You might also like
- Fast Facts: Cholangiocarcinoma: Diagnostic and therapeutic advances are improving outcomesFrom EverandFast Facts: Cholangiocarcinoma: Diagnostic and therapeutic advances are improving outcomesNo ratings yet
- Cystic Neoplasm and Endocrine Tumors of Pancreas: Presenter: Dr. Fuzail Ahmad Guide: Dr. Ravishankar N. Dr. Benak SDocument50 pagesCystic Neoplasm and Endocrine Tumors of Pancreas: Presenter: Dr. Fuzail Ahmad Guide: Dr. Ravishankar N. Dr. Benak Sbenak shivalingappaNo ratings yet
- Salivary Gland Cancer: From Diagnosis to Tailored TreatmentFrom EverandSalivary Gland Cancer: From Diagnosis to Tailored TreatmentLisa LicitraNo ratings yet
- Cystic Tumors of PancreasDocument140 pagesCystic Tumors of PancreasPooja BappannaNo ratings yet
- Thyroid TumoursDocument106 pagesThyroid TumoursJodene Rose RojasNo ratings yet
- Cytology IPQsDocument342 pagesCytology IPQsDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Cystic Neoplasm and Endocrine Tumors of Pancreas: Presenter: Dr. Fuzail Ahmad Guide: Dr. Ravishankar N. Dr. Benak SDocument53 pagesCystic Neoplasm and Endocrine Tumors of Pancreas: Presenter: Dr. Fuzail Ahmad Guide: Dr. Ravishankar N. Dr. Benak Sbenak shivalingappaNo ratings yet
- Salivaryglandtumors 150912063235 Lva1 App6892Document213 pagesSalivaryglandtumors 150912063235 Lva1 App6892Waqas IqbalNo ratings yet
- 3 Male Genital and KidneyDocument126 pages3 Male Genital and Kidneyindriana sariNo ratings yet
- Breast CytologyDocument34 pagesBreast Cytologypooo800% (1)
- Cystic LesionsDocument101 pagesCystic LesionsKartik GuptaNo ratings yet
- NeoplasiaDocument70 pagesNeoplasiaNestly QuerubinNo ratings yet
- Thyroid Neoplasm - Part 02 - Associate Prof DR Kishore G BanerjeeDocument24 pagesThyroid Neoplasm - Part 02 - Associate Prof DR Kishore G Banerjeenaveenarageson4No ratings yet
- Pancreas: 1. Congenital Anomalies of Pancreas. 2. Pancreatic Cysts. 3. Acute and Chronic Pancreatitis. 4. Pancreatic CancerDocument31 pagesPancreas: 1. Congenital Anomalies of Pancreas. 2. Pancreatic Cysts. 3. Acute and Chronic Pancreatitis. 4. Pancreatic Cancerjwan ahmedNo ratings yet
- Salivary gland cytology guideDocument30 pagesSalivary gland cytology guidePatrick BayuNo ratings yet
- NEOPLASIADocument70 pagesNEOPLASIARose de DiosNo ratings yet
- The Liver: Dr. I Made Naris Pujawan, M.Biomed, SP - PADocument19 pagesThe Liver: Dr. I Made Naris Pujawan, M.Biomed, SP - PAAnonymous D29e00No ratings yet
- PECOMADocument25 pagesPECOMAAnan JaiswalNo ratings yet
- Recent Advances in Classification of Renal TumorsDocument60 pagesRecent Advances in Classification of Renal TumorsTasleem AslamNo ratings yet
- Papillary CarcinomaDocument7 pagesPapillary Carcinomarazik89No ratings yet
- Gastric TypeDocument4 pagesGastric TypeleartaNo ratings yet
- Other TypesDocument17 pagesOther TypesJuan Maurencius CastleNo ratings yet
- Carcinoma InsituDocument46 pagesCarcinoma InsituminnalesriNo ratings yet
- Resident Short Reviews: Adenocarcinoma of the Urinary BladderDocument5 pagesResident Short Reviews: Adenocarcinoma of the Urinary BladdererikafebriyanarNo ratings yet
- Kista PankreasDocument16 pagesKista PankreasNur Islah AgustiNo ratings yet
- 4 IntestineDocument15 pages4 IntestinemyarjddbzNo ratings yet
- CNP - AjDocument33 pagesCNP - AjeviltohuntNo ratings yet
- Cytology of Fna of The BreastDocument11 pagesCytology of Fna of The BreastSara VinamdNo ratings yet
- Dr. YENITA's guide to gastrointestinal tumors and lesionsDocument108 pagesDr. YENITA's guide to gastrointestinal tumors and lesionsRaisa DilaNo ratings yet
