2019 (figure 3A), then started to cause of death (appendix p 12).
increase in the second half of 2019, continued to increase Fatal myocardial infarction rates declined throughout
throughout 2020, and peaked in the second half of 2020. the study period (figure 4C). After accounting for
However, the absolute change in prescribing between the seasonal effects, there was no noticeable change in
lowest and highest rates was relatively small (1253 myocardial infarction mortality rates following the onset
prescriptions per 10 000 person-months in March, 2019, of the COVID-19 pandemic.
compared with 1305 per 10 000 person-months in Between Jan 1, 2020, and Aug 1, 2021, 7508 (37·5%) of
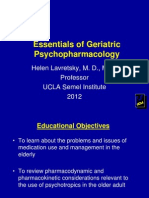
September, 2020). The outlier analysis detected no 20 042 participants died. The most frequently recorded
outliers between March, 2020, and August, 2021. By underlying cause of death was dementia, whereas
contrast, antipsychotic drug prescribing in participants COVID-19 was the second most common underlying
www.thelancet.com/healthy-longevity Vol 4 August 2023 e425
Articles
A Decomposition of additive time series
cause of death during this period (figure 5). Of the
1350
7508 participants who died, 1451 (19·3%) had COVID-19
1300 listed in any position on the death certificate, and
Data
1250 1286 (17·1%) had COVID-19 recorded as the underlying
1200 cause of death, meaning that 1286 (6·4%) of 20 042
1300 participants alive on Jan 1, 2020, died from COVID-19 by
1290
Trend
1280 Aug 1, 2021.
1270
1260
The median age at death from COVID-19 during this
period was the same as for death from any cause
50
Seasonal
25 (87 years [IQR 81–92]).
0
–25
Discussion
40
Remainder
20 We used routinely collected health data to examine
0 changes in antipsychotic drug prescribing and mortality
–20
before and during the COVID-19 pandemic.
2016 2017 2018 2019 2020 2021
Antipsychotic drug prescribing rates for people with
Year
dementia increased in 2019 and continued to increase
B Decomposition of additive time series during 2020, but the absolute change was small and on a
1350 background of lower rates of prescribing over the
1300
previous 2 years. Antipsychotic drug prescribing in
Data
1250
1200
1150 people with a subtype diagnosis of Alzheimer’s disease
increased throughout the 5-year study period. From
1290 2020 onwards, COVID-19 became the leading non-
Trend
1260
1230 dementia cause of death in people with dementia.
After accounting for seasonal effects on prescribing,
50 we observed a small increase in the proportion of people
Seasonal
25
0 with dementia prescribed antipsychotic medications
–25 following the onset of the COVID-19 pandemic. However,
50 the increased rates of prescribing began in the months
Remainder
25 before the arrival of COVID-19, suggesting that the
0
–25 COVID-19 pandemic might not have been the only cause
2016 2017 2018 2019 2020 2021 of the change. The age-stratified analysis showed a
Year notable increase in antipsychotic drug prescribing in the
youngest age group (60–64 years) during the 5-year study
C Decomposition of additive time series
period, but the reasons for this finding are unclear and
1600
1500 merit further investigation.
Data
1500 Howard and colleagues14 highlighted an increased
1450
1400 proportion of patients with dementia being prescribed
1525 antipsychotic drugs in 2020, compared with previous
1500
years, on the basis of publicly available NHS safety data
Trend
1475
1450 in England. Although our study identified an increase in
1450
75 antipsychotic drug prescribing between 2019 and 2020,
the use of a time-series analysis showed that, once
Seasonal
50
0 seasonal variations were accounted for, the absolute
–25
increase was minimal and occurred following particularly
60
low prescribing rates over the previous 2 years.
Remainder
40
0 A recent study by Luo and colleagues25 analysed routine
–40 health databases from six countries—France, Germany,
2016 2017 2018 2019 2020 2021 Italy, South Korea, the USA, and the UK—to investigate
Year the rates of antipsychotic drug prescribing in people with
Figure 3: Changes in antipsychotic drug prescribing rates in people with all-cause dementia (A), Alzheimer’s dementia during the COVID-19 pandemic. In keeping
disease (B), and vascular dementia (C) with the findings from our study, after the application of
Age-standardised, additive, autoregressive, integrated, moving average time-series model, accounting for interrupted time series, no substantial changes in
seasonal variations in prescribing. The data panel shows age-standardised prescribing rates. The trend panel shows
prescribing rates were observed before and after the
the trend of prescribing rates, accounting for seasonal variations. The seasonal panel shows the seasonal changes
in prescribing rates during the study period. The remainder panel shows the difference between the raw data and advent of COVID-19 in the UK, France, and South Korea.
