You might also like
- Development and Evaluation of The Compassionate Altruism ScaleDocument1 pageDevelopment and Evaluation of The Compassionate Altruism ScaleccareemailNo ratings yet
- NEO PI SummaryDocument12 pagesNEO PI SummaryRoseNTolentinoNo ratings yet
- Analysis of Clinical Trials Using SAS: A Practical Guide, Second EditionFrom EverandAnalysis of Clinical Trials Using SAS: A Practical Guide, Second EditionNo ratings yet
- Jer 17 4 226Document8 pagesJer 17 4 226Magno FilhoNo ratings yet
- Ijspt 14 845Document15 pagesIjspt 14 845Magno FilhoNo ratings yet
- Sue Yoshi 2007Document29 pagesSue Yoshi 2007Mark DeryNo ratings yet
- Publishedversionofthe MScarticleDocument6 pagesPublishedversionofthe MScarticleKanchit SuwanswadNo ratings yet
- Is The Royal London Space Analysis Reliable and Does It in Uence Orthodontic Treatment Decisions?Document5 pagesIs The Royal London Space Analysis Reliable and Does It in Uence Orthodontic Treatment Decisions?Kanchit SuwanswadNo ratings yet
- Prognosis of Six-Month Functioning After Moderate To Severe Traumatic Brain Injury: A Systematic Review of Prospective Cohort StudiesDocument12 pagesPrognosis of Six-Month Functioning After Moderate To Severe Traumatic Brain Injury: A Systematic Review of Prospective Cohort StudiesYan Sheng HoNo ratings yet
- Demand Forecasting and Inventory Control A Simulation Study On Automotive Spare Parts PDFDocument16 pagesDemand Forecasting and Inventory Control A Simulation Study On Automotive Spare Parts PDFRais HaqNo ratings yet
- Trends of Repetitive Transcranial Magnetic Stimulation From 2009 To 2018 - A Bibliometric AnalysisDocument11 pagesTrends of Repetitive Transcranial Magnetic Stimulation From 2009 To 2018 - A Bibliometric AnalysiszkydjssNo ratings yet
- 15 Treatment Outcomes of Meniscal Root TearsDocument11 pages15 Treatment Outcomes of Meniscal Root Tearsdados2000No ratings yet
- Functional Evaluation For Patients WithDocument6 pagesFunctional Evaluation For Patients WithWilton Wylie IskandarNo ratings yet
- The Fugl-Meyer Upper Extremity ScaleDocument2 pagesThe Fugl-Meyer Upper Extremity ScaleRosa M. AlcaláNo ratings yet
- ADMET Modeling Approaches in Drug DiscoveryDocument9 pagesADMET Modeling Approaches in Drug Discoveryjuan carlos monasterio saezNo ratings yet
- The Revised Bristol Rheumatoid Arthritis Fatigue Measures and The Rheumatoid Arthritis Impact of Disease Scale - Validation in Six CountriesDocument9 pagesThe Revised Bristol Rheumatoid Arthritis Fatigue Measures and The Rheumatoid Arthritis Impact of Disease Scale - Validation in Six CountriesROBINSON STALIN TIPANLUISA TIPANLUISANo ratings yet
- Physical Therapy in Sport: Gulcan Harput, Hande Guney-Deniz, John Nyland, Yavuz KocabeyDocument10 pagesPhysical Therapy in Sport: Gulcan Harput, Hande Guney-Deniz, John Nyland, Yavuz KocabeyNaara LibNo ratings yet
- A Critical Evaluation of The Pitchfork AnalysisDocument15 pagesA Critical Evaluation of The Pitchfork AnalysisKaruna ShresthaNo ratings yet
- Rim 2016Document29 pagesRim 2016buihuyanh2018No ratings yet
- Chow 2019Document6 pagesChow 2019JESUS GABRIEL RAMIREZ ESCALANTENo ratings yet
- Anthropometric Determination of Craniofacial Morphology: American Journal of Medical Genetics October 1996Document6 pagesAnthropometric Determination of Craniofacial Morphology: American Journal of Medical Genetics October 1996Diego TamesNo ratings yet