- Spleen AnatomyDocument74 pagesSpleen AnatomysaadNo ratings yet
- Diagnosing Pleural Effusions Through CytologyDocument33 pagesDiagnosing Pleural Effusions Through CytologyAnonymous brvvLxoIluNo ratings yet
- Tumours of The Biliary System: S. Kakar, L.J. BurgartDocument10 pagesTumours of The Biliary System: S. Kakar, L.J. Burgartderek lauNo ratings yet
- Appendix 1Document2 pagesAppendix 1blablalbablablablaNo ratings yet
- Git 7 PDFDocument29 pagesGit 7 PDFafaq alismailiNo ratings yet
- Liver Tumor Types and TreatmentsDocument39 pagesLiver Tumor Types and Treatmentsinstagram googleNo ratings yet
- Clinical Case CAPDocument82 pagesClinical Case CAPIna GargNo ratings yet
- 1 s2.0 S0011384010000377 MainDocument52 pages1 s2.0 S0011384010000377 MainAlberto Castillo SanchezNo ratings yet
- Carcinoma Gall BladderDocument25 pagesCarcinoma Gall Bladderrajan kumarNo ratings yet
- Diseases of Female Reproductive SystemDocument13 pagesDiseases of Female Reproductive SystemSalon LamichhaneNo ratings yet
- Nada's GI Path ReviewDocument44 pagesNada's GI Path ReviewNada Much100% (2)
- Pathology of Liver, Colon, and Oral Cavity LesionsDocument13 pagesPathology of Liver, Colon, and Oral Cavity LesionsdiahNo ratings yet
- Colorectal CancerDocument68 pagesColorectal Cancerjack sawda100% (1)
- Cytology 2Document30 pagesCytology 2okonkwojohnchuks1No ratings yet
- Diseases of the urinary system: kidney and bladder disordersDocument71 pagesDiseases of the urinary system: kidney and bladder disordersArsy Mira PertiwiNo ratings yet
- T5 Pancreas PDFDocument19 pagesT5 Pancreas PDFAmin ZahariNo ratings yet
- 3rd Stage Liver Diseases (2) - HMUDocument31 pages3rd Stage Liver Diseases (2) - HMUjwan ahmedNo ratings yet
- gastrointestinal polyps pgDocument36 pagesgastrointestinal polyps pgharish kumarNo ratings yet
- Cervical Cancer & Abnormalities GuideDocument75 pagesCervical Cancer & Abnormalities GuideShaimaa DawaNo ratings yet
- Benign Lesion Mimicking Malignant Breast LesionDocument82 pagesBenign Lesion Mimicking Malignant Breast Lesionachmad rizkiNo ratings yet
- 1 Tmu - JD - 039Document4 pages1 Tmu - JD - 039Hasan BlackNo ratings yet
- 1 Tmu - JD - 039 PDFDocument4 pages1 Tmu - JD - 039 PDFKristina SabuNo ratings yet
- Mucinous Cystic Neoplasm PancreasDocument44 pagesMucinous Cystic Neoplasm PancreasBensy IsaacNo ratings yet
- Slide 15 Diseases of Salivary Glands IIDocument64 pagesSlide 15 Diseases of Salivary Glands IIJustDen09100% (1)
- Non Urothelial Carcinoma of BladderDocument15 pagesNon Urothelial Carcinoma of BladderAida EsmeronNo ratings yet
- Kidney & Urothelial TumoursDocument74 pagesKidney & Urothelial Tumoursjames20123No ratings yet
- Chapter 9Document155 pagesChapter 9Kw ChanNo ratings yet
- PENCERNAANDocument25 pagesPENCERNAANMekki Lazir IlhdafNo ratings yet
- ABDOMINAL AND PELVIC MASSES IN PEDIATRICS - Level 4Document26 pagesABDOMINAL AND PELVIC MASSES IN PEDIATRICS - Level 4Malueth AnguiNo ratings yet
- Powerpoint: Colorectal Polyps and Colorectal CarcinomaDocument68 pagesPowerpoint: Colorectal Polyps and Colorectal Carcinomaj.doe.hex_87100% (5)
- Eosinophilic Solid and Cystic Renal Cell Carcinoma (ESC RCC)Document6 pagesEosinophilic Solid and Cystic Renal Cell Carcinoma (ESC RCC)Aswathy MiriamNo ratings yet
- In The Matter of The Adoption of Elizabeth MiraDocument2 pagesIn The Matter of The Adoption of Elizabeth MiradelayinggratificationNo ratings yet
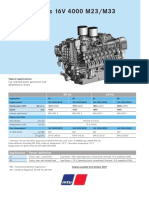
