You might also like
- Vitamin B12Document80 pagesVitamin B12Anand Veeranan100% (1)
- UW (Step 1) GIT - Educational Objectives PDFDocument69 pagesUW (Step 1) GIT - Educational Objectives PDFDrbee10No ratings yet
- Osm SupplementsDocument33 pagesOsm SupplementsJunk EmailNo ratings yet
- Inborn Errors of Metabolism IEM 1Document36 pagesInborn Errors of Metabolism IEM 1bhaskar chinnanandhi100% (1)
- With The Photographer by Stephen LeacockDocument8 pagesWith The Photographer by Stephen Leacockhassanainshahi1350% (2)
- Metabolic Disorders 01Document41 pagesMetabolic Disorders 01Brent LagartoNo ratings yet
- BodyTherapē EbookDocument78 pagesBodyTherapē EbookManoj KumarNo ratings yet
- Inborn Errors of MetabolismDocument60 pagesInborn Errors of MetabolismPyneandy KimberlyNo ratings yet
- The Benefits of BCAAs - Poliquin ArticleDocument8 pagesThe Benefits of BCAAs - Poliquin Articlecrespo100% (2)
- VitaminsDocument25 pagesVitaminspikachuNo ratings yet
- Aminacid MetabolismDocument84 pagesAminacid MetabolismAaronJose100% (1)
- Metabolic DisordersDocument59 pagesMetabolic DisordersKeannu Havana100% (1)
- A Complete Neurological Nursing Assessment GuideDocument57 pagesA Complete Neurological Nursing Assessment GuideSarithaRajeshNo ratings yet
- USMD, CSF, SEMEN - Professor'sDocument10 pagesUSMD, CSF, SEMEN - Professor'sMartin ClydeNo ratings yet
- Muscle & Fitness - May 2014 USADocument172 pagesMuscle & Fitness - May 2014 USALavishrack100% (3)
- AUB - Urine Screening For Metabolic DisordersDocument3 pagesAUB - Urine Screening For Metabolic DisordersJeanne Rodiño100% (1)
- Science Driven NutritionDocument39 pagesScience Driven Nutritionjan100% (1)
- Anti Anemic DrugsDocument31 pagesAnti Anemic DrugsAmanda Samurti Pertiwi100% (1)
- Ben Greenfield Bulletproof Your Knee PDFDocument25 pagesBen Greenfield Bulletproof Your Knee PDFhiggs1100% (1)
- Water Soluble VitaminsDocument87 pagesWater Soluble VitaminsSwosti ShresthaNo ratings yet
- Metabolic Disorder Obtain Plasma Ammonia High Normal Obtain Blood PH and C02 Obtain Blood PH and C02Document14 pagesMetabolic Disorder Obtain Plasma Ammonia High Normal Obtain Blood PH and C02 Obtain Blood PH and C02Grace LazarragaNo ratings yet
- Inborn Error of MetabolismDocument27 pagesInborn Error of MetabolismNarayan GhimireNo ratings yet
- Amino Acids Metabolism-Disorders-1Document19 pagesAmino Acids Metabolism-Disorders-1lucky mbaselaNo ratings yet
- Amino Acids Metabolism-DisordersDocument19 pagesAmino Acids Metabolism-Disorderslucky mbaselaNo ratings yet
- Inborn Errors of Amino Acid MetabolismDocument65 pagesInborn Errors of Amino Acid MetabolismSantino MajokNo ratings yet
- Inborn Errors of Protein MetabolismDocument48 pagesInborn Errors of Protein MetabolismChudasama DhruvrajsinhNo ratings yet
- Amino Acidss & AminoacidopathiesDocument55 pagesAmino Acidss & AminoacidopathiesMustafa KhandgawiNo ratings yet
- Chapter X - Mechanism of Protein MetabolismDocument30 pagesChapter X - Mechanism of Protein MetabolismAngelo AngelesNo ratings yet
- Inborn Errors of MetabolismDocument12 pagesInborn Errors of Metabolismmichelle octavianiNo ratings yet
- 4 Protein ReviewDocument87 pages4 Protein Reviewmika de guzmanNo ratings yet
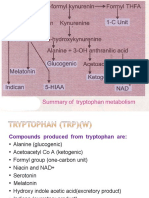
- TryptophanDocument41 pagesTryptophanmahalakshmiNo ratings yet
- Amino AcidsDocument46 pagesAmino AcidsdNo ratings yet
