You might also like
- Drug NeurontinDocument1 pageDrug NeurontinSrkocher100% (2)
- Stephan Heckers Catatonia 2023Document6 pagesStephan Heckers Catatonia 2023kendoca23No ratings yet
- Geriatrics 2023 FinalDocument119 pagesGeriatrics 2023 FinalBelinda ELISHANo ratings yet
- Behavioral Health Care PlanDocument10 pagesBehavioral Health Care Planapi-520664738No ratings yet
- Behavioral Health Care PlanDocument12 pagesBehavioral Health Care Planapi-520841770100% (1)
- Mental StatusDocument6 pagesMental StatusIgor Oliveira100% (1)
- Anthony Holland - PWSRomaniaOct2010 (Final2)Document20 pagesAnthony Holland - PWSRomaniaOct2010 (Final2)elutafNo ratings yet
- Meadows Paige Case StudyDocument16 pagesMeadows Paige Case Studyapi-607727110No ratings yet
- Delirious Mania - An Approach To Diagnosis and TreatmentDocument10 pagesDelirious Mania - An Approach To Diagnosis and TreatmentJaviera Paz Guerrero CassanelloNo ratings yet
- CASE Study SampleDocument6 pagesCASE Study SampleMary Shane Aragon MoraldeNo ratings yet
- Agot Rle Case Study 3Document17 pagesAgot Rle Case Study 3Angel May P AgotNo ratings yet
- Diagnosis Schizophrenia 2Document1 pageDiagnosis Schizophrenia 2Bukola OgunnaikeNo ratings yet
- Clinical and Neurologic Manifestation of Minimal Hepatic Encephalopathy and Overt Hepatic Encephalopathy - 2015 - Clinics in Liver DiseaseDocument12 pagesClinical and Neurologic Manifestation of Minimal Hepatic Encephalopathy and Overt Hepatic Encephalopathy - 2015 - Clinics in Liver DiseasecarolinapolotorresNo ratings yet
- 2011 Updates in Therapeutics: P P: The Pharmacotherapy Preparatory Review and Recertification CourseDocument11 pages2011 Updates in Therapeutics: P P: The Pharmacotherapy Preparatory Review and Recertification CourseDrx ahmed MaherNo ratings yet
- The Evaluation of A Patient With Dizziness - FullDocument11 pagesThe Evaluation of A Patient With Dizziness - Fullnatalia.gallinoNo ratings yet
- Delirium Pathway - OTLPCM002-3Document1 pageDelirium Pathway - OTLPCM002-3Iftida YatiNo ratings yet
- Phobic Postural Vertigo: A Cognitive-Behavior ApproachDocument2 pagesPhobic Postural Vertigo: A Cognitive-Behavior ApproachVa RissaNo ratings yet
- 3-Anxiety DisordersDocument57 pages3-Anxiety DisordersVidya BalaNo ratings yet
- 1.2 Overview & OutcomesDocument9 pages1.2 Overview & OutcomesShayla HudsonNo ratings yet
- DocumentDocument11 pagesDocumentFairuds MamalintaNo ratings yet
- Antidepressant Discontinuation SyndromeDocument26 pagesAntidepressant Discontinuation SyndromeDevi DamayantiNo ratings yet
- Practice A Mental HDocument1 pagePractice A Mental HroNo ratings yet
- Schizophrenia and Other Psychotic DisordersDocument32 pagesSchizophrenia and Other Psychotic DisordersAjeng Aristiany RahawarinNo ratings yet
- ScienceDocument3 pagesScienceAmal DavisNo ratings yet
- Psychosis and Seizure Disorder: Challenges in Diagnosis and TreatmentDocument7 pagesPsychosis and Seizure Disorder: Challenges in Diagnosis and TreatmentgreenanubisNo ratings yet
- Haloperidol PDFDocument1 pageHaloperidol PDFAda AlvarezNo ratings yet
- DR - Nuha Alshammari Consultant Psychiatrist: First Episode Psychosis/Youth Crisis ManagementDocument46 pagesDR - Nuha Alshammari Consultant Psychiatrist: First Episode Psychosis/Youth Crisis ManagementaliNo ratings yet
- Aripiprazole For Acute Mania in An Elderly Person: Balaji Bharadwaj, Shivanand Kattimani, Anuriddha MukherjeeDocument4 pagesAripiprazole For Acute Mania in An Elderly Person: Balaji Bharadwaj, Shivanand Kattimani, Anuriddha MukherjeeMay GaamNo ratings yet
- When Psychiatric Symptoms Re Ect Medical Conditions: Authors: Killian A WelchDocument8 pagesWhen Psychiatric Symptoms Re Ect Medical Conditions: Authors: Killian A WelchEkachaeryanti ZainNo ratings yet