the seasonal trend. The grey bars to the right of each panel show the relative scales of the components. Each grey An immediate increase in prescribing was identified in
bar represents the same length but as the plots are on different scales, the bars vary in size. Italy, and an immediate decrease was observed in
e426 www.thelancet.com/healthy-longevity Vol 4 August 2023
Articles
Germany. Conflicting variations were observed in the admitted to hospital, which probably led to
two included US datasets. The extent to which the underreporting of COVID-19 on death certificates.28
differing results across countries in Luo and colleagues’ Stroke mortality rate variations largely followed that of
study represent genuine differences in prescribing all-cause mortality. Following a reduction in stroke
practices during the pandemic, as opposed to differences mortality during 2018, we observed an increase in the
in approach to the coding of routine data, issues with second half of 2019, which continued throughout 2020,
data harmonisation, or models of health care, remains
unclear. A Decomposition of additive time series
Harrison and colleagues15 used routinely collected data 500
from the USA to compare the proportion of people with 400
Data
300
dementia prescribed an antipsychotic drug in the 30 days 200
before attendance at a health-care organisation 320
(eg, hospital or primary care centre) in 2020, compared Trend
300
280
with 2019. In Harrison and colleagues’ study, 16·4% of 260
patients were prescribed an antipsychotic drug 240
80
during 2020, compared with 14·7% in 2019. People
Seasonal
40
attending health-care centres in 2020 were on average 0
−40
more likely to be unwell than in the previous year, given
the concerns about nosocomial COVID-19 transmission, 200
Remainder
which might have biased the findings towards increased 100
rates of antipsychotic drug use in this study. 0
Sizoo and colleagues26 investigated antipsychotic drug 2016 2017 2018 2019 2020 2021
prescribing rates in psychogeriatric residents with Year
dementia in the Netherlands, before and during national
lockdowns. The proportion of people prescribed an B Decomposition of additive time series
35
antipsychotic drug was high (21·0–22·9%), reflecting the 30
Data
25
known higher rates of antipsychotic drug use in care- 20
home populations than in people not living in care 15
homes, but they did not identify a change in prescribing 24
22
practices over the study period.
Trend
20
Our analysis showed a marked increase in all-cause 18
mortality from late 2019 onwards, with two peaks in 2020
and early 2021, which coincided with the known peaks in 4
Seasonal
2
COVID-19 transmission in the UK.27 Previous studies 0
−2
have shown that people with dementia are at an increased
risk of severe symptoms or death from COVID-19.2 10
Remainder
5
From January, 2020, to August, 2021, COVID-19 0
became the leading non-dementia underlying cause of −5
death in people with dementia. According to our analysis, 2016 2017 2018 2019 2020 2021
about 6% of all people with dementia who were alive at Year
the start of 2020 died of COVID-19 over the subsequent C Decomposition of additive time series
19 months. This proportion is likely to be an
10·0
underestimate due to undertesting of COVID-19 early in
Data
7·5
the pandemic in the UK, particularly for those not 5·0
8
Trend
7
6
Figure 4: Changes in all-cause and cause-specific mortality rates
(A) All-cause mortality. (B) Stroke mortality. (C) Myocardial infarction mortality. 2
Seasonal
Age-standardised, additive, autoregressive, integrated, moving average time- 1
series model, accounting for seasonal variations in mortality. For all-cause 0
mortality, an outlier analysis detected outliers in April, May, and November, 2020, −1
and in January, 2021. The data panel shows the age-standardised mortality rates. 3
Remainder
The trend panel shows the trend of mortality rates, accounting for seasonal 2
1
trends. The seasonal panel shows the seasonal changes in prescribing rates during 0
−1
the study period. The remainder panel shows the difference between the raw −2
data and the seasonal trend. The grey bars to the right of each panel show the 2016 2017 2018 2019 2020 2021
relative scales of the components. Each grey bar represents the same length but Year
as the plots are on different scales, the bars vary in size.
www.thelancet.com/healthy-longevity Vol 4 August 2023 e427
Articles
indication are at an increased risk of death from
COVID-19.30
This study benefited from the application of a validated
code list to multiple complementary data sources to
identify people with dementia.20 We used individual-level,
linked, near-nationwide, routinely collected health data
to construct a population-based cohort. The use of time-
Dementia COVID-19 series analyses allowed us to account for seasonal
(42%) (17%)
variations in antipsychotic drug prescribing and
mortality, providing a more nuanced interpretation of
changes over the 5-year period.