- CFC Uruguay y EspañaDocument5 pagesCFC Uruguay y EspañaAndres OliveriNo ratings yet
- Cplex Imrt PDFDocument12 pagesCplex Imrt PDFDan MatthewsNo ratings yet
- Journal Pre-Proof: Journal of Bodywork & Movement TherapiesDocument62 pagesJournal Pre-Proof: Journal of Bodywork & Movement TherapiesValeria Tabares SanchezNo ratings yet
- Antropometria en BellezaDocument8 pagesAntropometria en BellezaRosa Natalia Muente RojasNo ratings yet
- A Particle Swarm Optimization Algorithm For Mixed Variable Nonlinear ProblemsDocument14 pagesA Particle Swarm Optimization Algorithm For Mixed Variable Nonlinear ProblemsAhmed WestministerNo ratings yet
- Modeling VI and VDRL Feedback Functions: Searching Normative Rules Through Computational SimulationDocument13 pagesModeling VI and VDRL Feedback Functions: Searching Normative Rules Through Computational SimulationProf. Carlos Eduardo Costa - CaêNo ratings yet
- Modelling and Trading Commodities With A New Deep Belief NetworkDocument7 pagesModelling and Trading Commodities With A New Deep Belief Networkdbr trackdNo ratings yet
- Morris 2Document22 pagesMorris 2IsmaelLouGomezNo ratings yet
- Ebp PaperDocument16 pagesEbp Paperapi-583545759No ratings yet
- #PENTING Demeurechy2018Document19 pages#PENTING Demeurechy2018Octapaedi SoetomoNo ratings yet
- NEO PI SummaryDocument13 pagesNEO PI SummaryEdielyn Gonzalvo GutierrezNo ratings yet
- Peterson 2008Document10 pagesPeterson 2008Fatamorgana AbdullahNo ratings yet
- 5factor ModelDocument15 pages5factor ModelAlmeDina AganovicNo ratings yet
- Trigonometric Similarity Measures For Neutrosophic Hypersoft Sets With Application To Renewable Energy Source SelectionDocument11 pagesTrigonometric Similarity Measures For Neutrosophic Hypersoft Sets With Application To Renewable Energy Source SelectionScience DirectNo ratings yet
- Predicting The Brazilian Stock Market Through Neural Networks and AdaptiveDocument4 pagesPredicting The Brazilian Stock Market Through Neural Networks and AdaptiveFarhan AhmedNo ratings yet
- Prótese No JoelhoDocument17 pagesPrótese No JoelhoPaula SampaioNo ratings yet
- FarkasDeutsch 1996Document6 pagesFarkasDeutsch 1996cristhian.eeuu.psNo ratings yet
- Bogacz CohenDocument66 pagesBogacz CohenmopendakNo ratings yet
- Iastm ReviewDocument14 pagesIastm Reviewcris.endo.ceNo ratings yet
- Informatic Parcellation of The Network Involved in The Computation of Subjective Value, Clithero & Rangel 2014Document14 pagesInformatic Parcellation of The Network Involved in The Computation of Subjective Value, Clithero & Rangel 2014María SolariNo ratings yet
- 1 s2.0 S0897189716300234 MainDocument7 pages1 s2.0 S0897189716300234 MainVenice s SantosNo ratings yet
- Item Response Theory Analysis of The IPIP Big-Five ScalesDocument23 pagesItem Response Theory Analysis of The IPIP Big-Five ScalesPersephona13No ratings yet
- Ayala2012-DikonversiDocument8 pagesAyala2012-DikonversinilamNo ratings yet
- Norms For The Rey-Osterrieth Complex FigureDocument23 pagesNorms For The Rey-Osterrieth Complex Figurelaura4dap100% (2)
- Physiotherapy: JournalofDocument1 pagePhysiotherapy: JournalofCyed CamiNo ratings yet
- Two-Minute Step Test of Exercise Capacity: Systematic Review of Procedures, Performance, and Clinimetric PropertiesDocument9 pagesTwo-Minute Step Test of Exercise Capacity: Systematic Review of Procedures, Performance, and Clinimetric PropertieslokoxfalsoNo ratings yet
