You might also like
- Hepatitis C Virus-Host Interactions and Therapeutics: Current Insights and Future PerspectivesFrom EverandHepatitis C Virus-Host Interactions and Therapeutics: Current Insights and Future PerspectivesNo ratings yet
- Recent Advance of Chronic Hepatitis B TreatmentDocument28 pagesRecent Advance of Chronic Hepatitis B Treatmentbudi darmantaNo ratings yet
- Fast Facts: Peripheral T-cell Lymphoma: Unraveling the complexities of diagnosis and managementFrom EverandFast Facts: Peripheral T-cell Lymphoma: Unraveling the complexities of diagnosis and managementNo ratings yet
- Update On MGT of Hepatitis B and CDocument57 pagesUpdate On MGT of Hepatitis B and Cadamu mohammadNo ratings yet
- Hepatitis B Virus and Hepatitis C Virus Co-Infection With HIVDocument54 pagesHepatitis B Virus and Hepatitis C Virus Co-Infection With HIVShree Narayan YadavNo ratings yet
- Clinical Resource Viral HepatitisDocument51 pagesClinical Resource Viral HepatitisDura EbrahimNo ratings yet
- Viral Hepatitis 2015Document54 pagesViral Hepatitis 2015Abdulziz Al-jedaieNo ratings yet
- Prezentare ClujDocument64 pagesPrezentare ClujAndreea IrimiaNo ratings yet
- Optimization of ART RegimenDocument81 pagesOptimization of ART RegimenMigori Art100% (1)
- HCV diagnostic and health care worker managementDocument36 pagesHCV diagnostic and health care worker managementLaboratorium Ansari SalehNo ratings yet
- Research ArticleDocument7 pagesResearch ArticlentnquynhproNo ratings yet
- Chronic Hepatitis B - New Goals, New Treatment: Ching-Lung Lai, M.D., and Man-Fung Yuen, M.DDocument4 pagesChronic Hepatitis B - New Goals, New Treatment: Ching-Lung Lai, M.D., and Man-Fung Yuen, M.DSofara RezantiNo ratings yet
- Viral Hepatitis Clinical CorrelationDocument59 pagesViral Hepatitis Clinical Correlationdrhananfathy100% (3)
- Acute & Chronic HepatitisDocument65 pagesAcute & Chronic HepatitisMahmoud AjinehNo ratings yet
- Jurnal Ebm PDFDocument10 pagesJurnal Ebm PDFagustin488No ratings yet
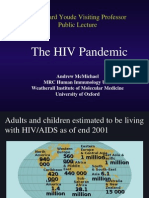
- The HIV Pandemic: Sir Edward Youde Visiting Professor Public LectureDocument50 pagesThe HIV Pandemic: Sir Edward Youde Visiting Professor Public LectureSanthosh SubramanianNo ratings yet
- Resistance in HCV: Andrew J. Muir, MD MHSDocument33 pagesResistance in HCV: Andrew J. Muir, MD MHSEleni HagosNo ratings yet
- VIRAL HEPATITIS IN PREGNANCY copy 1Document48 pagesVIRAL HEPATITIS IN PREGNANCY copy 1EndaleNo ratings yet
- Hepatitis B The Basics: David Wong University of Toronto March 2005Document36 pagesHepatitis B The Basics: David Wong University of Toronto March 2005Umi MazidahNo ratings yet
- Hepatitis Virus: Kurnia Dwi Artanti. Dept. of Epidemiology, Fac. of Public HealthDocument38 pagesHepatitis Virus: Kurnia Dwi Artanti. Dept. of Epidemiology, Fac. of Public Healthana fitrotulNo ratings yet
- Jose A Lavergne, M.D., F.A.C.PDocument61 pagesJose A Lavergne, M.D., F.A.C.PMarceloGuerraNo ratings yet
- Screening For Viral Hepatitis: Diagnostics (HBV and HCV) : Diana HardieDocument23 pagesScreening For Viral Hepatitis: Diagnostics (HBV and HCV) : Diana HardieWahyu PurnamaNo ratings yet
- HIV 101 and PharmacologyDocument36 pagesHIV 101 and Pharmacologyjoel contrerasNo ratings yet
- Hepatitis Viruses: VIRUS:Hepatitis A, B, CDocument25 pagesHepatitis Viruses: VIRUS:Hepatitis A, B, Carisita firmanNo ratings yet
- Management in Chronic Hepatitis B:: Interferon or Nucleoside Analogue?Document23 pagesManagement in Chronic Hepatitis B:: Interferon or Nucleoside Analogue?chaz5727xNo ratings yet
- Cobas® Taqman® HBV Test: Amplifying The PotentialDocument2 pagesCobas® Taqman® HBV Test: Amplifying The PotentialivanNo ratings yet
- HIV Topic Discussion HandoutDocument4 pagesHIV Topic Discussion HandoutMatthew LeiNo ratings yet
- 2018 Hepatitis Viral InfectionDocument51 pages2018 Hepatitis Viral Infectionkomang nickoNo ratings yet
