You might also like
- Annals of General PsychiatryDocument9 pagesAnnals of General PsychiatryPutu Agus GrantikaNo ratings yet
- Finding the Path in Alzheimer’s Disease: Early Diagnosis to Ongoing Collaborative CareFrom EverandFinding the Path in Alzheimer’s Disease: Early Diagnosis to Ongoing Collaborative CareNo ratings yet
- Incidence, Causes, and Consequences of Preventable Adverse Drug Reactions Occurring in Inpatients - A Systematic Review of Systematic Reviews - PMCDocument39 pagesIncidence, Causes, and Consequences of Preventable Adverse Drug Reactions Occurring in Inpatients - A Systematic Review of Systematic Reviews - PMCimyours9601No ratings yet
- Information Needs and Sources of Information Among People With Depression and Anxiety: A Scoping ReviewDocument18 pagesInformation Needs and Sources of Information Among People With Depression and Anxiety: A Scoping ReviewVince MartinezNo ratings yet
- Neurologist Communicationg The Diagnosis of ELADocument9 pagesNeurologist Communicationg The Diagnosis of ELAHabib G. Moutran BarrosoNo ratings yet
- The Massachusetts General Hospital Guide to Depression: New Treatment Insights and OptionsFrom EverandThe Massachusetts General Hospital Guide to Depression: New Treatment Insights and OptionsBenjamin G. ShaperoNo ratings yet
- Evaluation of Depression and Suicidal Patients in The Emergency RoomDocument15 pagesEvaluation of Depression and Suicidal Patients in The Emergency RoomjuanpbagurNo ratings yet
- Pharmacy: Ingestible Sensors and Medication Adherence: Focus On Use in Serious Mental IllnessDocument11 pagesPharmacy: Ingestible Sensors and Medication Adherence: Focus On Use in Serious Mental IllnessArif IrpanNo ratings yet
- Determinants and Prevalence of Relapse Among Patients With Substance Use Disorders: Case of Icyizere Psychotherapeutic CentreDocument12 pagesDeterminants and Prevalence of Relapse Among Patients With Substance Use Disorders: Case of Icyizere Psychotherapeutic CentreArif IrpanNo ratings yet
- Brightside BMC ArticleDocument10 pagesBrightside BMC ArticlePsydocNo ratings yet
- Apnea Obstructiva Del Sueño y DepresiónDocument9 pagesApnea Obstructiva Del Sueño y DepresiónVALENTIN MARTINEZ-OTERO PEREZNo ratings yet
- Relationship Between Health Literacy Scores and Patient Use of the iPET for Patient EducationFrom EverandRelationship Between Health Literacy Scores and Patient Use of the iPET for Patient EducationNo ratings yet
- Prevalence and Factors Associated With Depression Among Medical Students in Cameroon: A Cross-Sectional StudyDocument7 pagesPrevalence and Factors Associated With Depression Among Medical Students in Cameroon: A Cross-Sectional StudywatiNo ratings yet
- IkhsanDocument14 pagesIkhsanSilvia Icha RiskiNo ratings yet
- Comorbidity Study of Borderline Personality Disorder: Applying Association Rule Mining To The Taiwan National Health Insurance Research DatabaseDocument10 pagesComorbidity Study of Borderline Personality Disorder: Applying Association Rule Mining To The Taiwan National Health Insurance Research DatabaseGheorghe SecuNo ratings yet
- Pharmacoepidemiology and Pharmacovigilance: Synergistic Tools to Better Investigate Drug SafetyFrom EverandPharmacoepidemiology and Pharmacovigilance: Synergistic Tools to Better Investigate Drug SafetyRating: 4.5 out of 5 stars4.5/5 (3)