- (Biochemistry) Onsite Assignment No8 - Group XDocument33 pages(Biochemistry) Onsite Assignment No8 - Group XV THNo ratings yet
- Nutrition and Metabolism: Vitamins Presented Dr. Alhaji GblaDocument23 pagesNutrition and Metabolism: Vitamins Presented Dr. Alhaji GblaAlhaji GblaNo ratings yet
- Inborn Error of Metabolism - ايهDocument74 pagesInborn Error of Metabolism - ايهAyaNo ratings yet
- Amino AcidsDocument57 pagesAmino AcidsRAMA ABO SAMRANo ratings yet
- Lipid MetabolismDocument46 pagesLipid MetabolismammuNo ratings yet
- Ketosis & KetoacidosisDocument23 pagesKetosis & KetoacidosisrohishaakNo ratings yet
- 7 NOV 2023 Inborn Errors of Lipid MetabolismDocument66 pages7 NOV 2023 Inborn Errors of Lipid Metabolismwaleedemad649No ratings yet
- Iem - LectureDocument73 pagesIem - LectureAmirhossein SheikhiNo ratings yet
- Bio NotesDocument24 pagesBio NotesIslam MansourNo ratings yet
- Acute Complications of DMDocument57 pagesAcute Complications of DMMalueth AnguiNo ratings yet
- Fatty Acid Oxidation Part 2Document38 pagesFatty Acid Oxidation Part 2mudhugurigirishmaNo ratings yet
- Alcoholism Fatty Liver Liver Cirrhosisg6b1Document48 pagesAlcoholism Fatty Liver Liver Cirrhosisg6b1Franc SalinasNo ratings yet
- Metabolic-Disorders NotesDocument8 pagesMetabolic-Disorders NotesKeannu HavanaNo ratings yet
- The Liver and Its DisordersDocument41 pagesThe Liver and Its Disordersreuben kwotaNo ratings yet
- 7-8. Metabolism of Amino Acids. Catabolism of Individual Amino Acids. Amino Acid Derivatives, Special ProductsDocument87 pages7-8. Metabolism of Amino Acids. Catabolism of Individual Amino Acids. Amino Acid Derivatives, Special ProductsErin HillNo ratings yet
- Amino Acid Metabolism Disorders Series 2Document5 pagesAmino Acid Metabolism Disorders Series 2kiedd_04No ratings yet
- Heme DisordersDocument17 pagesHeme Disorderslucky mbaselaNo ratings yet
- Nutritional Diseases: Jandie P. Sagayno, PTRPDocument54 pagesNutritional Diseases: Jandie P. Sagayno, PTRPKristine Bernadette EnanoriaNo ratings yet
- 2 - Vitamin B ComplexDocument57 pages2 - Vitamin B ComplexPaulinNo ratings yet
- Vitamin 20 JulyDocument33 pagesVitamin 20 JulySafura IjazNo ratings yet
- BP MetabolismDocument28 pagesBP MetabolismVivin MarscellaNo ratings yet
- Investigation of Amino Acids DisordersDocument4 pagesInvestigation of Amino Acids Disorderskiedd_04100% (1)
- A Case of Liver Cirrhosis & Hepatic EncephalopathyDocument21 pagesA Case of Liver Cirrhosis & Hepatic EncephalopathyUdayakumar MannangattiNo ratings yet
- Case Reports Gout Vitamins MineralsDocument23 pagesCase Reports Gout Vitamins MineralsNasreen SultanaNo ratings yet
- B Vitamins in Macronutrient Metabolism-R1Document60 pagesB Vitamins in Macronutrient Metabolism-R1Dr. Mariam AANo ratings yet
- Lecture 5 - Synthesis of Non-Essential AADocument17 pagesLecture 5 - Synthesis of Non-Essential AAciyace7849No ratings yet
- Wa0028.Document46 pagesWa0028.Ziyadan AtiqueNo ratings yet
- Lect1 - 2017Document28 pagesLect1 - 2017George MakoriNo ratings yet
- 5) Adrenal GlandDocument74 pages5) Adrenal GlandABUBEKER BESHIRNo ratings yet
- Drugs For GoutDocument29 pagesDrugs For GoutSsempijja Joshua BuyinzaNo ratings yet
- Diabetic Emergencies and ManagementDocument41 pagesDiabetic Emergencies and ManagementNali peterNo ratings yet
- Vitamins & NutritionDocument56 pagesVitamins & Nutritionahmed abd elazizNo ratings yet