- Hepatitis - B: Presentedby DR - Priyankamadhavan Imds Deptof Oralpathologyand MicrobiologyDocument55 pagesHepatitis - B: Presentedby DR - Priyankamadhavan Imds Deptof Oralpathologyand Microbiologydr priyankaNo ratings yet
- HCV Cure For Everyone or Which Challenges Remain?: ReviewDocument4 pagesHCV Cure For Everyone or Which Challenges Remain?: Reviewapi-206282033No ratings yet
- EntecavirDocument48 pagesEntecavirAnil RajaniNo ratings yet
- Hepatitis B: DR Tanmay Vyas (DM Hepatology)Document37 pagesHepatitis B: DR Tanmay Vyas (DM Hepatology)Sreekanth VattikondaNo ratings yet
- Zoulim 2014Document18 pagesZoulim 2014Indah LestariNo ratings yet
- ContentServer - Asp 47Document8 pagesContentServer - Asp 47TataNo ratings yet
- Tacke2016 - Treatment For Hepatitis B in Patients With Drug ResistanceDocument7 pagesTacke2016 - Treatment For Hepatitis B in Patients With Drug ResistanceClarisa AnindyaNo ratings yet
- Heaptobiliary Disease by Lecturio.Document106 pagesHeaptobiliary Disease by Lecturio.louisegantierNo ratings yet
- 3.0HEPATIT Lecture 5Document48 pages3.0HEPATIT Lecture 5Jiya MuhammadNo ratings yet
- FTP PDFDocument5 pagesFTP PDFEltari SumbayakNo ratings yet
- Laboratory Tests To Monitor CMV Infection in Transplant PatientsDocument36 pagesLaboratory Tests To Monitor CMV Infection in Transplant PatientsmateenNo ratings yet
- HBV Infectionmain Aspects: N. Shavgulidze, MDDocument22 pagesHBV Infectionmain Aspects: N. Shavgulidze, MDRohan TejaNo ratings yet
- 10.1007@s10198 014 0653 XDocument5 pages10.1007@s10198 014 0653 XDr. Suhadi S.KM.,M.Kes.No ratings yet
- Pharmacological Management of Hepatitis CDocument62 pagesPharmacological Management of Hepatitis CWei HangNo ratings yet
- Tenofovir Associated Renal Toxicity in A Cohort of Hiv Infected Individuals in Goa - January - 2020 - 1577784624 - 0401138Document3 pagesTenofovir Associated Renal Toxicity in A Cohort of Hiv Infected Individuals in Goa - January - 2020 - 1577784624 - 0401138rfrdefNo ratings yet
- Type B hepatitis - the most common viral hepatitisDocument20 pagesType B hepatitis - the most common viral hepatitisBhupesh ChandNo ratings yet
- Antimicrob. Agents Chemother. 2010 Niesters 1283 9Document8 pagesAntimicrob. Agents Chemother. 2010 Niesters 1283 9Kiran MandapatiNo ratings yet
- Immunology 1Document9 pagesImmunology 1Alexandra Duque-DavidNo ratings yet
- Overview of Hepatitis Types A to EDocument40 pagesOverview of Hepatitis Types A to EPraveen RadhakrishnanNo ratings yet
- Bioscientific Review (BSR)Document9 pagesBioscientific Review (BSR)UMT JournalsNo ratings yet
- HBV AuditDocument5 pagesHBV AuditHatem SadekNo ratings yet
- Treatment of HCV in Persons With HIV CoinfectionDocument17 pagesTreatment of HCV in Persons With HIV CoinfectionSinziana OgrutanNo ratings yet
- Viral HepatitisDocument49 pagesViral HepatitisAster WidodoNo ratings yet
- Specific Investigations of HIV Infections 1Document15 pagesSpecific Investigations of HIV Infections 1jenny girlNo ratings yet
- Antiretroviral Therapy (ART) : When, How To Start HAART and Combination TherapiesDocument36 pagesAntiretroviral Therapy (ART) : When, How To Start HAART and Combination TherapiesMwanja MosesNo ratings yet
- Hepatitis A-E Viruses: Ini PPT DR - Catur Dari InternetDocument48 pagesHepatitis A-E Viruses: Ini PPT DR - Catur Dari InternetNurhidayahNo ratings yet
- Hepatology MRCP1Document87 pagesHepatology MRCP1Raouf Ra'fat SolimanNo ratings yet
- HIV/HCV Co-InfectionDocument23 pagesHIV/HCV Co-InfectionEleni HagosNo ratings yet
- Hepatitis A-E Viruses: An OverviewDocument48 pagesHepatitis A-E Viruses: An OverviewPrajakta TawdeNo ratings yet
- Telbivudine Versus Lamivudine in Patients With Chronic Hepatitis BDocument13 pagesTelbivudine Versus Lamivudine in Patients With Chronic Hepatitis BOkim NawarNo ratings yet
- Khubaib 2015Document21 pagesKhubaib 2015Thanh PhongNo ratings yet
- Highly Active Antiretroviral Therapy Associated.7Document5 pagesHighly Active Antiretroviral Therapy Associated.7FrancescFranquesaNo ratings yet
