You might also like
- Glytrin Brand Plan 2016-17 FinalDocument54 pagesGlytrin Brand Plan 2016-17 FinalIndranil PoddarNo ratings yet
- J Clin Endocrinol Metab. 2012 97 16 38Document23 pagesJ Clin Endocrinol Metab. 2012 97 16 38rizwan234No ratings yet
- Co 2019 Controle Glicemico IntDocument8 pagesCo 2019 Controle Glicemico InthauhauNo ratings yet
- Assessment and Treatment of Hyperglycemia in Critically IllDocument6 pagesAssessment and Treatment of Hyperglycemia in Critically IllYousif ElmasryNo ratings yet
- Diabetes Case StudyDocument7 pagesDiabetes Case Studyapi-242589113No ratings yet
- Prediabetes dmt2 PDFDocument10 pagesPrediabetes dmt2 PDFARIA MINDNo ratings yet
- Desantis 2006Document15 pagesDesantis 2006Hoàng ThôngNo ratings yet
- 64 Ej16-0546Document8 pages64 Ej16-0546jzhongg91No ratings yet
- Zhou2019 Article InsulinDegludecANovelUltra-LonDocument18 pagesZhou2019 Article InsulinDegludecANovelUltra-LonmehakNo ratings yet
- 134 2021 Article 6526Document13 pages134 2021 Article 6526Eyal RobinsonNo ratings yet
- Ryzodeg PDFDocument9 pagesRyzodeg PDFWen Wei ChungNo ratings yet
- Laporan Pendahuluan MaxillaDocument10 pagesLaporan Pendahuluan MaxillaElim ChoNo ratings yet
- Ajuste Con Dosis PreviasDocument23 pagesAjuste Con Dosis PreviasOscar AlfonsoNo ratings yet
- Original Article: Nancy J. Wei, MD, MMSC David M. Nathan, MD Deborah J. Wexler, MD, MSCDocument8 pagesOriginal Article: Nancy J. Wei, MD, MMSC David M. Nathan, MD Deborah J. Wexler, MD, MSCAnggie AnggriyanaNo ratings yet
- Derosa 2010 InfDocument5 pagesDerosa 2010 InfJuan Carlos FloresNo ratings yet
- Poststroke Hyperglycemia: Natural History and Immediate ManagementDocument5 pagesPoststroke Hyperglycemia: Natural History and Immediate ManagementEsteban Martin Chiotti KaneshimaNo ratings yet
- Gracia Ramos2016Document8 pagesGracia Ramos2016Rahmanu ReztaputraNo ratings yet
- Translating The A1C Assay Into Estimated Average Glucose ValuesDocument6 pagesTranslating The A1C Assay Into Estimated Average Glucose ValuesFaryalBalochNo ratings yet
- Pilot Study of Using Neutral Protamine HDocument2 pagesPilot Study of Using Neutral Protamine HLili kartikaNo ratings yet
- Wang, Basal-Bolus Vs PremixedDocument10 pagesWang, Basal-Bolus Vs Premixedhasan andrianNo ratings yet
- Van Dijk, 2013Document6 pagesVan Dijk, 2013Gebyar CaturNo ratings yet
- Nej Mo A 1204942Document11 pagesNej Mo A 1204942Nandha PuspitaSariNo ratings yet
- Dia Care 1987 Feinglos 72 5Document4 pagesDia Care 1987 Feinglos 72 5Kang Opik TaufikNo ratings yet
- Diabetes Care Glucosa Promedio EstimadaDocument6 pagesDiabetes Care Glucosa Promedio EstimadaGemeneza GonzalesNo ratings yet
- Insulin Drip YALEDocument4 pagesInsulin Drip YALEnikeNo ratings yet
- Insulinoterapia: Luis Antonio Rodríguez. Fellow-Endocrinología Clínica y Metabolismo 2020Document106 pagesInsulinoterapia: Luis Antonio Rodríguez. Fellow-Endocrinología Clínica y Metabolismo 2020Carlos PerezNo ratings yet
- Impact of Pharmacist Insulin Management On Hemoglobin A1c in Outpatient Hospital Clinic SettingDocument7 pagesImpact of Pharmacist Insulin Management On Hemoglobin A1c in Outpatient Hospital Clinic SettingSabrina JonesNo ratings yet
- Hba1c VariabilityDocument5 pagesHba1c Variabilityruruh_wibowoNo ratings yet
- Indikasi Insulin InfusionDocument7 pagesIndikasi Insulin InfusionnikeNo ratings yet
- Content ServerDocument9 pagesContent ServerNourma Kusuma WinawanNo ratings yet
- PAMW 2014-04 - WrobelDocument7 pagesPAMW 2014-04 - WrobelDiana SamuezaNo ratings yet
- Marvin Et Al 2016 Minimization of Hypoglycemia As An Adverse Event During Insulin Infusion Further Refinement of TheDocument7 pagesMarvin Et Al 2016 Minimization of Hypoglycemia As An Adverse Event During Insulin Infusion Further Refinement of TheChanukya GvNo ratings yet
- Estudio NICE - Sugar (2009)Document11 pagesEstudio NICE - Sugar (2009)Trt CamargoNo ratings yet
- JHH 201654 ADocument11 pagesJHH 201654 ABarbara Sakura RiawanNo ratings yet
- Once-Weekly Insulin For Type 2 Diabetes Without Previous Insulin TreatmentDocument10 pagesOnce-Weekly Insulin For Type 2 Diabetes Without Previous Insulin TreatmentharvardboyNo ratings yet
- Jurnal 5Document4 pagesJurnal 5MFWPNo ratings yet
- Insulin Analogs Versus Human Insulin in The Treatment of Patients With Diabetic KetoacidosisDocument6 pagesInsulin Analogs Versus Human Insulin in The Treatment of Patients With Diabetic KetoacidosisrosieveliaNo ratings yet
- 193-Article Text-300-1-10-20180929Document4 pages193-Article Text-300-1-10-20180929asdfasdNo ratings yet
- J Cjca 2012 07 744Document2 pagesJ Cjca 2012 07 744khadesakshi55No ratings yet
- Semaglutide Added To Basal Insulin in Type 2 Diabetes (SUSTAIN 5) : A Randomized, Controlled TrialDocument11 pagesSemaglutide Added To Basal Insulin in Type 2 Diabetes (SUSTAIN 5) : A Randomized, Controlled TrialIvan Dario Hernandez ErazoNo ratings yet
- Medi 97 E11671Document8 pagesMedi 97 E11671Bilo BiloNo ratings yet
- 881 Full PDFDocument5 pages881 Full PDFrizki giofaniNo ratings yet
- Hyperglycemia After Cardiac Surgery - Hebson2013Document6 pagesHyperglycemia After Cardiac Surgery - Hebson2013Dr XNo ratings yet
- 881 Full PDFDocument5 pages881 Full PDFRizki GiofaniNo ratings yet
- Joi 160014Document10 pagesJoi 160014Rush32No ratings yet
- P ('t':'3', 'I':'3054456811') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Document4 pagesP ('t':'3', 'I':'3054456811') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)fraditayyunusNo ratings yet
- Weber 2016Document10 pagesWeber 2016Rafaela Queiroz MascarenhasNo ratings yet
- Garber 2007Document6 pagesGarber 2007Diana SamuezaNo ratings yet
- Dialysis Induced Hypoglycemia in Non-Diabetic Chronic Kidney Disease PatientsDocument3 pagesDialysis Induced Hypoglycemia in Non-Diabetic Chronic Kidney Disease Patientsscience worldNo ratings yet
- Cover Article: Standards of Medicai Care in Diabetes: Focus On Updated Recommendations in Hospitaiized PatientsDocument4 pagesCover Article: Standards of Medicai Care in Diabetes: Focus On Updated Recommendations in Hospitaiized Patientsapi-283746687No ratings yet
- Hyperglycemia and Neurological Outcome in Patients With Head InjuryDocument7 pagesHyperglycemia and Neurological Outcome in Patients With Head InjuryOsQ_drNo ratings yet
- 6 FullDocument8 pages6 FullAnonymous QPakSNNo ratings yet
- Efficacy and Safety of Biosimilar Glargine-IMGDocument8 pagesEfficacy and Safety of Biosimilar Glargine-IMGSiddiq MohammedNo ratings yet
- Effect of An Intensive Lifestyle Intervention On Glycemic Control in Patients With Type 2 Diabetes A Randomized Clinical TrialDocument10 pagesEffect of An Intensive Lifestyle Intervention On Glycemic Control in Patients With Type 2 Diabetes A Randomized Clinical TrialTanzo GremoryNo ratings yet
- CJN 08900722 Full-1Document15 pagesCJN 08900722 Full-1Ricardo IbarraNo ratings yet
- Continuous Insulin InfusionDocument6 pagesContinuous Insulin Infusionbobobo22No ratings yet
- Insulin Detemir and Basal Insulin TherapyDocument7 pagesInsulin Detemir and Basal Insulin Therapymayrapp16No ratings yet
- Khowaja2018 Article GlycemicControlInHospitalizedP PDFDocument9 pagesKhowaja2018 Article GlycemicControlInHospitalizedP PDFMade Dedy KusnawanNo ratings yet
- Premixed Insulin Analogue Compared With Basal-Plus Regimen For Inpatient Glycemic ControlDocument9 pagesPremixed Insulin Analogue Compared With Basal-Plus Regimen For Inpatient Glycemic ControlAbraham RamonNo ratings yet
- Association Between Stress Hyperglycemia and OutcomesDocument9 pagesAssociation Between Stress Hyperglycemia and OutcomesResiden Neuro FK UNPAD - RSHSNo ratings yet
- Hypoglycemic Encephalopathy A Case Series and Literature Review On Outcome DeterminationDocument7 pagesHypoglycemic Encephalopathy A Case Series and Literature Review On Outcome Determinationc5qdk8jnNo ratings yet
- Edelman2015 Article Nurse-LedBehavioralManagementODocument8 pagesEdelman2015 Article Nurse-LedBehavioralManagementOIndah SundariNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 18: PsychiatryFrom EverandComplementary and Alternative Medical Lab Testing Part 18: PsychiatryRating: 5 out of 5 stars5/5 (1)
- Analogos de Insulina, Farmacocinética y FarmacodinamiaDocument11 pagesAnalogos de Insulina, Farmacocinética y FarmacodinamiaAlin VázquezNo ratings yet
- CO-VANCE (Metformin + Glibenclamide) Product PresentationDocument25 pagesCO-VANCE (Metformin + Glibenclamide) Product Presentationashe64h74No ratings yet
- Šta Sve (Ne) Znamo O OAD: Prof - DR Dragana Tomić Naglić, Endokrinolog, UKC VojvodinaDocument50 pagesŠta Sve (Ne) Znamo O OAD: Prof - DR Dragana Tomić Naglić, Endokrinolog, UKC VojvodinaNaglic MiroslavNo ratings yet
- Blood Glucose Test Worksheet: Activity 4Document3 pagesBlood Glucose Test Worksheet: Activity 4Marcelle Ann C. VillanuevaNo ratings yet
- Prefi Assignment 2Document29 pagesPrefi Assignment 2Joanne Bernadette AguilarNo ratings yet
- Ertuglifozin DM IIDocument2 pagesErtuglifozin DM IIMr. LNo ratings yet
- Pathophysiology of Type II Diabetes MellitusDocument7 pagesPathophysiology of Type II Diabetes Mellituschinthaka18389021No ratings yet
- Severe Hypoglicemia: Is It Still A Threat For Children and Adolescent With Type 1 DiabetesDocument11 pagesSevere Hypoglicemia: Is It Still A Threat For Children and Adolescent With Type 1 DiabetesSultan Rahmat SeptianNo ratings yet
- 1068 5615 2 PBDocument8 pages1068 5615 2 PBVicky AndriNo ratings yet
- Creatinine Clearance: 58 Ml/min: Fasting Lipid ProfileDocument4 pagesCreatinine Clearance: 58 Ml/min: Fasting Lipid ProfileAnn DassNo ratings yet
- SingleResult 12Document3 pagesSingleResult 12abdallah ghunajuqNo ratings yet
- 79th American Diabetes Association Scientific Sessions - ADA Update 2019 PDFDocument44 pages79th American Diabetes Association Scientific Sessions - ADA Update 2019 PDFAmit BhondveNo ratings yet
- dm2 Non-InsulinDocument38 pagesdm2 Non-Insulinapi-649066372No ratings yet
- Activity 2.1.1 Student Response SheetDocument7 pagesActivity 2.1.1 Student Response SheetJose RamirezNo ratings yet
- Pengaruh Air Perasan Jahe Terhadap Kadar Glukosa Darah Dan Gambaran Histopatologi Sel Beta PankreasDocument9 pagesPengaruh Air Perasan Jahe Terhadap Kadar Glukosa Darah Dan Gambaran Histopatologi Sel Beta Pankreaslailatul rofiahNo ratings yet
- Diabetic Emergencies During Ramadan FastingDocument4 pagesDiabetic Emergencies During Ramadan FastingAmany SalamaNo ratings yet
- Insulin TherapyDocument23 pagesInsulin TherapyEliana MuisNo ratings yet
- Diabetes Flow ChartDocument8 pagesDiabetes Flow ChartNicky ChhajwaniNo ratings yet
- Bismillah Fix Hba1c1Document23 pagesBismillah Fix Hba1c1NsafifahNo ratings yet
- Carbohydrates: Dianne P. Jagonia, RMTDocument20 pagesCarbohydrates: Dianne P. Jagonia, RMTKristine Marie PateñoNo ratings yet
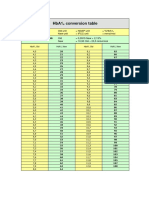
- HbA1cConversionTable PDFDocument1 pageHbA1cConversionTable PDFDarkoMaxNo ratings yet
- Management of Type 2 Diabetes During Ramadan: The Role of Gliclazide MRDocument25 pagesManagement of Type 2 Diabetes During Ramadan: The Role of Gliclazide MRMuhammad SugiartoNo ratings yet
- EmpagliflozinDocument2 pagesEmpagliflozinAusaf AhmadNo ratings yet
- Diabetes Melitus: Dr. Ihsanil Husna, SPPDDocument67 pagesDiabetes Melitus: Dr. Ihsanil Husna, SPPDnathan timothyNo ratings yet
- The 6 Stages of Diabetes Control & ReversalDocument7 pagesThe 6 Stages of Diabetes Control & ReversalHaleelu Abdul JaleelNo ratings yet
- Diabetic Ketoacidosis Triggered by Infection inDocument5 pagesDiabetic Ketoacidosis Triggered by Infection inpatricx10No ratings yet
- DMG 2022Document4 pagesDMG 2022Erika RosasNo ratings yet