You might also like
- (ASRA) Guidelines Neuraxial and AnticoagulationDocument6 pages(ASRA) Guidelines Neuraxial and Anticoagulationfraditayyunus82% (11)
- Journal Club TemplateDocument5 pagesJournal Club TemplateAnonymous zyHbTsybDXNo ratings yet
- Drug Study Heparin and FenylDocument4 pagesDrug Study Heparin and FenylAnisa Jamito67% (3)
- Stop Anticoagulation Neuraxial AnesthesiaDocument3 pagesStop Anticoagulation Neuraxial AnesthesiaGihan NakhlehNo ratings yet
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingFrom EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNo ratings yet
- Management of Antithrombotic Therapy For Neuraxial and Peripheral Nerve ProceduresDocument3 pagesManagement of Antithrombotic Therapy For Neuraxial and Peripheral Nerve Proceduresjojobod100% (1)
- SOPProningNonIntubated PatientFinal - 05182020 PDFDocument12 pagesSOPProningNonIntubated PatientFinal - 05182020 PDFzaenab anissaNo ratings yet
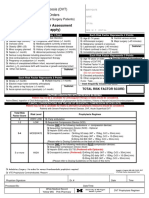
- Thrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersDocument2 pagesThrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersPutu Gizha Satrya GautamaNo ratings yet
- Anticoagulants Preoperative InstructionsDocument3 pagesAnticoagulants Preoperative InstructionsDevaki VisvalingamNo ratings yet
- Document PDFDocument4 pagesDocument PDFDebasis SahooNo ratings yet
- VTE Form - Surgical & Medical PatientsDocument2 pagesVTE Form - Surgical & Medical PatientsNatasha BhasinNo ratings yet
- SISS - Evaluation of Pediatric Abdominal Pain and ImagingDocument4 pagesSISS - Evaluation of Pediatric Abdominal Pain and ImagingPrincyNo ratings yet
- Clinical Pathway StrokeDocument8 pagesClinical Pathway StrokedjizhieeNo ratings yet
- VTE Prophylaxis GuidelinesDocument1 pageVTE Prophylaxis GuidelinesSylvia Ruth Alisa Nababan100% (1)
- Anae15291 Sup 0001 Appendixs1Document10 pagesAnae15291 Sup 0001 Appendixs1iamseraNo ratings yet
- Ricoagulazione PZ Per ALRDocument2 pagesRicoagulazione PZ Per ALRAgnese ValentiniNo ratings yet
- Anticoagulation in Presence of Neuraxial Anesthesia (Guidelines Do Not Apply To Peripheral NerveDocument3 pagesAnticoagulation in Presence of Neuraxial Anesthesia (Guidelines Do Not Apply To Peripheral NerveShoyeb KhanNo ratings yet
- 5 Pre Op CS & Major Surgery 22.06.2015Document5 pages5 Pre Op CS & Major Surgery 22.06.2015Mahesh RathnayakeNo ratings yet
- VTE Form - Surgical & Medical PatientsDocument2 pagesVTE Form - Surgical & Medical PatientsNatasha BhasinNo ratings yet
- Antithrombotics and Neuraxial Anesthesia GuidelineDocument6 pagesAntithrombotics and Neuraxial Anesthesia Guidelinelokeswara reddyNo ratings yet
- 134 2021 6401 Moesm1 EsmDocument16 pages134 2021 6401 Moesm1 Esmnina2911No ratings yet
- MR 4 AprilDocument11 pagesMR 4 AprilAriella maydenNo ratings yet
- Central Neuraxial and Nerve Blocks in Presence of Anticoagulants and AntiplateletsDocument42 pagesCentral Neuraxial and Nerve Blocks in Presence of Anticoagulants and AntiplateletsGaurav DeshmukhNo ratings yet
- VTE - Prophylaxis - PROTOCOL - V1.1 - With Forms - 07 - Dec - 2023Document20 pagesVTE - Prophylaxis - PROTOCOL - V1.1 - With Forms - 07 - Dec - 2023hatem newishyNo ratings yet