- Homeopathic First Aid For Infants and Children PDFDocument3 pagesHomeopathic First Aid For Infants and Children PDFRamesh Shah100% (1)
- Welcome - Embrace QuoteEngineDocument3 pagesWelcome - Embrace QuoteEnginegabyNo ratings yet
- Media Bulletin 03 09 21 COVID 19Document17 pagesMedia Bulletin 03 09 21 COVID 19Ram KrishnanNo ratings yet
- General School Operations: 118.01 1 Updated 19 20 Wis. StatsDocument76 pagesGeneral School Operations: 118.01 1 Updated 19 20 Wis. Statsapi-271033247No ratings yet
- Intellectual DiabilityDocument10 pagesIntellectual DiabilityAngelo PapimNo ratings yet
- Pharmaceutical Packing - A Growing PhenomenaDocument18 pagesPharmaceutical Packing - A Growing PhenomenaSiddharth SikariaNo ratings yet
- Paediatric Radiography DissertationDocument4 pagesPaediatric Radiography DissertationGhostWriterCollegePapersHartford100% (1)
- Kidney Treatment Guidelines For HyponatremiaDocument7 pagesKidney Treatment Guidelines For HyponatremialguerreroNo ratings yet
- REPORT - Crossroads of People - Place - ProsperityDocument57 pagesREPORT - Crossroads of People - Place - ProsperityVeny KimNo ratings yet
- EmpyemaDocument9 pagesEmpyemaJoePutraNo ratings yet
- Kursus Asas Minda Sihat Zon PuduDocument65 pagesKursus Asas Minda Sihat Zon PuduslevsterNo ratings yet
- Paediatric Consumer Health in IndiaDocument8 pagesPaediatric Consumer Health in IndiaAkash GuruNo ratings yet
- Research InstrumentDocument3 pagesResearch InstrumentMark Warren Atienza RevellameNo ratings yet
- Sids PresentationDocument10 pagesSids Presentationapi-257403826No ratings yet
- EUTHANASIADocument2 pagesEUTHANASIAMariaSNo ratings yet
- The Architecture of Hospitals ConferenceDocument6 pagesThe Architecture of Hospitals ConferenceJavier SiñaniNo ratings yet
- Physiological Peculiarities, Vices, Senses, and Behaviour of HorsesDocument13 pagesPhysiological Peculiarities, Vices, Senses, and Behaviour of HorsesSantosh RajaNo ratings yet
- Adoption Issues Young Children Face DevelopmentallyDocument6 pagesAdoption Issues Young Children Face DevelopmentallyNurfaradilla NasriNo ratings yet
- Module 6 - Sexual SelfDocument14 pagesModule 6 - Sexual SelfFlorence de LeonNo ratings yet
- Manifestations of ViolenceDocument2 pagesManifestations of ViolenceProjectSakinahDCNo ratings yet
- Interpretation MRCPCH 2009 Site: For Part 2 Exam For Part 2 ExamDocument35 pagesInterpretation MRCPCH 2009 Site: For Part 2 Exam For Part 2 Examyassine100% (1)
- Ehlers-Danlos Syndromes (EDS) : Fiona Li Pharm D Candidate University of Saint Joseph School of PharmacyDocument22 pagesEhlers-Danlos Syndromes (EDS) : Fiona Li Pharm D Candidate University of Saint Joseph School of PharmacyDiogo CapellaNo ratings yet
- EMBRYOLOGYDocument4 pagesEMBRYOLOGYbhagavan prasadNo ratings yet
- AURELIO-Issues, Trends and Challenges On The Care of Older Persons in The Different SettingsDocument14 pagesAURELIO-Issues, Trends and Challenges On The Care of Older Persons in The Different Settings3D - AURELIO, Lyca Mae M.0% (1)
- 2016 Work and Wellbeing Survey ResultsDocument51 pages2016 Work and Wellbeing Survey ResultsHutami PutriNo ratings yet
- Big DataDocument156 pagesBig DatalidieskaNo ratings yet
- Raisya Edlim 2313201037Document2 pagesRaisya Edlim 2313201037mas.aji.fatahillah.tm23No ratings yet
- Operator Handbook Red Team Osint Blue Team Reference V10nbsped 9798605493952Document443 pagesOperator Handbook Red Team Osint Blue Team Reference V10nbsped 9798605493952harshamlNo ratings yet
- Bma Specialty Doctor Specialist and Consultant Roles and Responsibilities Comparison Table Jul 2021Document1 pageBma Specialty Doctor Specialist and Consultant Roles and Responsibilities Comparison Table Jul 2021Shahab AnsariNo ratings yet
- Introduction To The Principles of Food Hygiene and SafetyDocument15 pagesIntroduction To The Principles of Food Hygiene and SafetyYasiqyhaidarNo ratings yet