Our study has several limitations. We used mortality
data to study fatal stroke and myocardial infarction as
outcomes to avoid issues with establishing whether
repeated codes reflect recurrent events or duplicate
Chronic
Ischaemic lung coding of previous events, an approach that can
Cancer heart disease
(6%)
disease substantially underestimate true rates of stroke and
(4%) (3%)
myocardial infarction. Routinely collected health data
Other
(16%)
will not identify disease outcomes with perfect accuracy,
Arrhythmias (2%)
Parkinson's and death certificate data often have a lower positive
disease (3%)
Cerebrovascular predictive value and sensitivity than other datasets.19
disease
(5%) Pneumonia and Given the poor availability of COVID-19 tests in the UK
influenza (2%) early in the pandemic, the COVID-19 mortality results
derived from death registration data are probably
Figure 5: Treemap of leading underlying causes of death in people with underestimates.28
dementia from Jan 1, 2020, to Aug 1, 2021 Despite these limitations, our study provides evidence
of a large increase in stroke and all-cause mortality in
albeit with a lower peak than in 2017. During the peaks in people with dementia during the COVID-19 pandemic,
mortality, stroke was more frequently listed as a although exact causes for this increase cannot be
contributing factor, rather than the underlying cause of pinpointed from these data, with COVID-19 becoming
death, which might in part be due to the increased risk of the most common non-dementia cause of death in this
stroke following COVID-19 infection.29 In contrast to population. A small absolute increase in antipsychotic
stroke, the rate of myocardial infarction deaths decreased drug prescribing in people with dementia was noted
during the study period, with no increase following the during the pandemic, but this rise had begun beforehand,
onset of COVID-19. suggesting that the pandemic was not the sole cause of
A previous meta-analysis identified that antipsychotic this small increase and was unlikely to be a major factor
drug use in people with dementia was consistently in the large concurrent increase in mortality.
associated with a 16% increased risk of stroke across cohort Deprescribing antipsychotic medications when possible
studies.5 Our study design could not establish whether a remains an essential aspect of dementia care, given that
causal relationship exists between changes in antipsychotic these drugs might be associated with increased mortality.
drug prescribing and resulting stroke and all-cause Contributors
mortality outcomes. Antipsychotic medications can be CS and AM were responsible for data curation, formal analysis, and
prescribed to people who have delirium, which they creation of figures. CS, AM, and TW accessed and verified the
underlying data. All authors were responsible for the methods,
develop because they are medically unwell. The disease participated in the revision of the manuscript, and had access to all the
causing the delirium might therefore lead to both an included data. AA and CS were responsible for data curation. AA, CLMS,
increased likelihood of antipsychotic drug use and and TW were responsible for project administration. CLMS and TW
increased mortality (termed confounding by indication). were responsible for funding acquisition and supervision. TW was
responsible for conceptualisation, writing the original manuscript, and
Additionally, people might receive antipsychotics submission for publication. All authors confirm they take full
palliatively to ease distress (reverse causation). In our view, responsibility for the decision to submit for publication.
the small increase in antipsychotic drug prescribing Declaration of interests
around the onset of the pandemic is unlikely to be CLMS reports a £10 million research grant from 2020 to 2024 to enable
responsible for the large increases in stroke and all-cause set-up of the British Heart Foundation Data Science Centre within
mortality throughout 2020. We suspect that most of the Health Data Research UK, the UK’s institute for health data science,
which as part of its activities has worked with Secure Anonymised
observed increase in mortality was caused by COVID-19, Information Linkage Wales (including a small investment of
although this suspicion cannot be refuted or confirmed by about £130 000 to enable access to the data relevant to this study); and is
this study design. Furthermore, some evidence suggests the Director of the British Heart Foundation Data Science Centre. CS
that older patients prescribed an antipsychotic drug for any was a co-investigator on a grant paid by the Benter Foundation to the
e428 www.thelancet.com/healthy-longevity Vol 4 August 2023
Articles
University of Edinburgh, Edinburgh, UK, for dementia research. All Cardiff University and specialist teams within the Welsh Government to
other authors declare no competing interests. develop new evidence which supports Prosperity for All by using the SAIL
Databank at Swansea University, to link and analyse anonymised data.
Data sharing
Administrative Data Research Wales is part of the Economic and Social
The North East–Newcastle and North Tyneside 2 research ethics
Research Council (part of UK Research and Innovation) funded
committee provided ethical approval for the CVD-COVID-UK/COVID-
Administrative Data Research UK (grant number ES/S007393/1). This
IMPACT research programme (REC no 20/NE/0161) to access, within
work was supported by the Wales COVID-19 Evidence Centre, funded by
secure trusted research environments, unconsented, whole-population,
Health and Care Research Wales. KK is supported by the National Institute
deidentified data from electronic health records collected as part of
for Health Research’s Applied Research Collaboration East Midlands and
patients’ routine health care. The CVD-COVID-UK/COVID-IMPACT For more on CVD-COVID-UK/
Leicester Biomedical Research Centre. TW was funded by a grant from the
Approvals & Oversight Board granted approval to this project to access COVID-IMPACT see https://
Scottish Neurological Research Fund, supported by the RS Macdonald
the data within the Secure Anonymised Information Linkage (SAIL) www.hdruk.ac.uk/projects/cvd-
charitable trust, and the Chief Scientist Office.
