You might also like
- Fluid and Electrolytes ManagementDocument21 pagesFluid and Electrolytes ManagementRasYa DINo ratings yet
- Treatment of Acute Hypokalaemia in AdultsDocument4 pagesTreatment of Acute Hypokalaemia in AdultsEmaNo ratings yet
- Item 6f - Acute Management of Hyperosmolar Hyperglycaemic StateDocument1 pageItem 6f - Acute Management of Hyperosmolar Hyperglycaemic StateStef AnNo ratings yet
- Treating and Monitoring Hypomagnesaemia For Non-Critical Areas of TrustDocument3 pagesTreating and Monitoring Hypomagnesaemia For Non-Critical Areas of Trustramy.elantaryNo ratings yet
- Hypokalaemia Guidelines v1 - May 2018Document9 pagesHypokalaemia Guidelines v1 - May 2018EmaNo ratings yet
- Adult Diabetic Ketoacidosis DKA Guideline South WestDocument6 pagesAdult Diabetic Ketoacidosis DKA Guideline South Westshada aaaNo ratings yet
- Commonly Prescribed Medications in Surgical Ed Sivakami Ver 5.0Document23 pagesCommonly Prescribed Medications in Surgical Ed Sivakami Ver 5.0Suiweng WongNo ratings yet
- MIL Vol 4Document6 pagesMIL Vol 4garywall.ukNo ratings yet
- Cisplatin-and-Etoposide (Ovarian Cancer)Document4 pagesCisplatin-and-Etoposide (Ovarian Cancer)Sindu SankarNo ratings yet
- Oncologic Emergencies Hypercalcemia of MalignancyDocument6 pagesOncologic Emergencies Hypercalcemia of MalignancyDapot SianiparNo ratings yet
- Potassium-Chloride-Intravenous ANMF1.0 20201208Document5 pagesPotassium-Chloride-Intravenous ANMF1.0 20201208aldyNo ratings yet
- Guideline For The Management of Hypokalaemia in Adults: Signs & SymptomsDocument2 pagesGuideline For The Management of Hypokalaemia in Adults: Signs & SymptomsmuzakiNo ratings yet
- Hypokalaemia PDFDocument2 pagesHypokalaemia PDFjenna1213No ratings yet
- Hypokalaemia PDFDocument2 pagesHypokalaemia PDFIulia RoxanaNo ratings yet
- Hypokalaemia PDFDocument2 pagesHypokalaemia PDFManuela KarinaaNo ratings yet
- Hypokalaemia PDFDocument2 pagesHypokalaemia PDFRisaNo ratings yet
- HyperkalaemiaDocument1 pageHyperkalaemiaRekaBNo ratings yet
- Poison and Antidote ChartDocument5 pagesPoison and Antidote ChartSusanne Mae Gonzales50% (2)
- Cisplatin-Pemetrexed (NSCLC)Document5 pagesCisplatin-Pemetrexed (NSCLC)Sindu SankarNo ratings yet
- Hyper Calc Emi ADocument26 pagesHyper Calc Emi AAman Tayal0% (1)
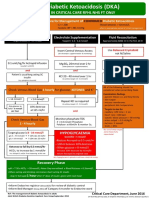
- Adult Diabetic Ketoacidosis (DKA) : For Use in Critical Care RFHL Nhs FT OnlyDocument1 pageAdult Diabetic Ketoacidosis (DKA) : For Use in Critical Care RFHL Nhs FT OnlyJung Bahadur SinghNo ratings yet
- Management of Hypokalaemia Clinical GuidelineDocument13 pagesManagement of Hypokalaemia Clinical GuidelineRadenroro Atih Utari RizkyNo ratings yet
- Lecture 1 Electrolyte ImbalanceDocument15 pagesLecture 1 Electrolyte ImbalanceSajib Chandra RoyNo ratings yet
- Inpatient Electrolyte RepletionDocument3 pagesInpatient Electrolyte Repletionapi-648757084No ratings yet
- NFCC. Chapter 8. ElectrolytesDocument13 pagesNFCC. Chapter 8. ElectrolytesOsman fadilNo ratings yet
- How Is Hypokalaemia Treated in Adults?: Medicines Q&AsDocument6 pagesHow Is Hypokalaemia Treated in Adults?: Medicines Q&AsNotForAbuseNo ratings yet
- Electrolyte Prescribe Gline AdultDocument2 pagesElectrolyte Prescribe Gline AdultMirelaNo ratings yet
- 205 Management of Hypo Kala Emi ADocument11 pages205 Management of Hypo Kala Emi AGresonNo ratings yet
- London Cancer Cisplatin Hydration Guideline v1Document2 pagesLondon Cancer Cisplatin Hydration Guideline v1dwi haris100% (1)