- اورژانسهای متابولیک، خانم دکتر رستمپورDocument65 pagesاورژانسهای متابولیک، خانم دکتر رستمپورMehdi RowshandelNo ratings yet
- 3 - Iron Toxicity Spring 2022Document32 pages3 - Iron Toxicity Spring 2022mariamkhaledd777No ratings yet
- Fast Facts: Long-Chain Fatty Acid Oxidation Disorders for PatientsFrom EverandFast Facts: Long-Chain Fatty Acid Oxidation Disorders for PatientsNo ratings yet
- English Literature 123Document3 pagesEnglish Literature 123hassanainshahi13No ratings yet
- TAG BiosynthesisDocument4 pagesTAG Biosynthesishassanainshahi13No ratings yet
- Serum Preparation. ExperimentDocument1 pageSerum Preparation. Experimenthassanainshahi13No ratings yet
- Whey Protein: Scholars Research Journal January 2011Document11 pagesWhey Protein: Scholars Research Journal January 2011Vinay MathurNo ratings yet
- Protein DOCSDocument13 pagesProtein DOCSFRANCIS FRANCISCO. CLIMACONo ratings yet
- Protein Hydrolysates, Myogenia 2016 V1.0Document11 pagesProtein Hydrolysates, Myogenia 2016 V1.0Stefanie MacherhammerNo ratings yet
- Adult Parenteral Nutrition: Harmacy Ompetency Ssessment EnterDocument16 pagesAdult Parenteral Nutrition: Harmacy Ompetency Ssessment EnterJeremy HamptonNo ratings yet
- Nutrients: Gut Microbiota, Muscle Mass and Function in Aging: A Focus On Physical Frailty and SarcopeniaDocument21 pagesNutrients: Gut Microbiota, Muscle Mass and Function in Aging: A Focus On Physical Frailty and SarcopeniaClaudia LougonNo ratings yet
- Oet Sample Reading TestDocument20 pagesOet Sample Reading TestAHMED TANJIMUL ISLAMNo ratings yet
- Protein Metab 2 Dra. SantosDocument7 pagesProtein Metab 2 Dra. SantosMelissa SalayogNo ratings yet
- Twenty Amino Acids: 2. Arginine - Arg - RDocument7 pagesTwenty Amino Acids: 2. Arginine - Arg - RSharizzaSumbingNo ratings yet
- Jurnal YuniDocument10 pagesJurnal YuniRahmilia Alifa PutriNo ratings yet
- Waterbury Diet PDFDocument26 pagesWaterbury Diet PDFrobert allenNo ratings yet
- Krista 2009Document9 pagesKrista 2009Vanessa BarrosNo ratings yet
- Beginner's GuideONLINE PDFDocument10 pagesBeginner's GuideONLINE PDFWayne TaylorNo ratings yet
- Kidney Tissue Targeted Metabolic Profiling of Unilateral Ureteral Obstruction Rats by NMRDocument12 pagesKidney Tissue Targeted Metabolic Profiling of Unilateral Ureteral Obstruction Rats by NMRkmdfwkefmNo ratings yet
- Whey Protein Meta AnáliseDocument14 pagesWhey Protein Meta AnáliseDaniela OliveiraNo ratings yet
- 8 Proven Bodybuilding Supplements For Muscle Growth and StrengthDocument5 pages8 Proven Bodybuilding Supplements For Muscle Growth and StrengthArjunRj WorldNo ratings yet
- HNF 41 Exer 7 JamisonDocument16 pagesHNF 41 Exer 7 JamisonJohn Bryan JamisonNo ratings yet
- Group 2 ProteinsDocument30 pagesGroup 2 ProteinslaarnieNo ratings yet
- Adult Nutritional Implications of Maple Syrup Urine DiseaseDocument50 pagesAdult Nutritional Implications of Maple Syrup Urine Diseaseapi-360120287No ratings yet
- ChankoDocument9 pagesChankoPauloCarvalhoNo ratings yet
- Liver Care Hepstan Protein PowderDocument14 pagesLiver Care Hepstan Protein Powderriya chileNo ratings yet
- UltrarunningDocument60 pagesUltrarunningLynseyNo ratings yet
- Disorders of Amino Acid Metabolism and TransportDocument94 pagesDisorders of Amino Acid Metabolism and TransportfakhribabikerNo ratings yet
- PQ 0403001990Document6 pagesPQ 0403001990Yuwono WibowoNo ratings yet