You might also like
- Membership FormDocument2 pagesMembership FormkamalsalmanNo ratings yet
- GMI Brochure PDFDocument2 pagesGMI Brochure PDFSulakhe ShounakNo ratings yet
- Turito 2Document2 pagesTurito 2M S SHARATHNo ratings yet
- 05B Casework Sup Genogram FormatDocument4 pages05B Casework Sup Genogram FormatAnonymous kF9IXBPNo ratings yet
- James - Edward - Splitek-5741e704fb77ad3 2Document7 pagesJames - Edward - Splitek-5741e704fb77ad3 2explota.tofmNo ratings yet
- Membership Application: Mail This Form or Apply Online atDocument1 pageMembership Application: Mail This Form or Apply Online atAndrew SeguelNo ratings yet
- Your Annual Gwinnett Retirement System Benefits StatementDocument3 pagesYour Annual Gwinnett Retirement System Benefits StatementMirela SzathmariNo ratings yet
- Mr. Kakku Ji: Insurance Proposal ForDocument6 pagesMr. Kakku Ji: Insurance Proposal ForHarish ChandNo ratings yet
- Population Pyramids GeographyDocument4 pagesPopulation Pyramids GeographyVictoria ParryNo ratings yet
- GSSFDocument1 pageGSSFgonNo ratings yet
- City of Ridgeland SOVC REPORT (1) Official Results SPecial Election Alderman at Large Feb 7, 2012Document1 pageCity of Ridgeland SOVC REPORT (1) Official Results SPecial Election Alderman at Large Feb 7, 2012D.I. SmithNo ratings yet
- Seals Lts Reg Form 2021-22 - SallyDocument2 pagesSeals Lts Reg Form 2021-22 - Sallybala naidooNo ratings yet
- Housing Rent US CensusDocument402 pagesHousing Rent US CensusMcKenzie StaufferNo ratings yet
- Nigeria Police Force Admission Portal - NPFDocument1 pageNigeria Police Force Admission Portal - NPFOlayinka IyandaNo ratings yet
- What Is Youth DevelopmentDocument25 pagesWhat Is Youth DevelopmentSahil SumitNo ratings yet
- Reporting To Work Instructions Rev 25feb21Document5 pagesReporting To Work Instructions Rev 25feb21Fahad FazilNo ratings yet
- Afcarsreport 20Document6 pagesAfcarsreport 20api-105678284No ratings yet
- Kevin Paul Bender-Bbaa28607d9cb49Document9 pagesKevin Paul Bender-Bbaa28607d9cb49harry.barnes7218No ratings yet
- Form Candidate PAG 2018Document2 pagesForm Candidate PAG 2018sulaiman fikranNo ratings yet
- Wayne RobertsonDocument2 pagesWayne RobertsonChand MinhasNo ratings yet
- CBS News Same-Sex Marriage Poll 04-03-09Document3 pagesCBS News Same-Sex Marriage Poll 04-03-09Unite the FightNo ratings yet
- UNN SM Core PortalDocument1 pageUNN SM Core PortalpeaceugbedeNo ratings yet
- Spectrum News/Siena College PollDocument4 pagesSpectrum News/Siena College PollCraigNo ratings yet
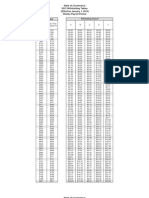
- 2012 CT Withholding TablesDocument8 pages2012 CT Withholding TablesHelen BennettNo ratings yet
- Wisconsin Identification Card (ID) ApplicationDocument2 pagesWisconsin Identification Card (ID) ApplicationAidan ZuehrNo ratings yet
- Nigeria Police Force Admission Portal - NPFDocument1 pageNigeria Police Force Admission Portal - NPFkennynaze.kmNo ratings yet
- Meridian Health Plan Member Information: Member Responsible Party/GuardianDocument1 pageMeridian Health Plan Member Information: Member Responsible Party/GuardianMythe CastilloNo ratings yet
- USKSF Membership Application FormDocument1 pageUSKSF Membership Application FormShi Fu Michael ShafferNo ratings yet
- Unit+3+Changing+Populations+Assignment+ +2c+Cgc1d1+ +Canada+Population+PyramidDocument4 pagesUnit+3+Changing+Populations+Assignment+ +2c+Cgc1d1+ +Canada+Population+PyramidAfnansstuffNo ratings yet