- Anticoagulantele Si Explorarile Invazive 2021Document33 pagesAnticoagulantele Si Explorarile Invazive 2021GabrielaOaneNo ratings yet
- Perioperative Management of AnticoagulationDocument33 pagesPerioperative Management of Anticoagulationmonge20No ratings yet
- Most of Cardiac Care Unit (C.C.U) DrugsDocument57 pagesMost of Cardiac Care Unit (C.C.U) DrugsOsama OmarNo ratings yet
- Perioperative Anticoagulation Bridging Guideline PostedDocument6 pagesPerioperative Anticoagulation Bridging Guideline PostedNuc Alexandru100% (1)
- VTE Prophylaxis PROTOCOL V1.2 Withforms 31 Dec 2023Document19 pagesVTE Prophylaxis PROTOCOL V1.2 Withforms 31 Dec 2023hatem newishyNo ratings yet
- Anticoagulatio N Asra Guidelines: Sravya VemuriDocument62 pagesAnticoagulatio N Asra Guidelines: Sravya VemuriSiva Prasad AspNo ratings yet
- Central Neuraxial & Plexus Block in Presence of Anticoagulant & Antiplatelet MedicationDocument41 pagesCentral Neuraxial & Plexus Block in Presence of Anticoagulant & Antiplatelet MedicationIndrani HemantkumarNo ratings yet
- STEMI Thrombolysis Protocol STElevation MIDocument6 pagesSTEMI Thrombolysis Protocol STElevation MISurya AtmajaNo ratings yet
- Practice Guidelines For Juniors 01 June 2016Document3 pagesPractice Guidelines For Juniors 01 June 2016ElaineNo ratings yet
- Tambahan EnglishDocument16 pagesTambahan EnglishHotman Raja GukgukNo ratings yet
- Stroke Guidelines: Cva Critical Pathway Department of NeurologyDocument5 pagesStroke Guidelines: Cva Critical Pathway Department of NeurologyplethoraldorkNo ratings yet
- Diagnostic Angiography SOPDocument2 pagesDiagnostic Angiography SOPQuality Assurance DepartmentNo ratings yet
- ASRA Guidelines For CNBDocument66 pagesASRA Guidelines For CNBAshiyan IrfanNo ratings yet
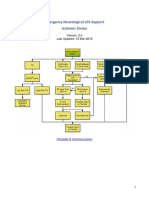
- Emergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Document22 pagesEmergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Aik NoeraNo ratings yet
- Bridging For Patients On DOACs/NOACsDocument1 pageBridging For Patients On DOACs/NOACsZieshNo ratings yet
- ALS Practical Assessment Tool 2018Document5 pagesALS Practical Assessment Tool 2018MorganeNo ratings yet
- Medical Surgical ATI Review Flashcards - QuizletDocument27 pagesMedical Surgical ATI Review Flashcards - QuizletNursyNurseNo ratings yet
- Enls V 3.0 Protocol Ais Final 0418Document25 pagesEnls V 3.0 Protocol Ais Final 0418Caleb LinNo ratings yet
- Expanding The Therapeutic Window For Acute Ischemic Stroke:: New Agents, New ApproachesDocument29 pagesExpanding The Therapeutic Window For Acute Ischemic Stroke:: New Agents, New ApproachesDr. RajibNo ratings yet
- تقيم الجلطات الوريدية للكبارDocument2 pagesتقيم الجلطات الوريدية للكبارAhmed Mohammed SalamaNo ratings yet
- PREOPinguinalherniaDocument2 pagesPREOPinguinalherniapatriciaatan1497No ratings yet
- EHRA Practical Guide On The Use of New Oral Anticoagulants in Patients With Non-Valvular Atrial FibrillationDocument41 pagesEHRA Practical Guide On The Use of New Oral Anticoagulants in Patients With Non-Valvular Atrial FibrillationAmelia Maria LasloNo ratings yet
- 443e Technique of Lumbar PunctureDocument4 pages443e Technique of Lumbar PunctureEXB GensanNo ratings yet