Databank. The deidentified data used in this study were made available covid-uk-project/
to accredited researchers only. Those wishing to gain access to the data References
should contact bhfdsc@hdruk.ac.uk in the first instance. The data used 1 Nichols E, Steinmetz JD, Vollset SE, et al. Estimation of the global
in this study are available in the SAIL Databank at Swansea University, prevalence of dementia in 2019 and forecasted prevalence in 2050:
Swansea, UK but, as restrictions apply, they are not publicly available. an analysis for the Global Burden of Disease Study 2019.
All proposals to use SAIL data are subject to review by an independent Lancet Public Health 2022; 7: e105–25.
Information Governance Review Panel (IGRP). Before any data can be 2 Numbers K, Brodaty H. The effects of the COVID-19 pandemic on
accessed, approval must be given by the IGRP. The IGRP considers each people with dementia. Nat Rev Neurol 2021; 17: 69–70.
project to ensure proper and appropriate use of SAIL data. When access 3 Atkins JL, Masoli JAH, Delgado J, et al. Preexisting comorbidities
has been granted, it is gained through a privacy protecting safe-haven predicting COVID-19 and mortality in the UK Biobank Community
Cohort. J Gerontol A Biol Sci Med Sci 2020; 75: 2224–30.
and remote access system referred to as the SAIL Gateway. SAIL has
established an application process to be followed by anyone who would 4 Manca R, De Marco M, Venneri A. The impact of COVID-19
infection and enforced prolonged social isolation on
like to access data via SAIL at https://www.saildatabank.com/
neuropsychiatric symptoms in older adults with and without
application-process. dementia: a review. Front Psychiatry 2020; 11: 585540.
Acknowledgments 5 Zivkovic S, Koh CH, Kaza N, Jackson CA. Antipsychotic drug use
This work was carried out with the support of the British Heart and risk of stroke and myocardial infarction: a systematic review
Foundation Data Science Centre led by Health Data Research UK (grant and meta-analysis. BMC Psychiatry 2019; 19: 189.
number SP/19/3/34678). This study made use of deidentified data held in 6 Hsu W-T, Esmaily-Fard A, Lai C-C, et al. Antipsychotics and the risk
the Secure Anonymised Information Linkage (SAIL) Wales Databank and of cerebrovascular accident: a systematic review and meta-analysis
made available via the British Heart Foundation Data Science Centre’s of observational studies. J Am Med Dir Assoc 2017; 18: 692–99.
CVD-COVID-UK/COVID-IMPACT consortium. This work used data 7 Yu Z-H, Jiang H-Y, Shao L, Zhou Y-Y, Shi H-Y, Ruan B. Use of
provided by patients and collected by the National Health Service (NHS) as antipsychotics and risk of myocardial infarction: a systematic review
and meta-analysis. Br J Clin Pharmacol 2016; 82: 624–32.
part of their care and support. We would also like to acknowledge all data
providers who make health-relevant data available for research. We wish to 8 Huang K-L, Fang C-J, Hsu C-C, Wu S-I, Juang JJ, Stewart R.
Myocardial infarction risk and antipsychotics use revisited: a meta-
acknowledge the collaborative partnership that enabled acquisition and
analysis of 10 observational studies. J Psychopharmacol 2017;
access to the deidentified data, which led to this output. The collaboration 31: 1544–55.
was led by the Swansea University Health Data Research UK team under
9 Schneider LS, Dagerman KS, Insel P. Risk of death with atypical
the direction of the Welsh Government Technical Advisory Cell and antipsychotic drug treatment for dementia: meta-analysis of
includes the following groups and organisations: the SAIL Databank, randomized placebo-controlled trials. JAMA 2005; 294: 1934–43.
Administrative Data Research Wales, Digital Health and Care Wales, 10 Nørgaard A, Jensen-Dahm C, Wimberley T, et al. Effect of
Public Health Wales, NHS Shared Services Partnership, and the Welsh antipsychotics on mortality risk in patients with dementia with and
Ambulance Service Trust. All research conducted has been completed without comorbidities. J Am Geriatr Soc 2022; 70: 1169–79.
under the permission and approval of the SAIL independent Information 11 Kuehn BM. FDA warns antipsychotic drugs may be risky for elderly.
Governance Review Panel (project number 0911). The British Heart JAMA 2005; 293: 2462.
Foundation Data Science Centre (grant number SP/19/3/34678, awarded to 12 Medicines and Healthcare Regulatory products Agency. New advice
Health Data Research UK) funded co-development (with NHS Digital) of issued on risperidone and olanzapine. 2004. https://webarchive.
the trusted research environment, provision of linked datasets, data access, nationalarchives.gov.uk/ukgwa/20111115115956/http://www.mhra.
user software licences, computational usage, and data management and gov.uk/PrintPreview/DefaultSP/CON002047
wrangling support, with additional contributions from the Health Data (accessed Aug 24, 2022).