- Zara Margarret JavedDocument1 pageZara Margarret JavedAnees JavedNo ratings yet
- View of People Regarding The Newspaper They ReadDocument3 pagesView of People Regarding The Newspaper They ReadGaurav SinghNo ratings yet
- Caleb Long StatementDocument1 pageCaleb Long StatementSantiago FloresNo ratings yet
- Joe Giudice Smiles After ICE Release in First Photo in Over 3 YearsDocument1 pageJoe Giudice Smiles After ICE Release in First Photo in Over 3 YearsJared SmithNo ratings yet
- Bulan Januari 2023Document2 pagesBulan Januari 2023Sinli Nur HNo ratings yet
- Grevic 19Document1 pageGrevic 19GutiNo ratings yet
- Biden vs. Trump: Neck and Neck in Texas, Quinnipiac University Poll Finds Nearly 6 in 10 Say Yes To Mail-In Ballots in NovemberDocument22 pagesBiden vs. Trump: Neck and Neck in Texas, Quinnipiac University Poll Finds Nearly 6 in 10 Say Yes To Mail-In Ballots in NovemberThe TexanNo ratings yet
- Regional DEED Data, Becker County, Nov. 15, 2021Document8 pagesRegional DEED Data, Becker County, Nov. 15, 2021Michael AchterlingNo ratings yet
- Exclusive Spectrum News Siena College Poll ResultsDocument9 pagesExclusive Spectrum News Siena College Poll ResultsJohn McLaughlinNo ratings yet
- WNE Polling - Nov. 2013 Casino SurveyDocument8 pagesWNE Polling - Nov. 2013 Casino SurveyMassLiveNo ratings yet
- Click Here To Find Out!Document2 pagesClick Here To Find Out!Bryan DavenportNo ratings yet
- E 5 DFD 5Document3 pagesE 5 DFD 5bayworld creativesNo ratings yet
- Chi 223 Results Part 2Document8 pagesChi 223 Results Part 2tempuser59No ratings yet
- Mor Files 9785534Document6 pagesMor Files 9785534tyleraigbekaenNo ratings yet
- Navy - PrintDocument7 pagesNavy - PrintPeter abuh SabohNo ratings yet
- CSU - I-20 Request Form UG and PGDocument3 pagesCSU - I-20 Request Form UG and PGxspiiirONo ratings yet
- Dispensary Mandatory Date of Birth of The Family Should Be in Format (Dd/mm/yyy)Document6 pagesDispensary Mandatory Date of Birth of The Family Should Be in Format (Dd/mm/yyy)Sahil SinghNo ratings yet
- Sacramento County CPS InformationDocument2 pagesSacramento County CPS InformationABC10No ratings yet
- Methods in Business ResearchDocument3 pagesMethods in Business Researchasif tajNo ratings yet
- Employment Application Form: PhotoDocument3 pagesEmployment Application Form: Photojay balongaNo ratings yet
- Barangay Profile BontocDocument14 pagesBarangay Profile Bontocolisihan1959No ratings yet
- Bio DataDocument1 pageBio DataSuraj GuptaNo ratings yet
- Academic InformationDocument2 pagesAcademic InformationKiprotich SirmaNo ratings yet
- NSS Final SeDocument19 pagesNSS Final SeShrutiNo ratings yet
- Texas Benchmark Final Poll Results 092122Document8 pagesTexas Benchmark Final Poll Results 092122Ashley ValenzuelaNo ratings yet
- Barangay Data BaseDocument208 pagesBarangay Data BaseJustin AbadNo ratings yet
- DOLE TUPAD FormDocument2 pagesDOLE TUPAD FormShienna Mariz Caldito Elep100% (3)
- Apolinario Gaio-2023-03-05t20 - 32 - 16Document2 pagesApolinario Gaio-2023-03-05t20 - 32 - 16gaionario127No ratings yet
- Biodata Parents Certification of WaiverDocument21 pagesBiodata Parents Certification of WaiverJA Ely AnnNo ratings yet
- Sept. 7 Siena Poll On Student LoansDocument3 pagesSept. 7 Siena Poll On Student LoansZach WilliamsNo ratings yet
- 2 AllDocument8 pages2 AllAileen Riza CampoNo ratings yet