- UCSF Antithrombotics Neuraxia Lnterventions Guideline Version4Document5 pagesUCSF Antithrombotics Neuraxia Lnterventions Guideline Version4Olguita Huaccha PastorNo ratings yet
- Recruitment Checklist: Security Forces Hospital ProgramDocument4 pagesRecruitment Checklist: Security Forces Hospital ProgramDerick RanaNo ratings yet
- SBH/HSC Pre-Angiogram/ Angioplasty/Stent ChecklistDocument2 pagesSBH/HSC Pre-Angiogram/ Angioplasty/Stent ChecklistKena Ben100% (2)
- Critical Care Admission OrdersDocument6 pagesCritical Care Admission OrdersTariq Niaz Ahmad, MDNo ratings yet
- NEURO2 1.02C Hemorrhagic Stroke - Dr. HiyadanDocument2 pagesNEURO2 1.02C Hemorrhagic Stroke - Dr. HiyadanAra Diocos100% (1)
- DCR and Dcs DSTCDocument52 pagesDCR and Dcs DSTCGustafPandyHattaNo ratings yet
- Clinical Pathway - Stroke Without Thrombolytic TherapyDocument4 pagesClinical Pathway - Stroke Without Thrombolytic TherapysiusiuwidyantoNo ratings yet
- Neuraxial Analgesia & Anticoagulation: Charles E Smith MDDocument53 pagesNeuraxial Analgesia & Anticoagulation: Charles E Smith MDPraveen RamasamyNo ratings yet
- Ventura County Medical Center: Mi Thrombolysis, Management ofDocument3 pagesVentura County Medical Center: Mi Thrombolysis, Management ofblackcat657No ratings yet
- Anticoagulation Protocol For PostDocument8 pagesAnticoagulation Protocol For PostMohammed IbrahimNo ratings yet
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModeJelena Obrenovic StankovicNo ratings yet
- Hydrocephalus Clinical Pathway: James L. PatigayonDocument6 pagesHydrocephalus Clinical Pathway: James L. PatigayonJayson OlileNo ratings yet
- Different in the therapy of pressure negtotheeva single-useFrom EverandDifferent in the therapy of pressure negtotheeva single-useNo ratings yet
- Assuring Optimal Trauma Care-The RoleDocument8 pagesAssuring Optimal Trauma Care-The RolerisnayektiNo ratings yet
- Mgmentof TBIDocument3 pagesMgmentof TBIrisnayektiNo ratings yet
- Non Operative Management Splenic Injury WGradingDocument4 pagesNon Operative Management Splenic Injury WGradingrisnayektiNo ratings yet
- Leaving Against Medical Advice: Facing The Issue in The Emergency DepartmentDocument6 pagesLeaving Against Medical Advice: Facing The Issue in The Emergency DepartmentrisnayektiNo ratings yet
- ICUManagementof CPPDocument2 pagesICUManagementof CPPrisnayektiNo ratings yet
- Materi Mohd Hosni, CamoDocument33 pagesMateri Mohd Hosni, CamorisnayektiNo ratings yet
- MATERI SENJA SETIAKA, S.Kep. Ns.Document50 pagesMATERI SENJA SETIAKA, S.Kep. Ns.risnayektiNo ratings yet
- Preventionof HypothermiaDocument2 pagesPreventionof HypothermiarisnayektiNo ratings yet
- Development Dysplasia of HipDocument151 pagesDevelopment Dysplasia of HipKyla Obrien100% (1)
- Compartment Syndrome PDFDocument187 pagesCompartment Syndrome PDFAmayaNo ratings yet
- #12 - NCM 109 (Rle) - TransesDocument4 pages#12 - NCM 109 (Rle) - TransesJaimie BanaagNo ratings yet
- Sample Question Paper - PeDocument6 pagesSample Question Paper - PedinguNo ratings yet
- Revision 1.Document9 pagesRevision 1.Sebayari RiosNo ratings yet
- Journal Reading Acute Spinal Cord InjuryDocument14 pagesJournal Reading Acute Spinal Cord InjuryamandaNo ratings yet
- The Skeletal SystemDocument96 pagesThe Skeletal SystemCheghe PerezNo ratings yet