- Diesel Engines 16V 4000 M23/M33: 50 HZ 60 HZDocument2 pagesDiesel Engines 16V 4000 M23/M33: 50 HZ 60 HZAlberto100% (1)
- EASE Module 1 Geometric RelationsDocument26 pagesEASE Module 1 Geometric RelationsMarlon MiclatNo ratings yet
- Coleção Bernoulli Ensino Médio 2020 - 100% BNCC by Bernoulli Sistema de Ensino - IssuuDocument1 pageColeção Bernoulli Ensino Médio 2020 - 100% BNCC by Bernoulli Sistema de Ensino - IssuuVitor OliveiraNo ratings yet
- Lesson Plans by Noman Niaz MaharDocument3 pagesLesson Plans by Noman Niaz MaharNoman Niaz 13No ratings yet
- Abnormal Psychology Unit IDocument14 pagesAbnormal Psychology Unit IMahadevan K V100% (1)
- Elitox PPT ENG CompressedDocument18 pagesElitox PPT ENG CompressedTom ArdiNo ratings yet
- Report On Foundations For Dynamic Equipment: Reported by ACI Committee 351Document14 pagesReport On Foundations For Dynamic Equipment: Reported by ACI Committee 351Erick Quan LunaNo ratings yet
- Parking Garage Design GuidelinesDocument17 pagesParking Garage Design GuidelinesCarlos Benjamin BCNo ratings yet
- Ap Finance Go PDFDocument3 pagesAp Finance Go PDFSuresh Babu ChinthalaNo ratings yet
- Are The Risk Management Tools at Your Law Firm Working?Document17 pagesAre The Risk Management Tools at Your Law Firm Working?vantoffNo ratings yet
- Science in VedasDocument42 pagesScience in VedasPratyush NahakNo ratings yet
- Create Sales Order (Bapi - Salesorder - Createfromdat2) With Bapi Extension2Document5 pagesCreate Sales Order (Bapi - Salesorder - Createfromdat2) With Bapi Extension2raky03690% (1)
- Labor Law 1 Class NotesDocument20 pagesLabor Law 1 Class Notescmv mendozaNo ratings yet
- Test Bank For American Pageant Volume 1 16th EditionDocument36 pagesTest Bank For American Pageant Volume 1 16th Editionzoonwinkfoxyj8100% (48)
- BS KashmiryatDocument67 pagesBS KashmiryatWaqas AhmedNo ratings yet
- Protective & Marine Coatings: Hi-Solids Alkyd Metal PrimerDocument4 pagesProtective & Marine Coatings: Hi-Solids Alkyd Metal PrimerAna CabreraNo ratings yet
- The Definition and Unit of Ionic StrengthDocument2 pagesThe Definition and Unit of Ionic StrengthDiego ZapataNo ratings yet
- Samsung C&T AuditDocument104 pagesSamsung C&T AuditkevalNo ratings yet
- Time To Get SeriousDocument354 pagesTime To Get SeriousEdmond Blair100% (1)
- Geraldez Vs Ca 230 Scra 329Document12 pagesGeraldez Vs Ca 230 Scra 329Cyrus Pural EboñaNo ratings yet
- Registration Form Proficiency Testing Program: Name Designation Mob. / Tel. NoDocument4 pagesRegistration Form Proficiency Testing Program: Name Designation Mob. / Tel. NoOwais Manzoor MalikNo ratings yet
- OOD ch11Document31 pagesOOD ch11Pumapana GamingNo ratings yet
- 6 Fsiqiatria-1524041346Document48 pages6 Fsiqiatria-1524041346მირანდა გიორგაშვილიNo ratings yet
- Lead and Manage Team Effectiveness for BSBWOR502Document38 pagesLead and Manage Team Effectiveness for BSBWOR502roopaNo ratings yet
- Using Facebook Groups To Support Teachers' Professional DevelopmentDocument22 pagesUsing Facebook Groups To Support Teachers' Professional DevelopmentLilmal SihamNo ratings yet
- Dell in India Targeting SMB Markets - The Differentiation Strategy PDFDocument16 pagesDell in India Targeting SMB Markets - The Differentiation Strategy PDFJatinNo ratings yet
- UTH homework template for English exercisesDocument8 pagesUTH homework template for English exercisesCinthya Peña de MezaNo ratings yet
- 3.part I-Foundations of Ed (III)Document25 pages3.part I-Foundations of Ed (III)Perry Arcilla SerapioNo ratings yet
- PCC 3300 PDFDocument6 pagesPCC 3300 PDFdelangenico4No ratings yet