- 2 Effects of A Pharmaceutical Care Intervention Coronary Heart DiseaseDocument16 pages2 Effects of A Pharmaceutical Care Intervention Coronary Heart DiseaseRosalinda Marquez VegaNo ratings yet
- 2014 Article 5105Document26 pages2014 Article 5105Billy Ch SendukNo ratings yet
- Treating Opioid Use Disorder in General Medical SettingsFrom EverandTreating Opioid Use Disorder in General Medical SettingsSarah E. WakemanNo ratings yet
- Artículo Evidencia de Recaídas (Hardelveld)Document8 pagesArtículo Evidencia de Recaídas (Hardelveld)María CastilloNo ratings yet
- GMHAT - Cardiac Patients Reino UnidoDocument7 pagesGMHAT - Cardiac Patients Reino UnidoIleana AjaNo ratings yet
- Prevalence of Depression and Anxiety in SLE PDFDocument14 pagesPrevalence of Depression and Anxiety in SLE PDFRidho PratamaNo ratings yet
- 1. 1 Trinidad y Tobago 2023Document11 pages1. 1 Trinidad y Tobago 2023WENDY PHRITSILA PEÑA TICONANo ratings yet
- NannsDocument9 pagesNannsal jaynNo ratings yet
- Cost-of-illness studies: Measuring healthcare costs fact vs fictionDocument2 pagesCost-of-illness studies: Measuring healthcare costs fact vs fictionIoana AntonesiNo ratings yet
- Assessing What Matters Most To Patients With or atDocument16 pagesAssessing What Matters Most To Patients With or atandreamandu25No ratings yet
- Theory Introduction PaperDocument6 pagesTheory Introduction Paperapi-530825663No ratings yet
- Safety of Psychotropic Medications in People With COVID-19: Evidence Review and Practical RecommendationsDocument14 pagesSafety of Psychotropic Medications in People With COVID-19: Evidence Review and Practical Recommendationsracm89No ratings yet
- Direct Costs of Parkinson's Disease in Brazil: A Case StudyDocument8 pagesDirect Costs of Parkinson's Disease in Brazil: A Case StudyIJAERS JOURNALNo ratings yet
- Revised Olu-ELR Does Patient Engagement Impact Relapse Outcomes - EditedDocument43 pagesRevised Olu-ELR Does Patient Engagement Impact Relapse Outcomes - Editedsamir morogaNo ratings yet
- Fenton (2012) - The Cost of Satisfaction - A National Study of Patient Satisfaction, Health Care Utilization, Expenditures, and MortalityDocument7 pagesFenton (2012) - The Cost of Satisfaction - A National Study of Patient Satisfaction, Health Care Utilization, Expenditures, and Mortalityghcabsb87No ratings yet
- Research Paper On Dual DiagnosisDocument6 pagesResearch Paper On Dual Diagnosisyfwkdbaod100% (1)
- 2020 05 23 20110841v1 FullDocument29 pages2020 05 23 20110841v1 FullAjeng baskoroNo ratings yet
- A Randomized Trial of Telemedicine-Based Collaborative Care For DepressionDocument9 pagesA Randomized Trial of Telemedicine-Based Collaborative Care For DepressionMoira P. ShawNo ratings yet
- The Opioid Epidemic and the Therapeutic Community Model: An Essential GuideFrom EverandThe Opioid Epidemic and the Therapeutic Community Model: An Essential GuideJonathan D. AveryNo ratings yet
- Journal Pre-Proofs: Brain, Behavior, and ImmunityDocument26 pagesJournal Pre-Proofs: Brain, Behavior, and ImmunitycoconitaNo ratings yet
- Physician Stress and Burnout: The Impact of Health Information TechnologyDocument9 pagesPhysician Stress and Burnout: The Impact of Health Information TechnologyAgam MaldiniNo ratings yet
- Exercise Interventions For The Prevention of DepreDocument12 pagesExercise Interventions For The Prevention of DeprefitrianiNo ratings yet
- 1 s2.0 S016383431830433X AmDocument26 pages1 s2.0 S016383431830433X AmmorganitarawriterNo ratings yet