- A Systematic Review On The Effect of Mechanical Stretch On Hypertrophic Scars After Burn InjuriesDocument9 pagesA Systematic Review On The Effect of Mechanical Stretch On Hypertrophic Scars After Burn Injuriesrizk86No ratings yet
- A Tutorial On Modeling fMRI Data Using A General Linear ModelDocument25 pagesA Tutorial On Modeling fMRI Data Using A General Linear ModelAnkit GuptaNo ratings yet
- SPE-102079-PA Gringarten From Straight Lines To DeconvolutionDocument22 pagesSPE-102079-PA Gringarten From Straight Lines To DeconvolutionChávez Ibarra Sergio Kevin100% (1)
- Criterion-Related Validity of Sit-And-Reach Test For Estimating Hamstring and Lumber ExtensibilityDocument14 pagesCriterion-Related Validity of Sit-And-Reach Test For Estimating Hamstring and Lumber Extensibility2022736541No ratings yet
- Interpreting Change Scores For Pain and Functional Status in Low Back Pain - Towards International Consensus Regarding Minimal Important ChangeDocument6 pagesInterpreting Change Scores For Pain and Functional Status in Low Back Pain - Towards International Consensus Regarding Minimal Important ChangeAmbar MonzoncilloNo ratings yet
- PET NEMA IQ Phantom Dataset Image 2021 IRANDocument10 pagesPET NEMA IQ Phantom Dataset Image 2021 IRANp110054No ratings yet
- Part 2Document10 pagesPart 2soho1303No ratings yet
- Measurement of Knee Joint Range of Motion With A Digital Goniometer: A Reliability StudyDocument7 pagesMeasurement of Knee Joint Range of Motion With A Digital Goniometer: A Reliability StudyTripatdeep SinghNo ratings yet
- Fuzzy C-Means Clustering Algorithm For Directional Data (FCM4DD)Document7 pagesFuzzy C-Means Clustering Algorithm For Directional Data (FCM4DD)Yanelin Abarca PonceNo ratings yet
- Hansen 2017 Regression Kink With An Unknown ThresholdDocument14 pagesHansen 2017 Regression Kink With An Unknown ThresholdOdalice SampaioNo ratings yet
- Jaw Rotation in Dysarthria Measured With A Single Electromagnetic Articulography SensorDocument15 pagesJaw Rotation in Dysarthria Measured With A Single Electromagnetic Articulography SensorRosario Lartiga MazryNo ratings yet
- Measures of Effect Size For Comparative Studies Applications, Interpretations and LimitationsDocument46 pagesMeasures of Effect Size For Comparative Studies Applications, Interpretations and LimitationsXiang-Yang LouNo ratings yet
- 2003 Evaluating SngleCase Data Compare 7 Stat Methods Parker PDFDocument23 pages2003 Evaluating SngleCase Data Compare 7 Stat Methods Parker PDFAdina CarterNo ratings yet
- Management Thoracic Pain 2019Document9 pagesManagement Thoracic Pain 2019Lotte WeggemanNo ratings yet
- CTRG2015 Submission 451Document12 pagesCTRG2015 Submission 451Sri RamyaNo ratings yet
- Valiandes 2017Document17 pagesValiandes 2017Banu a/p Ramanan IPGKKBNo ratings yet
- Correlation Between Adversity Quotient (AQ) With IQ, EQ and SQ Among Polytechnic Students Using Rasch ModelDocument8 pagesCorrelation Between Adversity Quotient (AQ) With IQ, EQ and SQ Among Polytechnic Students Using Rasch ModelManojsinghpatel ManojsinghpatelNo ratings yet
- Psychological Measurement: Theory, Paradoxes, and PrototypesDocument12 pagesPsychological Measurement: Theory, Paradoxes, and PrototypesJuan Diego González BustilloNo ratings yet
- Journal 1: Exploratory Factor Analysis (EFA) and Confirmatory Factor Analysis (CFA) With Rasch Measurement Model Critique ConclusionDocument4 pagesJournal 1: Exploratory Factor Analysis (EFA) and Confirmatory Factor Analysis (CFA) With Rasch Measurement Model Critique ConclusionPavitra KannadassNo ratings yet