Research UK Data and Connectivity component of the UK Government 13 National Institute for Health and Clinical Excellence. Dementia:
Chief Scientific Adviser’s National Core Studies programme to coordinate assessment, management and support for people living with
national COVID-19 priority research. Consortium partner organisations dementia and their carers. 2018. https://www.nice.org.uk/guidance/
funded the time of contributing data analysts, biostatisticians, ng97/chapter/Recommendations#pharmacological-interventions-
epidemiologists, and clinicians. This work was supported by the Con-COV for-dementia (accessed Aug 24, 2022).
team funded by the Medical Research Council (grant 14 Howard R, Burns A, Schneider L. Antipsychotic prescribing to
number MR/V028367/1), and by Health Data Research UK (grant number, people with dementia during COVID-19. Lancet Neurol 2020; 19: 892.
HDR-9006) funded by the UK Medical Research Council, Engineering and 15 Harrison SL, Buckley BJR, Lane DA, Underhill P, Lip GYH.
Physical Sciences Research Council, Economic and Social Research Associations between COVID-19 and 30-day thromboembolic
events and mortality in people with dementia receiving
Council, Department of Health and Social Care (England), Chief Scientist
antipsychotic medications. Pharmacol Res 2021; 167: 105534.
Office of the Scottish Government Health and Social Care Directorates,
16 Wood A, Denholm R, Hollings S, et al. Linked electronic health
Health and Social Care Research and Development Division
records for research on a nationwide cohort of more than 54 million
(Welsh Government), Public Health Agency (Northern Ireland), British people in England: data resource. BMJ 2021; 373: n826.
Heart Foundation, and the Wellcome Trust. This work was supported by
17 Schnier C, Wilkinson T, Akbari A, et al. The Secure Anonymised
the Administrative Data Research Wales programme of work. The Information Linkage databank Dementia e-cohort (SAIL-DeC).
Administrative Data Research Wales programme of work is aligned to the Int J Popul Data Sci 2020; 5: 1121.
priority themes as identified in the Welsh Government’s national strategy: 18 van de Vorst IE, Vaartjes I, Sinnecker LF, Beks LJM, Bots ML,
Prosperity for All. Administrative Data Research Wales brings together Koek HL. The validity of national hospital discharge register data on
data science experts at Swansea University Medical School, staff from the dementia: a comparative analysis using clinical data from a
Wales Institute of Social and Economic Research, Data and Methods at university medical centre. Neth J Med 2015; 73: 69–75.
www.thelancet.com/healthy-longevity Vol 4 August 2023 e429
Articles
19 Wilkinson T, Ly A, Schnier C, et al. Identifying dementia cases with 25 Luo H, Lau WCY, Chai Y, et al. Rates of antipsychotic drug
routinely collected health data: a systematic review. prescribing among people living with dementia during the
Alzheimers Dement 2018; 14: 1038–51. COVID-19 pandemic. JAMA Psychiatry 2023; 80: 211–19.
20 Wilkinson T, Schnier C, Bush K, et al. Identifying dementia 26 Sizoo EM, Thunnissen JA, van Loon AM, et al. The course of
outcomes in UK Biobank: a validation study of primary care, neuropsychiatric symptoms and psychotropic drug use in Dutch
hospital admissions and mortality data. Eur J Epidemiol 2019; nursing home patients with dementia during the first wave of
34: 557–65. COVID-19: a longitudinal cohort study. Int J Geriatr Psychiatry 2022;
21 Clegg A, Bates C, Young J, et al. Development and validation of an 37: gps.5693.
electronic frailty index using routine primary care electronic health 27 Barnard RC, Davies NG, Jit M, Edmunds WJ. Modelling the
record data. Age Ageing 2016; 45: 353–60. medium-term dynamics of SARS-CoV-2 transmission in England in
22 Office for National Statistics. Leading causes of death in England the omicron era. Nat Commun 2022; 13: 4879.
and Wales (revised 2016). People, population and community. 2017. 28 Aburto JM, Kashyap R, Schöley J, et al. Estimating the burden of
https://www.ons.gov.uk/peoplepopulationandcommunity/ the COVID-19 pandemic on mortality, life expectancy and lifespan
birthsdeathsandmarriages/deaths/methodologies/ inequality in England and Wales: a population-level analysis.
userguidetomortalitystatistics/ J Epidemiol Community Health 2021; 75: 735–40.
leadingcausesofdeathinenglandandwalesrevised2016 29 Merkler AE, Parikh NS, Mir S, et al. Risk of ischemic stroke in
(accessed June 3, 2021). patients with coronavirus disease 2019 (COVID-19) vs patients with
23 Chen C, Liu L-M. Joint estimation of model parameters and outlier influenza. JAMA Neurol 2020; 77: 1–7.
effects in time series. J Am Stat Assoc 1993; 88: 284–97. 30 Austria B, Haque R, Mittal S, et al. Mortality in association with
24 López-de-Lacalle J. tsoutliers: detection of outliers in time series. antipsychotic medication use and clinical outcomes among geriatric
R packageversion 0.6–8. 2019. https://CRAN.R-project.org/ psychiatry outpatients with COVID-19. PLoS One 2021;
package=tsoutliers (accessed July 19, 2023). 16: e0258916.
