You might also like
- TraderJoes CookbookDocument150 pagesTraderJoes Cookbookjennifer.farris12No ratings yet
- Back and Spine AnatomyDocument7 pagesBack and Spine AnatomyCarmela Beatriz Suelan100% (1)
- Workshop PPT (Final) Knee JointDocument127 pagesWorkshop PPT (Final) Knee Jointpasha100% (2)
- Basic BiomechanicsDocument54 pagesBasic BiomechanicsStevenDanielNo ratings yet
- Quantity Surveying & Estimation-2Document17 pagesQuantity Surveying & Estimation-2Engr Nissar KakarNo ratings yet
- Face Bow FINALDocument53 pagesFace Bow FINALAnna PooraniNo ratings yet
- Mobile Management SystemDocument9 pagesMobile Management SystemNaga Sai Anitha NidumoluNo ratings yet
- ASTM A-967-13 Pasivado Inoxidable PDFDocument7 pagesASTM A-967-13 Pasivado Inoxidable PDFmagierezNo ratings yet
- 300 ArticulatorsDocument65 pages300 Articulatorsthebhaskar100% (1)
- M T Ch16 Innate Immunity SDocument30 pagesM T Ch16 Innate Immunity SAnonymous STRYVGKNo ratings yet
- Knee ExaminationDocument5 pagesKnee ExaminationQandeelNo ratings yet
- Lower Extremity Orthotic DevicesDocument27 pagesLower Extremity Orthotic DevicesJohn Patrick ShiaNo ratings yet
- Mandibular Movements ModifiedDocument50 pagesMandibular Movements ModifiedMohamed Gamal100% (1)
- Isolated Roller Guide Shoes WRG200, WRG300Document15 pagesIsolated Roller Guide Shoes WRG200, WRG300Johan GuíaNo ratings yet
- ArticulatorDocument41 pagesArticulatorjohn mwambuNo ratings yet
- Articulators My ClassDocument45 pagesArticulators My ClasssrinivaskalluriNo ratings yet
- The Floreio ProjectDocument15 pagesThe Floreio ProjectMauroZdrilićNo ratings yet
- Lecture 1 TF BiomechanicsDocument63 pagesLecture 1 TF BiomechanicsAlfred JacksonNo ratings yet
- Cast/Splint Choice and Application: Worku K. (MD)Document15 pagesCast/Splint Choice and Application: Worku K. (MD)Worku KifleNo ratings yet
- Reduction, Relocation and Splinting in Emergency Room (RASER)From EverandReduction, Relocation and Splinting in Emergency Room (RASER)No ratings yet
- Occlusion in Fixed ProsthodonticsDocument84 pagesOcclusion in Fixed ProsthodonticsGayathri Gangadharan100% (3)
- K3M 2008 - Form 6Document15 pagesK3M 2008 - Form 6SeanNo ratings yet
- Manalaysay JPT Thesis With Approval PDFDocument103 pagesManalaysay JPT Thesis With Approval PDFTheresa Marie PrestoNo ratings yet
- Foot Akle Leg KneeDocument81 pagesFoot Akle Leg KneeadamufatimamaajiNo ratings yet
- Block 1 Practical 1Document14 pagesBlock 1 Practical 1joe doweNo ratings yet
- 7 Muscle Length TestingDocument8 pages7 Muscle Length Testingbuhlembatha304No ratings yet
- ملخص علم الحركةDocument7 pagesملخص علم الحركةPhantomNo ratings yet
- Robotic Unicondylar PlanningDocument17 pagesRobotic Unicondylar PlanningSuvodipBhattacharyaNo ratings yet
- Examination-Of-Rotational-Profile 2Document2 pagesExamination-Of-Rotational-Profile 2Nadia NajwaNo ratings yet
- Dental Articulator and Face BowDocument12 pagesDental Articulator and Face BowRihan RihanNo ratings yet
- RADIOLOGY OF KNEE For StudentDocument70 pagesRADIOLOGY OF KNEE For Studentjamie mutucNo ratings yet
- H L: Reduce and Save!: Synopsis - Anatomy and The DiseaseDocument5 pagesH L: Reduce and Save!: Synopsis - Anatomy and The DiseaseEl OnNo ratings yet
- Radiography of The Thoracic SpineDocument59 pagesRadiography of The Thoracic SpineEzra NserekoNo ratings yet
- 2023 - 02 - 17 WPA Classification Rules and Regulations - Edition February 2023 - FinalDocument183 pages2023 - 02 - 17 WPA Classification Rules and Regulations - Edition February 2023 - FinalOktaviani FitriyahNo ratings yet