- Electrolye Repletion Inservice HandoutDocument4 pagesElectrolye Repletion Inservice Handoutapi-648891519No ratings yet
- Prescribing Information For The Administration of AminophyllineDocument2 pagesPrescribing Information For The Administration of AminophyllinekolperrNo ratings yet
- Paed Parenteral Fluid ThyDocument1 pagePaed Parenteral Fluid ThyZulia Ahmad BurhaniNo ratings yet
- Final 2Document11 pagesFinal 2Nikk LadeNo ratings yet
- Overdose and PoisoningDocument4 pagesOverdose and PoisoningMahmoud SelimNo ratings yet
- Syndrome of Inappropriate Adh Secretion (Siadh) PathophysiologyDocument2 pagesSyndrome of Inappropriate Adh Secretion (Siadh) PathophysiologyJuliana FeronNo ratings yet
- MTOR-Inhibitors - Switch From CNI: Commercially Available DrugsDocument3 pagesMTOR-Inhibitors - Switch From CNI: Commercially Available DrugshassanNo ratings yet
- Dka CalculatorDocument1 pageDka CalculatorTalib AdilNo ratings yet
- Icu ProtocolDocument4 pagesIcu Protocolmehal guptaNo ratings yet
- Case 1B Answer KeyDocument5 pagesCase 1B Answer KeyChettan KeralaNo ratings yet
- Management of Anesthesia: Diabetes MellitusDocument29 pagesManagement of Anesthesia: Diabetes MellitusHari PrasadNo ratings yet
- IVFluids Guideline Poster July 2017Document1 pageIVFluids Guideline Poster July 2017rana muzamilNo ratings yet
- HypokalemiaDocument7 pagesHypokalemiaNader SmadiNo ratings yet
- Hyponatremia Topic DiscussionDocument4 pagesHyponatremia Topic Discussionapi-647904873No ratings yet
- Paediatric Pam I DR On Ate IV MonographDocument2 pagesPaediatric Pam I DR On Ate IV MonographDouglas MutenyoNo ratings yet
- MGT of D KetoacidosisDocument5 pagesMGT of D Ketoacidosisshabatat2002No ratings yet
- HypocalcemiaDocument34 pagesHypocalcemiaClaudia IrimieNo ratings yet
- Salbutamol 2017: Newborn Use OnlyDocument3 pagesSalbutamol 2017: Newborn Use OnlynurfitriaNo ratings yet
- Calcium GluconateDocument1 pageCalcium GluconateDilip SenthNo ratings yet
- Amlodipine by HamidDocument21 pagesAmlodipine by HamidShaheen UiiahNo ratings yet
- DKA Guidelines Version 4.0 28 Dec 2016FINALDocument4 pagesDKA Guidelines Version 4.0 28 Dec 2016FINALbenNo ratings yet
- Canine Glaucoma - Medical and Surgical Traetment OptionsDocument6 pagesCanine Glaucoma - Medical and Surgical Traetment OptionsRochiWinchesterNo ratings yet
- Clinical Enquiry Comment/Case ManagementDocument9 pagesClinical Enquiry Comment/Case ManagementMian EhsanNo ratings yet
- Furosemide (Frusemide) 2017Document5 pagesFurosemide (Frusemide) 2017Akhmad Rafi'iNo ratings yet
- Algorithms For IV Fluid Therapy in Children and Young People in Hospital Iv Fluid Therapy in ChildrenDocument12 pagesAlgorithms For IV Fluid Therapy in Children and Young People in Hospital Iv Fluid Therapy in ChildrenSREEDEVI T SURESH0% (1)
- Glossary and Guidelines For Use: PreparationsDocument36 pagesGlossary and Guidelines For Use: PreparationsMuhammad ThaufiqurrakhmanNo ratings yet
- Zyl OricDocument3 pagesZyl OricMohammed IbrahimNo ratings yet
- Acute Management of Hypocalcaemia in AdultsDocument1 pageAcute Management of Hypocalcaemia in Adultsaimi hj zulkipliNo ratings yet
- Annex I Summary of Product CharacteristicsDocument29 pagesAnnex I Summary of Product CharacteristicslisnerisNo ratings yet
- Intro To AromatherapyDocument58 pagesIntro To AromatherapyrameshgounderNo ratings yet