e430 www.thelancet.com/healthy-longevity Vol 4 August 2023
View publication stats
You might also like
- PIIS2666756823001058Document10 pagesPIIS2666756823001058antoine2567No ratings yet
- Jurnal Covid-19Document12 pagesJurnal Covid-19mayankfauzanNo ratings yet
- COVID-19 Trajectories Among 57 Million Adults in England: A Cohort Study Using Electronic Health RecordsDocument17 pagesCOVID-19 Trajectories Among 57 Million Adults in England: A Cohort Study Using Electronic Health RecordsJudelle Enriquez-GazaNo ratings yet
- Trends in All-Cause Mortality Among People WitDocument8 pagesTrends in All-Cause Mortality Among People WitLinhNo ratings yet
- Mackenzie 2013Document10 pagesMackenzie 2013scribd.glowing960No ratings yet
- 1 s2.0 S2213219821012022 MainDocument10 pages1 s2.0 S2213219821012022 Main茹光毅No ratings yet
- Pen TingDocument9 pagesPen Tingabraham rumayaraNo ratings yet
- File DementiaDocument12 pagesFile DementiaLucienneNo ratings yet
- PIIS2213858720302722Document10 pagesPIIS2213858720302722juan carlos monasterio saezNo ratings yet
- Neurological and Neuropsychiatric Complications of COVID-19 in 153 Patients: A UK-wide Surveillance StudyDocument8 pagesNeurological and Neuropsychiatric Complications of COVID-19 in 153 Patients: A UK-wide Surveillance StudyJhonatan LadinoNo ratings yet
- A Comparative Study of Severity Ofpulmonary Tuberculosis Among Dibetics and Non Dibetics Patients in Tertiary Care HospitalDocument8 pagesA Comparative Study of Severity Ofpulmonary Tuberculosis Among Dibetics and Non Dibetics Patients in Tertiary Care HospitalIJAR JOURNALNo ratings yet
- Fu RongDocument9 pagesFu RongTín NguyễnNo ratings yet
- Articles: BackgroundDocument9 pagesArticles: BackgroundMuhammad AhmadNo ratings yet
- RiskDocument29 pagesRiskCarolinaNo ratings yet
- Clinical Utility of Existing and Second GenerationDocument10 pagesClinical Utility of Existing and Second GenerationSimbakutty VenkataramananNo ratings yet
- 2017 Article 3Document8 pages2017 Article 3Ocha24 TupamahuNo ratings yet
- Correll - 22 - Factors and Their Weight in Reducing Life Expectancy in SchizophreniaDocument9 pagesCorrell - 22 - Factors and Their Weight in Reducing Life Expectancy in SchizophreniaClaudia OvejasNo ratings yet
- Stark 2003Document5 pagesStark 2003Jorge Urrutia OrtizNo ratings yet
- Painful Diabetic Polyneuropathy: A Comprehensive Guide for CliniciansFrom EverandPainful Diabetic Polyneuropathy: A Comprehensive Guide for CliniciansNo ratings yet
- Jurnalul Clinic deDocument4 pagesJurnalul Clinic deIonescu RaduNo ratings yet
- An International Commentary On Dysphagia and Dysphonia During The COVID 19 PandemicDocument26 pagesAn International Commentary On Dysphagia and Dysphonia During The COVID 19 PandemicRomian ValenciaNo ratings yet
- Alta Incidencia de ACV Hemorrágico en IX Región - Doussoulin 2017Document2 pagesAlta Incidencia de ACV Hemorrágico en IX Región - Doussoulin 2017Abi Dennise Nahuelpán LienlafNo ratings yet
- How To OvercomeDocument19 pagesHow To OvercomeRyaneNo ratings yet
- The 2023 Duke-ISCVID Criteria For Infective Endocarditis: Updating The Modified Duke CriteriaDocument23 pagesThe 2023 Duke-ISCVID Criteria For Infective Endocarditis: Updating The Modified Duke CriteriaHand SanitizerNo ratings yet
- DoxycyclineDocument11 pagesDoxycyclineIrma Rahayu LatarissaNo ratings yet
- Temporal Trends and Patterns in Heart Failure Incidence: A Population-Based Study of 4 Million IndividualsDocument9 pagesTemporal Trends and Patterns in Heart Failure Incidence: A Population-Based Study of 4 Million Individualsabraham rumayaraNo ratings yet
- Study of Metabolic Syndrome and Diabetes Mellitus Among Ischemic Stroke Patients in A Tertiary Hospital, Northern KarnatakaDocument7 pagesStudy of Metabolic Syndrome and Diabetes Mellitus Among Ischemic Stroke Patients in A Tertiary Hospital, Northern KarnatakaIJAR JOURNALNo ratings yet