- Delirium and DementiaDocument12 pagesDelirium and DementiaSNo ratings yet
- Huntington DiseaseDocument2 pagesHuntington DiseaseAlly JuanezaNo ratings yet
- Depression in The ElderlyDocument24 pagesDepression in The ElderlyagguzmanNo ratings yet
- Unit 5 Neurotic DDocument24 pagesUnit 5 Neurotic Dreeta yadavNo ratings yet
- NCM 105 Rle Case 1 BasigDocument17 pagesNCM 105 Rle Case 1 BasigMaria Charis Anne IndananNo ratings yet
- Dosi 2014Document4 pagesDosi 2014Neurobites ESLNo ratings yet
- Psychopharmacologic Agents Lec 2016Document23 pagesPsychopharmacologic Agents Lec 2016roseanne_erikaNo ratings yet
- 17-Delirium DementiaDocument34 pages17-Delirium DementiaNada EhabNo ratings yet
- Huntington DiseaseDocument2 pagesHuntington DiseaseAlly JuanezaNo ratings yet
- CM Alzheimer's Disease SantosDocument1 pageCM Alzheimer's Disease SantosKyle SantosNo ratings yet
- Comatose PatientDocument11 pagesComatose PatientUWIMANA Jean ClaudeNo ratings yet
- (PSYCH) Neurocognitive DisordersDocument14 pages(PSYCH) Neurocognitive DisordersThesa TagalogNo ratings yet
- Principles of Seizure ManagementDocument119 pagesPrinciples of Seizure ManagementRenan Toledo SandaloNo ratings yet
- Fresh Test For December 2016 (Test 7)Document26 pagesFresh Test For December 2016 (Test 7)Kanaga6432No ratings yet
- Behavioral Health Care PlanDocument9 pagesBehavioral Health Care Planapi-520634647No ratings yet
- Acute Polymorphic Psychotic Disorder With Symptoms of SchizophreniaDocument4 pagesAcute Polymorphic Psychotic Disorder With Symptoms of SchizophreniadysphileNo ratings yet
- Psych Case StudyDocument13 pagesPsych Case Studyapi-736869233No ratings yet
- Altered Mental Status During Critical Illness: Delirium and ComaDocument8 pagesAltered Mental Status During Critical Illness: Delirium and ComantnquynhproNo ratings yet
- ALZHEIMERDocument2 pagesALZHEIMERLorelyn Santos CorpuzNo ratings yet
- The Minimally Conscious State: Definition and Diagnostic CriteriaDocument7 pagesThe Minimally Conscious State: Definition and Diagnostic CriteriadonnyawNo ratings yet
- Dementia & DeliriumDocument7 pagesDementia & DeliriumSudesna Roy ChowdhuryNo ratings yet
- Diseases: Delirium Assessment in Older People in Emergency Departments. A Literature ReviewDocument12 pagesDiseases: Delirium Assessment in Older People in Emergency Departments. A Literature ReviewChika SabaNo ratings yet
- Dementia Vs Delirium HandoutDocument2 pagesDementia Vs Delirium HandoutnvifNo ratings yet
- Dissociative Identity Disorder A Case of Three SelDocument2 pagesDissociative Identity Disorder A Case of Three SelMartín SalamancaNo ratings yet
- Stability Indicating RP-HPLC Method Development and Validation For Estimation of Tiagabine Hydrochloride in TabletDocument26 pagesStability Indicating RP-HPLC Method Development and Validation For Estimation of Tiagabine Hydrochloride in TabletBaru Chandrasekhar RaoNo ratings yet
- برزنتيشن هديك١Document22 pagesبرزنتيشن هديك١Abdallah AlquranNo ratings yet
- Exam 1 BlueprintDocument6 pagesExam 1 BlueprintMindiNo ratings yet
- Case Study - Izabella WertzDocument11 pagesCase Study - Izabella Wertzapi-663559916No ratings yet
- Cerebral Palsy: Signs & Symptoms / Pathophysiology / Drug Studies / Ncps / Health TeachingsDocument22 pagesCerebral Palsy: Signs & Symptoms / Pathophysiology / Drug Studies / Ncps / Health TeachingsGeoffrey Sintaan RiveraNo ratings yet
- Nelson en Ingles Capitulos 16 A 20Document81 pagesNelson en Ingles Capitulos 16 A 20Mario TurichNo ratings yet
- Final Paper - CBT and SchizophreniaDocument14 pagesFinal Paper - CBT and Schizophreniatanis.payneNo ratings yet