- Journal Review Final PaperDocument10 pagesJournal Review Final Paperapi-464793486No ratings yet
- Surviving Cancer, COVID-19, and Disease: The Repurposed Drug RevolutionFrom EverandSurviving Cancer, COVID-19, and Disease: The Repurposed Drug RevolutionNo ratings yet
- Content ServerDocument11 pagesContent ServerALONDRA FERNANDA RODRIGUEZ HERRERANo ratings yet
- Research ArticleDocument9 pagesResearch ArticleShannon GonsalvesNo ratings yet
- Farmacos en AncianosDocument12 pagesFarmacos en AncianosKarina Alexandra Vera-Pinto EstacioNo ratings yet
- Efficacy, Acceptability, and Safety of Antidepressants For Low Back Pain: A Systematic Review and Meta-AnalysisDocument13 pagesEfficacy, Acceptability, and Safety of Antidepressants For Low Back Pain: A Systematic Review and Meta-Analysisskola onlajnNo ratings yet
- Comparision by Gender COVID19 ReviewDocument9 pagesComparision by Gender COVID19 ReviewMitchel Cordova LoaizaNo ratings yet
- Prevalence of Depression, Anxiety, and Adjustment Disorder in Oncological, Haematological, and Palliative-Care Settings: A Meta-Analysis of 94 Interview-Based StudiesDocument16 pagesPrevalence of Depression, Anxiety, and Adjustment Disorder in Oncological, Haematological, and Palliative-Care Settings: A Meta-Analysis of 94 Interview-Based StudiesClaudia EvelineNo ratings yet
- Prescription Opioid Use Among Adults With Mental Health Disorders in The United StatesDocument11 pagesPrescription Opioid Use Among Adults With Mental Health Disorders in The United StatesAnanda WulandariNo ratings yet
- Patient Education and CounselingDocument5 pagesPatient Education and CounselingQianqian FanNo ratings yet
- Effects of The Tailored Activity ProgramDocument14 pagesEffects of The Tailored Activity ProgramBarbara Aguilar MaulenNo ratings yet
- Antidepressants and Health-Related Quality of Life For Patients With DepressionDocument14 pagesAntidepressants and Health-Related Quality of Life For Patients With Depressionjohndoe691488No ratings yet
- Post Stroke DepresiDocument9 pagesPost Stroke DepresiSitti Rosdiana YahyaNo ratings yet
- Cancer - 2018 - Nathan - Adverse Mental Health Outcomes in A Population Based Cohort of Survivors of Childhood CancerDocument13 pagesCancer - 2018 - Nathan - Adverse Mental Health Outcomes in A Population Based Cohort of Survivors of Childhood CancerJuliana SoaresNo ratings yet
- Managing Health in the Genomic Era: A Guide to Family Health History and Disease RiskFrom EverandManaging Health in the Genomic Era: A Guide to Family Health History and Disease RiskNo ratings yet
- Brasil, Campeão Mundial de DepressãoDocument16 pagesBrasil, Campeão Mundial de DepressãoValéria AlmeidaNo ratings yet
- 2011 Detection of Depression and Anxiety Disorders in Primary Care Friendly)Document9 pages2011 Detection of Depression and Anxiety Disorders in Primary Care Friendly)rocksurNo ratings yet
- Kupeli2019 Article ExpressiveWritingAsATherapeuti PDFDocument12 pagesKupeli2019 Article ExpressiveWritingAsATherapeuti PDFHimmatul LuthfiyahNo ratings yet
- Blood Transfusion Therapy DefinitionDocument27 pagesBlood Transfusion Therapy DefinitionEvangelin MelvinNo ratings yet
- Lung Cancer (Nursing Care)Document5 pagesLung Cancer (Nursing Care)heiyuNo ratings yet
- Heydriontad Ervoxereniot Dehydration Overexertion Hyperthermia Sweating ThirstDocument36 pagesHeydriontad Ervoxereniot Dehydration Overexertion Hyperthermia Sweating ThirstMaica Canete100% (1)