- Evidence-Practice Gaps in Lung Cancer: A Scoping Review: European Journal of Cancer Care October 2016Document13 pagesEvidence-Practice Gaps in Lung Cancer: A Scoping Review: European Journal of Cancer Care October 2016Dharpure Mr. Harshal Namdeorao --No ratings yet
- Evidence-Based Management of Acute Heart Failure PDFDocument11 pagesEvidence-Based Management of Acute Heart Failure PDFアレクサンダー ロドリゲスNo ratings yet
- Diabetes Tipo 2 y Mortalidad Relacionada Con COVID 19 en El Entorno de Cuidados IntensivosDocument8 pagesDiabetes Tipo 2 y Mortalidad Relacionada Con COVID 19 en El Entorno de Cuidados IntensivosDaniela VelascoNo ratings yet
- CultivosDocument19 pagesCultivosRodrigo SierraNo ratings yet
- Bmjopen 2011 000666Document6 pagesBmjopen 2011 000666Fabiola PortugalNo ratings yet
- Predicting Risk of Recurrent Acute Kidney Injury: A Systematic ReviewDocument8 pagesPredicting Risk of Recurrent Acute Kidney Injury: A Systematic ReviewJhon JeffreyNo ratings yet
- Jurnal Covid 19Document46 pagesJurnal Covid 19Adeta Yuniza100% (1)
- Gout and The Risk of Epilepsy A Population Based.44Document6 pagesGout and The Risk of Epilepsy A Population Based.44Afni Panggar BesiNo ratings yet
- 327 FullDocument2 pages327 FullfabaNo ratings yet
- Nejmoa 1911614Document14 pagesNejmoa 1911614Riandhani UpitariniaNo ratings yet
- Healthcare: Allergic Rhinitis and Laryngeal Pathology: Real-World EvidenceDocument9 pagesHealthcare: Allergic Rhinitis and Laryngeal Pathology: Real-World EvidencePutri Rizky AmaliaNo ratings yet
- Pa Nag Iot Akos 2015Document7 pagesPa Nag Iot Akos 2015Gabriel ParizotoNo ratings yet
- Multiple Sclerosis Lancet 2018Document15 pagesMultiple Sclerosis Lancet 2018Sarah Miryam CoffanoNo ratings yet
- Fry Et Al 2017Document9 pagesFry Et Al 2017Ernest YipNo ratings yet
- 8th R.LDocument54 pages8th R.LWilliam Tac anNo ratings yet
- Association Between BMI and COVID-19 - 210503 - 155148Document10 pagesAssociation Between BMI and COVID-19 - 210503 - 155148nNo ratings yet
- Politicas y Esteticas Del Cuerpo, Zandra PedrazaDocument6 pagesPoliticas y Esteticas Del Cuerpo, Zandra PedrazaJou ÁlvarezNo ratings yet
- Dehydration and Clinical Outcome in Hospitalised Older Adults: A Cohort StudyDocument8 pagesDehydration and Clinical Outcome in Hospitalised Older Adults: A Cohort StudyJonathan EdbertNo ratings yet
- 1st JournalDocument11 pages1st Journaloke boskuNo ratings yet
- Frampton 2021 LidDocument12 pagesFrampton 2021 LidDr Poonam Sharma VelamuriNo ratings yet
- Lavados 2021Document12 pagesLavados 2021Gian Franco Oneto TapiaNo ratings yet
- Oldridge2012 HeartQol1 PreprintDocument26 pagesOldridge2012 HeartQol1 PreprintNabhan BihaqiNo ratings yet
- Eclinicalmedicine: A # B # C D E F G H I J K L M N O P Q R S T U V W X Y Z # A # B C DDocument12 pagesEclinicalmedicine: A # B # C D E F G H I J K L M N O P Q R S T U V W X Y Z # A # B C Dyowan wandikboNo ratings yet
- Prevalence, Factors and Complication of Diabetes in An Underdeveloped Region of Khyber Pukhtun Khawa: A Cross-Sectional StudyDocument6 pagesPrevalence, Factors and Complication of Diabetes in An Underdeveloped Region of Khyber Pukhtun Khawa: A Cross-Sectional StudyOpenaccess Research paperNo ratings yet
- Body Mass Index and Mini Nutritional Assessment-Short Form Aspredictors of In-Geriatric Hospital Mortality in Older Adults WithCOVID-19Document7 pagesBody Mass Index and Mini Nutritional Assessment-Short Form Aspredictors of In-Geriatric Hospital Mortality in Older Adults WithCOVID-19Dani CapiNo ratings yet
- PIIS0140673622003270Document7 pagesPIIS0140673622003270chaivat kNo ratings yet
- 1 s2.0 S0920996420301584 MainDocument10 pages1 s2.0 S0920996420301584 MainAndreaNo ratings yet
- Nihr Rds Ukbnov25Document21 pagesNihr Rds Ukbnov25Rishi CaleyachettyNo ratings yet