- A Randomized Multicenter Trial On A Lung Ultrasound-Guided Treatment Strategy in Patients On Chronic Hemodialysis With High Cardiovascular RiskDocument9 pagesA Randomized Multicenter Trial On A Lung Ultrasound-Guided Treatment Strategy in Patients On Chronic Hemodialysis With High Cardiovascular RiskMarco Antonio Viera ArevaloNo ratings yet
- MCQS CNS PathologyDocument14 pagesMCQS CNS PathologyFourth YearNo ratings yet
- Newborn ScreeningDocument2 pagesNewborn ScreeningMercy Anne EcatNo ratings yet
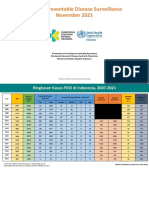
- 11 - VPD Surveillance Performance Analysis 2021 November 2021 (29122021)Document57 pages11 - VPD Surveillance Performance Analysis 2021 November 2021 (29122021)Kiky RizkyNo ratings yet
- NCM106-Cellular Aberrations-Module1-Lesson 1Document9 pagesNCM106-Cellular Aberrations-Module1-Lesson 1Esmareldah Henry SirueNo ratings yet
- Group 2 DkaDocument59 pagesGroup 2 DkaAkio OzaragaNo ratings yet
- Hearing Impairment by Nyanga KeyDocument4 pagesHearing Impairment by Nyanga KeyMbuyoti KanyataNo ratings yet
- RhabdomyosarcomaDocument2 pagesRhabdomyosarcomaLoti MarcNo ratings yet
- Report-220116000181081 Mrs - SAHILIKHARADE 21sep2022 102232Document2 pagesReport-220116000181081 Mrs - SAHILIKHARADE 21sep2022 102232Ajinkya kasarNo ratings yet
- 05 - 2.7 - Cell Division Gone Wrong - Cancer - ANSWERSDocument20 pages05 - 2.7 - Cell Division Gone Wrong - Cancer - ANSWERSVicky UngariuddanieNo ratings yet
- SMA Bahasa Inggris 11 Summative AssessmentDocument9 pagesSMA Bahasa Inggris 11 Summative Assessmentalberthoal588No ratings yet
- Acute Lymphoblastic Leukemia - UERM Aug 16-31Document40 pagesAcute Lymphoblastic Leukemia - UERM Aug 16-31TeresaNo ratings yet
- Epidemiology ReportDocument76 pagesEpidemiology Reportjammy malanaNo ratings yet
- Checklist Communication SkillsDocument4 pagesChecklist Communication SkillsKaruna Sree PNo ratings yet
- Prevalence of Developmental DysplasiaDocument7 pagesPrevalence of Developmental DysplasiaAdrian SanduNo ratings yet
- Delayed Sleep Phase SyndromeDocument2 pagesDelayed Sleep Phase SyndromeAbubakar BusatiNo ratings yet
- Pro-Choice Violence in VirginiaDocument11 pagesPro-Choice Violence in VirginiaHuman Life InternationalNo ratings yet
- INFLAMATORY AND STDsDocument26 pagesINFLAMATORY AND STDsNathaniel BudayNo ratings yet
- Assessment of Older Adults Powerpoint Rebecca WinsorDocument19 pagesAssessment of Older Adults Powerpoint Rebecca WinsorRose Antonette BenitoNo ratings yet
- Cancer NotesDocument6 pagesCancer NotesRocco WalksNo ratings yet
- Alliance For Childhood Cancer Gabriella Miller Kids First 2.0 Letter of SupportDocument2 pagesAlliance For Childhood Cancer Gabriella Miller Kids First 2.0 Letter of SupportAndrew KaczynskiNo ratings yet
- Does Metformin Raise Cholesterol Levels - DIQDocument2 pagesDoes Metformin Raise Cholesterol Levels - DIQFathima Sheik KatherNo ratings yet
- Rahul-Protocol-v0 1 1Document30 pagesRahul-Protocol-v0 1 1ElroyNo ratings yet
- Factsheet On Gender and Family Violence: Relevant StatisticsDocument3 pagesFactsheet On Gender and Family Violence: Relevant StatisticsReuben DylanNo ratings yet
- IMRT & Stereotactic Radiotherapy: Christopher GolbyDocument41 pagesIMRT & Stereotactic Radiotherapy: Christopher GolbyAmr MuhammedNo ratings yet
- Tren Tata Laksana Kanker Prostat PDFDocument18 pagesTren Tata Laksana Kanker Prostat PDFShannia FrnsNo ratings yet
- Instructions For Use Before Using: Buprenorphine/nalox 8mg/2mg SL TabDocument5 pagesInstructions For Use Before Using: Buprenorphine/nalox 8mg/2mg SL TabPhilipNo ratings yet
- Wk7 IhumanDocument8 pagesWk7 IhumanPesh B NimmoNo ratings yet
- Diabetic Foot Ulcer - StatPearls - NCBI BookshelfDocument8 pagesDiabetic Foot Ulcer - StatPearls - NCBI BookshelfIsna SalisNo ratings yet