- Knee (Word)Document18 pagesKnee (Word)dwNo ratings yet
- Face Bows and Articulators PDFDocument30 pagesFace Bows and Articulators PDFggNo ratings yet
- GoniometryDocument55 pagesGoniometryKhondokar ArafatNo ratings yet
- Prosthetic Knee Joints: Dot IiDocument49 pagesProsthetic Knee Joints: Dot IiAlfred JacksonNo ratings yet
- Fractures TCA 1 2-27-08Document6 pagesFractures TCA 1 2-27-08api-3822433No ratings yet
- GoniometrystandardsDocument12 pagesGoniometrystandardsPips RahulNo ratings yet
- Dentatus: More Than 85 Years of Swedish Quality in The Global Dental ServiceDocument24 pagesDentatus: More Than 85 Years of Swedish Quality in The Global Dental ServiceHùngNo ratings yet
- Orthoses, Prostheses and Ambulatory Aids For BPTDocument75 pagesOrthoses, Prostheses and Ambulatory Aids For BPTSourav DeyNo ratings yet
- MovSciLec MSC 2101 Week13Document14 pagesMovSciLec MSC 2101 Week13Mary SotoNo ratings yet
- The Facebow: Occlusion Lab ExamDocument7 pagesThe Facebow: Occlusion Lab ExamNaresh TeresNo ratings yet
- Advanced Radiographic Positions For The Lower Extremities: by Prof. Jarek StelmarkDocument39 pagesAdvanced Radiographic Positions For The Lower Extremities: by Prof. Jarek StelmarkLeannys HernándezNo ratings yet
- The Knee Is One of The More Commonly Injured JointsDocument4 pagesThe Knee Is One of The More Commonly Injured JointslieNo ratings yet
- Musculoskeletal SystemDocument15 pagesMusculoskeletal SystemFRIA DEMAISIPNo ratings yet
- Tutorial - Basic Rigging: Nik PavlovDocument5 pagesTutorial - Basic Rigging: Nik PavlovAntonycruzvNo ratings yet
- Dental ArticulatorsDocument48 pagesDental ArticulatorsMahmoud Gamal El FeelNo ratings yet
- Lower Limb Positioning Peer MentoringDocument92 pagesLower Limb Positioning Peer MentoringJae Em DiestroNo ratings yet
- Surgery 1 - 1st ray-MTPJ (1-25-08)Document3 pagesSurgery 1 - 1st ray-MTPJ (1-25-08)Eddie MillsNo ratings yet
- Hip ExaminationDocument7 pagesHip ExaminationWaqas Haleem100% (1)
- LecturesDocument16 pagesLecturesAmr Mohamed GalalNo ratings yet
- MSK Clin Skills Ankle+FootDocument3 pagesMSK Clin Skills Ankle+FootmalikNo ratings yet
- Distal Radius Osteotomy ComDocument37 pagesDistal Radius Osteotomy ComIskolar MorenoNo ratings yet
- Angulos y Arcos de MovimientoDocument15 pagesAngulos y Arcos de MovimientoIsaac Godìnez100% (2)
- 2Beginner-Intermediate Cello-Double Bass Left Hand PedagogyDocument8 pages2Beginner-Intermediate Cello-Double Bass Left Hand Pedagogyblon majorsNo ratings yet
- Reading Knee - RamaDocument33 pagesReading Knee - RamavjhvghcghcghghNo ratings yet
- The ArticulatorDocument16 pagesThe ArticulatorHamza RiazNo ratings yet
- Articulators Nehal MainaliDocument89 pagesArticulators Nehal MainaliNehal MainaliNo ratings yet
- Teknik Radiografi Cruris Dan Knee Joint: Yeti Kartikasari, ST.M.KesDocument21 pagesTeknik Radiografi Cruris Dan Knee Joint: Yeti Kartikasari, ST.M.KesFavian Nadia SaputraNo ratings yet
- Examination of ElbowDocument82 pagesExamination of Elbowbhavikaagarwal07No ratings yet
- Osteotomiesaroundthehip 160203173448Document130 pagesOsteotomiesaroundthehip 160203173448Mit ParikhNo ratings yet
- Anatomy (Patellofemoral Joint)Document3 pagesAnatomy (Patellofemoral Joint)Andy Delos ReyesNo ratings yet
- Osseous Structure Vs FunctionDocument1 pageOsseous Structure Vs FunctionalezanderiiiINo ratings yet