- Ada Cvd-Renalcompendium Fin-WebDocument32 pagesAda Cvd-Renalcompendium Fin-WebJoseph Antonio Apaza GómezNo ratings yet
- The Prevalence and Risk Factors Associated With Type 2 Diabetic Retinopathy in RwandaDocument9 pagesThe Prevalence and Risk Factors Associated With Type 2 Diabetic Retinopathy in RwandaIJAR JOURNALNo ratings yet
- Multiple Sclerosis LancetDocument15 pagesMultiple Sclerosis LancetMichelleNo ratings yet
- Schizophrenia Case StudyDocument3 pagesSchizophrenia Case StudyKumar Suryavanshi100% (1)
- Mental Health Quiz Online - Psychiatric Disorders - Mental Health Nursing - Nursing OfficerDocument26 pagesMental Health Quiz Online - Psychiatric Disorders - Mental Health Nursing - Nursing OfficermanishjeswalNo ratings yet
- Autism Spectrum Disorders Etiology and PDocument7 pagesAutism Spectrum Disorders Etiology and PGabriela Lala100% (1)
- Pych Preboards QuestionsDocument18 pagesPych Preboards QuestionsPaul Lexus Gomez LorenzoNo ratings yet
- A Guide To The Judicious Use of Lab Tests in PsychiatryDocument8 pagesA Guide To The Judicious Use of Lab Tests in Psychiatrykoyote73100% (1)
- First Aid MneumonicsDocument17 pagesFirst Aid MneumonicsJay PatelNo ratings yet
- Acute and Transient Psychotic Disorders: Presented By: Dr. Karrar Husain Moderator: Dr. M. Amir UsmaniDocument65 pagesAcute and Transient Psychotic Disorders: Presented By: Dr. Karrar Husain Moderator: Dr. M. Amir Usmanitugba1234No ratings yet
- Essentials of Geriatric PsychiatryDocument87 pagesEssentials of Geriatric PsychiatryFeisalAlykhanNo ratings yet
- Psychiatric Practice TestDocument4 pagesPsychiatric Practice TestARISNo ratings yet
- Management of Neuropsychiatric Symptoms of Dementia - UpToDateDocument57 pagesManagement of Neuropsychiatric Symptoms of Dementia - UpToDateGaleno AgusNo ratings yet
- DepressionDocument10 pagesDepressionsalfaciNo ratings yet
- Irwin 1962Document6 pagesIrwin 1962Izhal StewartNo ratings yet
- Nicotine Use in Schizophrenia The Self Medication Hypotheses PDFDocument14 pagesNicotine Use in Schizophrenia The Self Medication Hypotheses PDFEmiNo ratings yet
- Book Review of Peter Bartlett, Oliver Lewis and Oliver Thorold, Mental Disability and The European Convention On Human RightsDocument6 pagesBook Review of Peter Bartlett, Oliver Lewis and Oliver Thorold, Mental Disability and The European Convention On Human RightsJohn RussellNo ratings yet
- About Psychiatric Drugs Side-EffectsDocument60 pagesAbout Psychiatric Drugs Side-EffectsKarthikeyan Sudarsana BabuNo ratings yet
- Chapter 31 - PsychosisDocument15 pagesChapter 31 - PsychosisDragutin PetrićNo ratings yet
- Abilify Dosing GuideDocument2 pagesAbilify Dosing GuidemtassyNo ratings yet
- Add-On Pharmacotherapy For PatientsDocument2 pagesAdd-On Pharmacotherapy For PatientsmarcoNo ratings yet
- Movement DisordersDocument10 pagesMovement DisordersAli 10No ratings yet
- Drug StudyDocument27 pagesDrug StudyMariefer EsplagoNo ratings yet
- Family Psychoeducation PsychosisDocument3 pagesFamily Psychoeducation PsychosisCharlesNo ratings yet
- Review TestDocument40 pagesReview TestJhozel QuiloNo ratings yet
- Schizophrenic DisorderDocument64 pagesSchizophrenic Disorder123soeryaNo ratings yet
- DRUG StudyDocument3 pagesDRUG StudyArfe BaquinquitoNo ratings yet
- Dementia Care 3 End of Life CareDocument7 pagesDementia Care 3 End of Life Caredogstar23100% (1)
- Mental Health E3 QuizletDocument2 pagesMental Health E3 QuizletTodd ColeNo ratings yet
- Update On Pharmacotherapy in Psychodermatological DisordersDocument12 pagesUpdate On Pharmacotherapy in Psychodermatological Disordersmaat1No ratings yet
- Drug Study FluphenazineDocument4 pagesDrug Study FluphenazineaolbinarNo ratings yet
- Tardive DyskinesiaDocument2 pagesTardive Dyskinesiajhonny12321No ratings yet
- Seroquel (Quetiapine)Document3 pagesSeroquel (Quetiapine)E100% (1)