- What Is COVID-19?: Most Common SymptomsDocument3 pagesWhat Is COVID-19?: Most Common SymptomsJerome LazaroNo ratings yet
- Bài Tập Trắc Nghiệm Anh 10- Chương Trình Thí ĐiểmDocument143 pagesBài Tập Trắc Nghiệm Anh 10- Chương Trình Thí ĐiểmPhong ĐâyNo ratings yet
- Geriatric SyndromesDocument3 pagesGeriatric SyndromesAhmad Badli MohemadNo ratings yet
- Needlestick InjuryDocument24 pagesNeedlestick InjuryAli AlisonNo ratings yet
- Magazine'21Document77 pagesMagazine'21nerdsonloose0906No ratings yet
- COVID 19 Science Report Therapeutics 4 May PDFDocument41 pagesCOVID 19 Science Report Therapeutics 4 May PDFjolamo1122916No ratings yet
- Final Clinical SurgeryDocument107 pagesFinal Clinical SurgeryMahmoud Farag100% (1)
- TR-AUTOHEMOTHERAPY AUTOLOGOUS BLOOD TRANSFUSION OZONE THERAPY Â AN UPDATEDocument43 pagesTR-AUTOHEMOTHERAPY AUTOLOGOUS BLOOD TRANSFUSION OZONE THERAPY Â AN UPDATEweb3351100% (1)
- Cimicifuga RacemosaDocument16 pagesCimicifuga RacemosaKamalNo ratings yet
- Ketamine and Its Effects On Sensory PerceptionDocument4 pagesKetamine and Its Effects On Sensory Perceptionapi-557854804No ratings yet
- Bearded Dragon Periodontal Disease-Aurora Animal HospitalDocument1 pageBearded Dragon Periodontal Disease-Aurora Animal HospitalPedro Trotsky DeathMaskNo ratings yet
- Nursing Drug StudyDocument12 pagesNursing Drug StudyJoshkorro Geronimo100% (2)
- 2020 Q2 SMEA: St. Mary'S College of Borongan, IncDocument49 pages2020 Q2 SMEA: St. Mary'S College of Borongan, Incacademic coordinatorNo ratings yet
- Certificate of Physical FitnessDocument2 pagesCertificate of Physical FitnessHarsh SahuNo ratings yet
- Nursing Care Plan: Actual ThreatsDocument7 pagesNursing Care Plan: Actual ThreatsJason OgalescoNo ratings yet
- Possible Preeclampsia As Health DeficitDocument3 pagesPossible Preeclampsia As Health DeficitCharisse BulasaNo ratings yet
- 21 CFR Part 864Document47 pages21 CFR Part 864luciano063No ratings yet
- Injury Classification and Lagging Indicators SidercaDocument14 pagesInjury Classification and Lagging Indicators SidercaEmilse QuirogaNo ratings yet
- Presentasion Vit KDocument18 pagesPresentasion Vit KAnancy Reza NgarbinganNo ratings yet
- Bcs Model Test 1Document19 pagesBcs Model Test 1IAMSANWAR019170No ratings yet
- Daftar PustakaDocument4 pagesDaftar Pustakachica_asNo ratings yet
- Standar Singkatan RSCMDocument54 pagesStandar Singkatan RSCMyannastiNo ratings yet
- Biogenic Silver Nanoparticles Synthesis Characterization and Its Potential Against Cancer Inducing Bacteria - 2016 - Journal of Molecular LiquidsDocument10 pagesBiogenic Silver Nanoparticles Synthesis Characterization and Its Potential Against Cancer Inducing Bacteria - 2016 - Journal of Molecular LiquidsCINDY VANESSA RESTREPO BURGOSNo ratings yet
- Hoerr NECAD 2018 PennSt Histopath Research DxFILEminimizer PDFDocument43 pagesHoerr NECAD 2018 PennSt Histopath Research DxFILEminimizer PDFamamùra maamarNo ratings yet
- Clsi La4 A4Document44 pagesClsi La4 A4Cristian Gutiérrez VeraNo ratings yet
- U N O R S L: Niversity of Egros Ccidental-Ecoletos Chool of AWDocument3 pagesU N O R S L: Niversity of Egros Ccidental-Ecoletos Chool of AWJanica DivinagraciaNo ratings yet
- Drugs and Substance AbuseDocument15 pagesDrugs and Substance AbuseEve Lexy MutituNo ratings yet
- Science Vi-Quarter 2 Module (Week 1-2 Nervous System)Document21 pagesScience Vi-Quarter 2 Module (Week 1-2 Nervous System)Denver TamayoNo ratings yet