0% found this document useful (0 votes)
163 views2 pagesMembership Application for SLAAPS
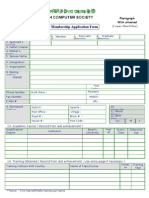
This document contains an application for membership to the Sri Lanka Association of Administrative & Professional Secretaries. The application requests personal details such as name, address, contact information, education history, employment details, and a declaration of truth. It specifies the annual subscription fees and required documents for the application, including a letter from the employer. Upon approval, the application will be certified by a recommending member and processed by the association's executive council and secretary.
Uploaded by
niroshini dadyCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
163 views2 pagesMembership Application for SLAAPS
This document contains an application for membership to the Sri Lanka Association of Administrative & Professional Secretaries. The application requests personal details such as name, address, contact information, education history, employment details, and a declaration of truth. It specifies the annual subscription fees and required documents for the application, including a letter from the employer. Upon approval, the application will be certified by a recommending member and processed by the association's executive council and secretary.
Uploaded by
niroshini dadyCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd