You might also like
- Quality Control of Tablets Lecture 1Document15 pagesQuality Control of Tablets Lecture 1Muhammad AzeemNo ratings yet
- Effects of Leptin On The SkeletonDocument22 pagesEffects of Leptin On The SkeletonErika AvilaNo ratings yet
- Bonviva Is A HERO 2015Document36 pagesBonviva Is A HERO 2015drgayuhNo ratings yet
- Review Role of Oestrogen in The Regulation of Bone Turnover at The MenarcheDocument12 pagesReview Role of Oestrogen in The Regulation of Bone Turnover at The MenarcheSherly LudjiNo ratings yet
- Metabolism: The Importance of The Circadian System & Sleep For Bone HealthDocument16 pagesMetabolism: The Importance of The Circadian System & Sleep For Bone HealthAlonso FernandezNo ratings yet
- Assessing The Relationship BetweenDocument6 pagesAssessing The Relationship BetweenTri Eka JuliantoNo ratings yet
- 1 s2.0 S8756328217302302 MainDocument6 pages1 s2.0 S8756328217302302 Mainahmed fikryNo ratings yet
- Arth2011 580632Document6 pagesArth2011 580632hylee102594No ratings yet
- Comparison of Effectiveness and Safety of Ibandronate and Mi - 2017 - OsteoporosDocument8 pagesComparison of Effectiveness and Safety of Ibandronate and Mi - 2017 - OsteoporosDavid Ruiz GonzalezNo ratings yet
- (1479683X - European Journal of Endocrinology) Bone Turnover Marker Monitoring in Osteoporosis Treatment ResponseDocument3 pages(1479683X - European Journal of Endocrinology) Bone Turnover Marker Monitoring in Osteoporosis Treatment ResponseAlfred AlfredNo ratings yet
- Serum Leptin Levels Are Associated With Bone Mass in Nonobese WomenDocument4 pagesSerum Leptin Levels Are Associated With Bone Mass in Nonobese WomenTemtem HmNo ratings yet
- Las Trabeculas y La CalcificacionDocument9 pagesLas Trabeculas y La CalcificacionyatibaduizaNo ratings yet
- Gut Microbiota Induce IGF-1 and Promote Bone Formation and GrowthDocument10 pagesGut Microbiota Induce IGF-1 and Promote Bone Formation and GrowthValiio mazNo ratings yet
- Bone Mineral Density Progression Following Long-Term Simultaneous Pancreas-Kidney Transplantation in Type-1 DiabetesDocument6 pagesBone Mineral Density Progression Following Long-Term Simultaneous Pancreas-Kidney Transplantation in Type-1 Diabetesmiguel saba sabaNo ratings yet
- Relationship Between Bone-Specific Physical Activity Scores and Measures For Body Composition and Bone Mineral Density in Healthy Young College WomenDocument10 pagesRelationship Between Bone-Specific Physical Activity Scores and Measures For Body Composition and Bone Mineral Density in Healthy Young College WomenheryNo ratings yet
- Anchala Mahilange - jemds-ORADocument4 pagesAnchala Mahilange - jemds-ORAdrpklalNo ratings yet
- O Treinamento de Força Aumenta A Densidade Mineral Óssea Regional e A Remodelação Óssea em Homens de Meia-Idade e IdososDocument7 pagesO Treinamento de Força Aumenta A Densidade Mineral Óssea Regional e A Remodelação Óssea em Homens de Meia-Idade e IdososCarolina Drummond Rocha MoraisNo ratings yet
- La Densidad y La CalcificacionDocument9 pagesLa Densidad y La CalcificacionyatibaduizaNo ratings yet
- 10.1007@s10067 020 05150 ZDocument8 pages10.1007@s10067 020 05150 ZEriC. ChaN.No ratings yet
- Nandrolona Osteoporose RCTDocument6 pagesNandrolona Osteoporose RCTrodrigoNo ratings yet
- JBMR 3905Document10 pagesJBMR 3905Panagiotes KoutelidakesNo ratings yet
- Specker 2015 - Does Exercise Influence Pediatric Bone - A Systematic ReviewDocument15 pagesSpecker 2015 - Does Exercise Influence Pediatric Bone - A Systematic ReviewStavros LitsosNo ratings yet
- OP1 Maingrant ApplicationDocument6 pagesOP1 Maingrant Applicationmysticpixel94No ratings yet
- Iannitti Et Al., 2012 BPSDocument19 pagesIannitti Et Al., 2012 BPSTommaso IannittiNo ratings yet
- Regulatory Pathways Revealing New Approaches2008Document14 pagesRegulatory Pathways Revealing New Approaches2008Cami GutierrezNo ratings yet
- s00223 019 00581 6Document9 pagess00223 019 00581 6Dhruvi KansaraNo ratings yet
- Obsop Journal 1Document14 pagesObsop Journal 1Radditt GoberNo ratings yet
- Efectos A Largo Plazo de Anorexia y Baja Masa OseaDocument6 pagesEfectos A Largo Plazo de Anorexia y Baja Masa OsealeticiadelfinofotosNo ratings yet
- Dish - TbsDocument8 pagesDish - TbscarlosNo ratings yet
- Maturitas: SciencedirectDocument6 pagesMaturitas: Sciencedirectaeroforce20No ratings yet
- Nqab 264Document12 pagesNqab 264Luis Felipe Nascimento RodriguesNo ratings yet
- Alterations of Bone Microstructure and Strength in End-Stage Renal FailureDocument12 pagesAlterations of Bone Microstructure and Strength in End-Stage Renal FailureDany AGarciaNo ratings yet
- Bibliography Current World Literature: Geriatric Orthopaedics Management of OsteoporosisDocument10 pagesBibliography Current World Literature: Geriatric Orthopaedics Management of OsteoporosisLisa AdeliaNo ratings yet
- Orthopaedic Surgery - 2019 - Qu - Bone Turnover Markers and Bone Mineral Density To Predict Osteoporotic Fractures in OlderDocument8 pagesOrthopaedic Surgery - 2019 - Qu - Bone Turnover Markers and Bone Mineral Density To Predict Osteoporotic Fractures in OlderAlfred AlfredNo ratings yet
- Importancia Del Pico de Masa Osea Bonjour 2009Document13 pagesImportancia Del Pico de Masa Osea Bonjour 2009leticiadelfinofotosNo ratings yet
- 2014 - Augmentation of Tendon-to-Bone HealingDocument9 pages2014 - Augmentation of Tendon-to-Bone HealingBeatriz Pinhal MarquesNo ratings yet
- Relation Between Obesity and Bone Mineral Density and Vertebral Fractures in Korean Postmenopausal WomenDocument7 pagesRelation Between Obesity and Bone Mineral Density and Vertebral Fractures in Korean Postmenopausal WomenMaverick 18No ratings yet
- Stubbs 2014Document17 pagesStubbs 2014sajith4457No ratings yet
- Bone Turnover Rate and Bone Formation Resorption Balance Durin - 2017 - OsteoporDocument8 pagesBone Turnover Rate and Bone Formation Resorption Balance Durin - 2017 - OsteoporDavid Ruiz GonzalezNo ratings yet
- 1 s2.0 S8756328205002589 MainDocument9 pages1 s2.0 S8756328205002589 MainPoramate PITAK-ARNNOPNo ratings yet
- Bone Tissue EngineeringDocument9 pagesBone Tissue EngineeringKevinNo ratings yet
- The Role of Circulating Bone Cell Precursors in Fracture HealingDocument8 pagesThe Role of Circulating Bone Cell Precursors in Fracture HealinghanifahsaNo ratings yet
- "Nutraceuticals" in Relation To Human Skeletal Muscle and ExerciseDocument18 pages"Nutraceuticals" in Relation To Human Skeletal Muscle and ExerciseErnestoNo ratings yet
- Agastache Rugosa Ethanol Extract Suppresses Bone Loss Via Induction of - CompressedDocument9 pagesAgastache Rugosa Ethanol Extract Suppresses Bone Loss Via Induction of - Compressedela.sofiaNo ratings yet
- JJBMRDocument9 pagesJJBMRDeby AnditaNo ratings yet
- Change of Hyoid Bone Position in Patients TreatedDocument18 pagesChange of Hyoid Bone Position in Patients TreatedYesenia PaisNo ratings yet
- Effect of Physical Therapy On Bone Remodelling in Preterm Infants: A Multicenter Randomized Controlled Clinical TrialDocument13 pagesEffect of Physical Therapy On Bone Remodelling in Preterm Infants: A Multicenter Randomized Controlled Clinical TrialAroa BermudezNo ratings yet
- Resistance Ex Bone TurnoverDocument7 pagesResistance Ex Bone TurnoverHari25885No ratings yet
- (15432742 - International Journal of Sport Nutrition and Exercise Metabolism) Making Sense of Muscle Protein Synthesis A Focus On Muscle GrowDocument13 pages(15432742 - International Journal of Sport Nutrition and Exercise Metabolism) Making Sense of Muscle Protein Synthesis A Focus On Muscle GrowjepoNo ratings yet
- Botox Issues ReferenceList Pacesetter April 2020Document16 pagesBotox Issues ReferenceList Pacesetter April 2020Amr Mohamed GalalNo ratings yet
- Osteoprogenitor Enviar A Angie ArelisDocument22 pagesOsteoprogenitor Enviar A Angie ArelisAngie ColonNo ratings yet
- Nutrition and Osteoporosis: V.E. Bianchi, L.J. Dominguez, M. BarbagalloDocument10 pagesNutrition and Osteoporosis: V.E. Bianchi, L.J. Dominguez, M. BarbagalloMartha SimonaNo ratings yet
- Biology TMJ 2013Document8 pagesBiology TMJ 2013Nidia TorreaNo ratings yet
- 2022 Article 16231Document7 pages2022 Article 16231Ana Carolina SouzaNo ratings yet
- Effect of Intravenous Pamidronate Treatment in Children With Osteogenesis ImperfectaDocument5 pagesEffect of Intravenous Pamidronate Treatment in Children With Osteogenesis Imperfectavikash singhNo ratings yet
- Sex Steroids and Bone: Current Perspectives: Juan BalaschDocument16 pagesSex Steroids and Bone: Current Perspectives: Juan Balaschrajeshraju2002No ratings yet
- Blood Cells, Molecules and DiseasesDocument4 pagesBlood Cells, Molecules and DiseasesDavide MalheiroNo ratings yet
- Whole BVDocument14 pagesWhole BVAdrian StanNo ratings yet
- Treatment of Postmenopausal OsteoporosisDocument8 pagesTreatment of Postmenopausal OsteoporosisLaura_Puspita__9294No ratings yet
- Does Obesity Protect Postmenopausal Women Against Osteoporosis?Document10 pagesDoes Obesity Protect Postmenopausal Women Against Osteoporosis?Indah MaulidawatiNo ratings yet
- Pharmacy: Irrational Use of Medicines-A Summary of Key ConceptsDocument13 pagesPharmacy: Irrational Use of Medicines-A Summary of Key ConceptsEndah susantiNo ratings yet
- Project 2 Nathan ChaulkDocument17 pagesProject 2 Nathan Chaulkapi-535482465No ratings yet
- Unit I. Introduction Into Pharmacology. Pharmacy Branches Discussion PointsDocument14 pagesUnit I. Introduction Into Pharmacology. Pharmacy Branches Discussion PointsAlina TacuNo ratings yet
- RSSL Training Good Distribution PracticeDocument1 pageRSSL Training Good Distribution PracticeCeangoNo ratings yet
- Colchicine - General DataDocument3 pagesColchicine - General DataCatalina BanuNo ratings yet
- Products Medicine WarehouseDocument54 pagesProducts Medicine WarehouseksdmksdmNo ratings yet
- Module 3-5 I PmqaDocument11 pagesModule 3-5 I Pmqa11Lag2Carisma II, Jose P.No ratings yet
- PONV Guidelines Update 110110Document3 pagesPONV Guidelines Update 110110Fauzan Luthfi A MNo ratings yet
- Pharmacognosy: 1. GPAT Discussion CenterDocument9 pagesPharmacognosy: 1. GPAT Discussion CenterMustakim PatelNo ratings yet
- Pharmaceutical Sector of Bangladesh: Prospects and ChallengesDocument46 pagesPharmaceutical Sector of Bangladesh: Prospects and ChallengesRifat Ibna LokmanNo ratings yet
- AP PGECET Pharmacy Syllabus and Exam PatternDocument3 pagesAP PGECET Pharmacy Syllabus and Exam PatternpavaniNo ratings yet
- Antibiotics in Oral & Maxillofacial SurgeryDocument50 pagesAntibiotics in Oral & Maxillofacial SurgerysevattapillaiNo ratings yet
- NYPD Payroll List.Document7,411 pagesNYPD Payroll List.CabinCr3wNo ratings yet
- Kodak PlanDocument48 pagesKodak PlanSean Mickey100% (2)
- IV Med AdminDocument4 pagesIV Med AdminMa. Ferimi Gleam BajadoNo ratings yet
- Pharmacy Informatics (PDFDrive)Document114 pagesPharmacy Informatics (PDFDrive)Sydney Edelweiss MadridNo ratings yet
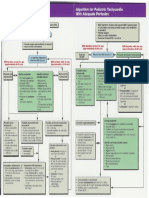
- Pediatric Tachycardia AlgorithmsDocument1 pagePediatric Tachycardia AlgorithmsGalih FatoniNo ratings yet
- 18.jaladi Himaja Battu Rakesh PDFDocument9 pages18.jaladi Himaja Battu Rakesh PDFFebby da costaNo ratings yet
- International Journal of Advances in Pharmaceutical AnalysisDocument7 pagesInternational Journal of Advances in Pharmaceutical Analysisayu febrianiNo ratings yet
- Date Year Hs Code Product QuantityunitDocument45 pagesDate Year Hs Code Product QuantityunitProschool HyderabadNo ratings yet
- Mcneil Consumer Healthcare CompanyDocument6 pagesMcneil Consumer Healthcare CompanyJennifer JohnsonNo ratings yet
- 7.0 InterchangibilityDocument2 pages7.0 InterchangibilitySanket ChintawarNo ratings yet
- Infectious DiseaseaDocument22 pagesInfectious DiseaseasamNo ratings yet
- Basic Clinical Pharmacology 14Th Edition Bertram G Katzung 2 Full ChapterDocument67 pagesBasic Clinical Pharmacology 14Th Edition Bertram G Katzung 2 Full Chapterjames.rutz213100% (6)
- Determination of Ibuprofen and Paraben in Pharmaceutical Formulations Using Flowinjection and Derivative SpectrophotometryDocument2 pagesDetermination of Ibuprofen and Paraben in Pharmaceutical Formulations Using Flowinjection and Derivative Spectrophotometrycamelia_ioana_14No ratings yet
- Barangay Monthly Inventory of Vaccinated PopulationDocument14 pagesBarangay Monthly Inventory of Vaccinated PopulationLaceth Joyce T. LASATNo ratings yet
- 3 Week Review StudyPlanDocument2 pages3 Week Review StudyPlanSNo ratings yet
- N-Methylation of Peptides A New Perspective in Medicinal ChemistryDocument12 pagesN-Methylation of Peptides A New Perspective in Medicinal Chemistryrawal.ravindraNo ratings yet