- Winsteps Tutorial 1 PDFDocument37 pagesWinsteps Tutorial 1 PDFpipequinnNo ratings yet
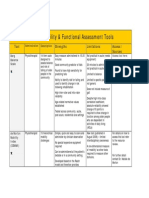
- Assessment Tools for Mobility & Functional IndependenceDocument4 pagesAssessment Tools for Mobility & Functional Independencesonya63265No ratings yet
- Volune-6 - Issue-1-2012Document256 pagesVolune-6 - Issue-1-2012Trung NguyenNo ratings yet
- LTMDocument49 pagesLTMparbuiNo ratings yet
- The de Morton Mobility Index (DEMMI) - An Essential Health IndexDocument15 pagesThe de Morton Mobility Index (DEMMI) - An Essential Health IndexWilsonWooNo ratings yet
- Face Q Scales For Health Related Quality of Life Development and ValidationDocument12 pagesFace Q Scales For Health Related Quality of Life Development and ValidationRoxana MilicaNo ratings yet
- Paper Reference For Transport IntegrationDocument18 pagesPaper Reference For Transport IntegrationDanang Desfri ANo ratings yet
- A Telehealth Delivered Toilet Training Intervention For Children With AutismDocument9 pagesA Telehealth Delivered Toilet Training Intervention For Children With AutismFernanda Guinter HerterNo ratings yet
- Acceptance On Mobile Learning Via SMS: A Rasch Model AnalysisDocument7 pagesAcceptance On Mobile Learning Via SMS: A Rasch Model AnalysisrozhanidrusNo ratings yet
- Embretson PsychometricDocument22 pagesEmbretson PsychometricSilviu OroianuNo ratings yet
- Item Banking. ERIC/AE DigestDocument7 pagesItem Banking. ERIC/AE DigestAndi UlfaNo ratings yet
- Best Test DesignDocument242 pagesBest Test Designjose peralesNo ratings yet
- Promoting Childrens and Adolescents Social and Emotional DevelopmentDocument16 pagesPromoting Childrens and Adolescents Social and Emotional DevelopmentViviana MuñozNo ratings yet
- Kaiser F.G, Et Al - Behavioral-Based Environmental Attitude Development of An Instrument For AdolescentsDocument10 pagesKaiser F.G, Et Al - Behavioral-Based Environmental Attitude Development of An Instrument For Adolescentsmochamad ali ChomainiNo ratings yet
- Rasch Model: January 2010Document3 pagesRasch Model: January 2010Raj'z KingzterNo ratings yet
- Teacher Assessment Literacy and Student Outcomes in The Province of Tawi-Tawi, PhilippinesDocument26 pagesTeacher Assessment Literacy and Student Outcomes in The Province of Tawi-Tawi, PhilippinesAllanNo ratings yet
- Dry Eye DiseaseDocument250 pagesDry Eye DiseaseFarhanif FauzanputraNo ratings yet
- Introduction To IRTDocument64 pagesIntroduction To IRTClinPsyNo ratings yet
- Manual Do Usuário Do Laz Stats PDFDocument476 pagesManual Do Usuário Do Laz Stats PDFLuiz PereiraNo ratings yet
- Borsboom, D., Mellenbergh, G. J., Van Heerden, J. (2003) .Document17 pagesBorsboom, D., Mellenbergh, G. J., Van Heerden, J. (2003) .Cristina Aguilera SaavedraNo ratings yet
- Real Statistics Examples Correlation ReliabilityDocument404 pagesReal Statistics Examples Correlation ReliabilityMetalurgista SosNo ratings yet
- Bayesian Inference For Multistage and Other Incomplete DesignsDocument19 pagesBayesian Inference For Multistage and Other Incomplete DesignstimobechgerNo ratings yet
- Rasch ModelDocument8 pagesRasch ModelWan AfwanNo ratings yet
- Bogardus Dan Guttman ScaleDocument2 pagesBogardus Dan Guttman ScaleCommunication Management UINo ratings yet