- Treatment Procedures For EachDocument10 pagesTreatment Procedures For EachJovel WeirNo ratings yet
- History and Physical Exam in RheumatologyDocument111 pagesHistory and Physical Exam in Rheumatologyimaday99No ratings yet
- Risk Assessment - Abseiling TowerDocument1 pageRisk Assessment - Abseiling TowerChar KuahNo ratings yet
- Brittany Juanita HallDocument5 pagesBrittany Juanita HallMcKenzie Stauffer100% (1)
- Neck, Part 1: With Dr. Craig CanbyDocument36 pagesNeck, Part 1: With Dr. Craig CanbyMalikkahNo ratings yet
- JHA - MCY Upgrade Preparation For Salman Phase 1 (Drainage&Scaffolding)Document5 pagesJHA - MCY Upgrade Preparation For Salman Phase 1 (Drainage&Scaffolding)hairol uisbNo ratings yet
- Safety InductionDocument63 pagesSafety Inductionereniacamilo09No ratings yet
- Physiogenesis and Psychogenesis in The 'Post-Concussional Syndrome'Document11 pagesPhysiogenesis and Psychogenesis in The 'Post-Concussional Syndrome'IgorNo ratings yet
- Physical Education: Quarter 3 - Module 1Document30 pagesPhysical Education: Quarter 3 - Module 1edel dearce IIINo ratings yet
- Skeletal Trauma Basic Science Management and Reconstruction 2 Volume Set 6Th Edition Bruce Browner All ChapterDocument68 pagesSkeletal Trauma Basic Science Management and Reconstruction 2 Volume Set 6Th Edition Bruce Browner All Chapterherbert.hawkins665100% (5)
- Primary THA in DDH Crow's 2&3: Manor Hospital Walsall A Teaching Trust of University of BirminghamDocument32 pagesPrimary THA in DDH Crow's 2&3: Manor Hospital Walsall A Teaching Trust of University of BirminghamDr Meenakshi ParwaniNo ratings yet
- Fracture AssessmentDocument8 pagesFracture AssessmentmandyNo ratings yet
- The Basic Principles of External Fixation Using The Ilizarov DeviceDocument30 pagesThe Basic Principles of External Fixation Using The Ilizarov DevicedendroaspisblackNo ratings yet
- Ent Mcqs For Part I Exam: Prepared By: Dr. Fouad ShamsanDocument86 pagesEnt Mcqs For Part I Exam: Prepared By: Dr. Fouad ShamsanAli QuwarahNo ratings yet
- BFO-Review of Pathology AFODocument32 pagesBFO-Review of Pathology AFOnovitaNo ratings yet
- Rehabilitation and Treatments of Sports InjuriesDocument20 pagesRehabilitation and Treatments of Sports InjuriesRAJESH MALIKNo ratings yet
- Dokumen - Tips Handbook of Third Edition Osteology Handbook of Handbook of Third Edition OsteologyDocument19 pagesDokumen - Tips Handbook of Third Edition Osteology Handbook of Handbook of Third Edition OsteologyJULIANA MATHAVANo ratings yet
- Presidential Owners ManualDocument15 pagesPresidential Owners ManualMano DanoNo ratings yet
- Pelvic Walls, Joints, Vessels & Nerves, Pelvic Organs PPT FinalDocument106 pagesPelvic Walls, Joints, Vessels & Nerves, Pelvic Organs PPT Finalntege stuart100% (1)
- Spine Surgery - A Practical Atlas - Wetzel, F. Todd Hanley, Edward N - 2002 - New York - McGraw-Hill - 9780838586174 - Anna's ArchiveDocument248 pagesSpine Surgery - A Practical Atlas - Wetzel, F. Todd Hanley, Edward N - 2002 - New York - McGraw-Hill - 9780838586174 - Anna's ArchiveSrikanthNo ratings yet
- Maxillofacial TraumaDocument70 pagesMaxillofacial Traumaeman_879_123456No ratings yet
- Las 4.2 - Hope 2 - Sports Related InjuriesDocument4 pagesLas 4.2 - Hope 2 - Sports Related InjuriesJoebert MaderaNo ratings yet