- Ebook PDF Colorectal Surgery A Companion To Specialist Surgical Practice 6th Edition PDFDocument41 pagesEbook PDF Colorectal Surgery A Companion To Specialist Surgical Practice 6th Edition PDFrobert.gonzales146100% (37)
- Clinical Manifestations of Complicated Malaria - An OverviewDocument9 pagesClinical Manifestations of Complicated Malaria - An OverviewArja' WaasNo ratings yet
- ECMO (Extracorporeal Membrane Oxygenation)Document22 pagesECMO (Extracorporeal Membrane Oxygenation)dhivya singhNo ratings yet
- NCP Ineffective Airway ClearanceDocument2 pagesNCP Ineffective Airway Clearanceniomi0884% (31)
- X-Ray Findings and Key Signs in RadiologyDocument3 pagesX-Ray Findings and Key Signs in RadiologylilyNo ratings yet
- Edukasi Kesehatan di Bulan RamadhanDocument10 pagesEdukasi Kesehatan di Bulan RamadhanDiki MulyadiNo ratings yet
- Impaired Physical MobilityDocument3 pagesImpaired Physical MobilityCalimlim Kim100% (1)
- Managing Hemophilia Care ComprehensivelyDocument33 pagesManaging Hemophilia Care ComprehensivelyZuna QaziNo ratings yet
- Prepared by Honorable GAKWAYA: Gram NegativeDocument19 pagesPrepared by Honorable GAKWAYA: Gram NegativeNyakubahwa HonoreNo ratings yet
- Preoperative PreparationDocument22 pagesPreoperative Preparationjackyploes100% (1)
- Central University of Kerala: Covid-19 Test ReportDocument2 pagesCentral University of Kerala: Covid-19 Test ReportJackson p georgeNo ratings yet
- Outpatient ResumeDocument1 pageOutpatient ResumeAbdul GamalNo ratings yet
- Glioblastoma: in This Fact SheetDocument17 pagesGlioblastoma: in This Fact SheetSunil GvalaniNo ratings yet
- Zyprexa 020592 S 063,021086 S 041 LBLDocument5 pagesZyprexa 020592 S 063,021086 S 041 LBLbonjovicamoiNo ratings yet
- Vertigo: Causes, Symptoms and TreatmentDocument3 pagesVertigo: Causes, Symptoms and TreatmentJemsner IrothNo ratings yet
- Benign and Malignant Cervical LesionsDocument46 pagesBenign and Malignant Cervical LesionsRohitNo ratings yet
- TranslateDocument8 pagesTranslateberliananastasya pNo ratings yet
- Nexcare - Drug StudyDocument2 pagesNexcare - Drug StudyrufinodanicaNo ratings yet
- Clinical-Professional-Reasoning-Exam UON 2017Document17 pagesClinical-Professional-Reasoning-Exam UON 2017nathanNo ratings yet
- Research Secondary HypertensionDocument51 pagesResearch Secondary HypertensionDomeng TalksNo ratings yet
- Mental Retardation, Giftedness, and EBDDocument127 pagesMental Retardation, Giftedness, and EBDLikhaan PerformingArts HomeStudioNo ratings yet
- Social Anxiety Disorder: Understanding SADDocument7 pagesSocial Anxiety Disorder: Understanding SADAntonia Milena LambaNo ratings yet
- Cholangiocarcinoma - A Review of The Literature and Future Directions in Therapy - HB SurgicalDocument12 pagesCholangiocarcinoma - A Review of The Literature and Future Directions in Therapy - HB SurgicalAnna MariaNo ratings yet
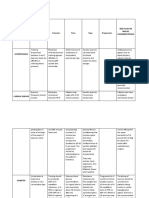
- Medical Conditions Frequency Intensity Time Type Progression Red Flags or Special ConsideratrionsDocument4 pagesMedical Conditions Frequency Intensity Time Type Progression Red Flags or Special ConsideratrionsClaire Madriaga GidoNo ratings yet
- Rabies PreventionDocument3 pagesRabies PreventionFrinkaWijaya100% (1)
- BOTOXDocument12 pagesBOTOXJanani KrishnanNo ratings yet
- Parmed X PDFDocument4 pagesParmed X PDFIoannis AmanatidisNo ratings yet