- X-Ray Views HipDocument1 pageX-Ray Views Hipjuly mirandillaNo ratings yet
- Hip ExaminationDocument4 pagesHip ExaminationLiyana Huda KamaruddinNo ratings yet
- Cubitus Varus, Elbow Joint, Mitali JoshiDocument13 pagesCubitus Varus, Elbow Joint, Mitali JoshiKapil Lakhwara100% (1)
- Tips for Everyday Life and Sports With an Artificial Joint: Expert guidebook for dealing with a prosthesis for patients with a new hip or knee jointFrom EverandTips for Everyday Life and Sports With an Artificial Joint: Expert guidebook for dealing with a prosthesis for patients with a new hip or knee jointNo ratings yet
- Decomposition of Diacetone AlcoholDocument3 pagesDecomposition of Diacetone Alcoholaryajs2017No ratings yet
- Naples Capital Improvement Plan 2022-2026Document215 pagesNaples Capital Improvement Plan 2022-2026Omar Rodriguez OrtizNo ratings yet
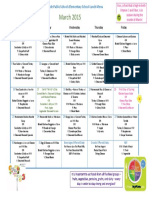
- Seaside Elementary School Lunch Menu LewisDocument1 pageSeaside Elementary School Lunch Menu Lewisapi-345910065No ratings yet
- Egipto Underweight Case Study MNT1Document14 pagesEgipto Underweight Case Study MNT1Hyacinth M. NotarteNo ratings yet
- T1001W6F011Document1 pageT1001W6F011Asim SaleemNo ratings yet
- Tenda Catalogo 2020 PDFDocument24 pagesTenda Catalogo 2020 PDFTenda Región AndinaNo ratings yet
- Unit Homework Momentum Its Conservation Ans KeyDocument6 pagesUnit Homework Momentum Its Conservation Ans KeyKristyne Olicia100% (1)
- SAE AS4059F Table1Document2 pagesSAE AS4059F Table1CherryNo ratings yet
- STP-27RD Press Kit MAY 2019: Launching On Electron Vehicle Six: 'Thats A Funny Looking Cactus'Document9 pagesSTP-27RD Press Kit MAY 2019: Launching On Electron Vehicle Six: 'Thats A Funny Looking Cactus'SrivasNo ratings yet
- Data Sheet Tiristor s701c15n3sDocument8 pagesData Sheet Tiristor s701c15n3sLeo SalgadoNo ratings yet
- Capgemini TestsDocument50 pagesCapgemini TestsObli Narasimha RajanNo ratings yet
- Earth Pressure CalculationsDocument5 pagesEarth Pressure Calculationsnazeer_mohdNo ratings yet
- Snoo Wilson Adaptation of The BedbugDocument49 pagesSnoo Wilson Adaptation of The BedbugMike Vanden HeuvelNo ratings yet
- MOV S ManualDocument84 pagesMOV S ManualAbdulrahmanNo ratings yet
- Robot Car MatlabDocument93 pagesRobot Car MatlabDalasa OljiraNo ratings yet
- Advanced Training Course On FPGA Design and VHDL For Hardware Simulation and SynthesisDocument17 pagesAdvanced Training Course On FPGA Design and VHDL For Hardware Simulation and SynthesisMD RockyNo ratings yet
- MST WRN Overview UsDocument4 pagesMST WRN Overview UsedgarNo ratings yet
- A Project Work Submitted in Partial Fulfilment of The Requirement For The Degree of B.SC (Honours) in M.J.P. Rohilkhand University, BareillyDocument4 pagesA Project Work Submitted in Partial Fulfilment of The Requirement For The Degree of B.SC (Honours) in M.J.P. Rohilkhand University, Bareillymohd ameerNo ratings yet
- Assessment of Nutritional Status of People Living With HIV/AIDS (PLWHA) in The Age Group of 18-55 YearsDocument12 pagesAssessment of Nutritional Status of People Living With HIV/AIDS (PLWHA) in The Age Group of 18-55 YearsIOSRjournalNo ratings yet
- Examen de Corigenţă La Limba Engleză Clasa A VIIDocument6 pagesExamen de Corigenţă La Limba Engleză Clasa A VIIAnonymous HdI5CTRNo ratings yet
- The Basic Parts of An Airplane and Their FunctionsDocument4 pagesThe Basic Parts of An Airplane and Their FunctionsSubash DhakalNo ratings yet