
You might also like
- Cairns 2006Document12 pagesCairns 2006David LorencNo ratings yet
- Test Exercitii SpondiDocument9 pagesTest Exercitii Spondipanaghia.marian.17No ratings yet
- Lopes 2017Document7 pagesLopes 2017alonsoNo ratings yet
- 10 1097@JWH 0000000000000102Document11 pages10 1097@JWH 0000000000000102Winda YaniNo ratings yet
- Jurnal 3Document31 pagesJurnal 3Putra Muhammad HNo ratings yet
- Effectiveness of Core Stabilization Exercises and Routine Exercise Therapy in Management of Pain in Chronic Non-Specific Low Back Pain A Randomized Controlled Clinical Trial PDFDocument5 pagesEffectiveness of Core Stabilization Exercises and Routine Exercise Therapy in Management of Pain in Chronic Non-Specific Low Back Pain A Randomized Controlled Clinical Trial PDFFelipe solis jimenez100% (1)
- Aluko2013 2Document11 pagesAluko2013 2Dr Ahmed NabilNo ratings yet
- Taise Angeli Boff, Fernanda Pasinato, Ângela Jornada Ben, Judith E. Bosmans, Maurits Van Tulder, Rodrigo Luiz CarregaroDocument10 pagesTaise Angeli Boff, Fernanda Pasinato, Ângela Jornada Ben, Judith E. Bosmans, Maurits Van Tulder, Rodrigo Luiz CarregaroNaomiNo ratings yet
- Journal ComparedDocument4 pagesJournal ComparedRisalah Al KhaerNo ratings yet
- KTversusmicropore, BJPT2015Document9 pagesKTversusmicropore, BJPT2015Ju ChangNo ratings yet
- Jurnal CCFTDocument8 pagesJurnal CCFTfi.afifah NurNo ratings yet
- Hipopresivos y Dolor Lumbar Cronico 2021Document9 pagesHipopresivos y Dolor Lumbar Cronico 2021klgarivasNo ratings yet
- RPG Na Recuperação de Pacientes Com Cervicalgia PDFDocument9 pagesRPG Na Recuperação de Pacientes Com Cervicalgia PDFHildemar ShirataNo ratings yet
- Satpute 2018Document9 pagesSatpute 2018Mahmoud Abo AlfaNo ratings yet
- 10 1016@j Physio 2019 11 002Document27 pages10 1016@j Physio 2019 11 002Milton Ricardo de Medeiros FernandesNo ratings yet
- The Effect of Addition Kinesio Taping To Mckenzie Exercise in Patient With Chronic Mechanical Low Back PainDocument4 pagesThe Effect of Addition Kinesio Taping To Mckenzie Exercise in Patient With Chronic Mechanical Low Back PainRama BayuNo ratings yet
- Abstracts / Manual Therapy 25 (2016) E57 Ee169 E132Document2 pagesAbstracts / Manual Therapy 25 (2016) E57 Ee169 E132NICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- RCT LBP MsiDocument12 pagesRCT LBP Msimukesh pokharelNo ratings yet
- cln63 6p0763Document8 pagescln63 6p0763marcelonorisNo ratings yet
- Pilates RandomizadoDocument13 pagesPilates RandomizadorodrigueuresNo ratings yet
- Comparing The Pilates Method With No Exercise or Lumbar Stabilization For Pain and Functionality in Patients With Chronic Low Back Pain: Systematic Review and Meta-AnalysisDocument11 pagesComparing The Pilates Method With No Exercise or Lumbar Stabilization For Pain and Functionality in Patients With Chronic Low Back Pain: Systematic Review and Meta-AnalysisDinda BungaNo ratings yet
- Effects of Six-Week Exercise Training Protocol On Pain Relief in Patients With Lumbar Disc HerniationDocument7 pagesEffects of Six-Week Exercise Training Protocol On Pain Relief in Patients With Lumbar Disc HerniationAlexandra NistorNo ratings yet
- Clinical Pilates Versus General Exercise For Chronic Low Back Pain: Randomized TrialDocument9 pagesClinical Pilates Versus General Exercise For Chronic Low Back Pain: Randomized TrialvistablancaNo ratings yet
- Pillastrini 2016Document41 pagesPillastrini 2016alonsoNo ratings yet
- Negrini 2Document5 pagesNegrini 2iguija6769No ratings yet
- 189-198 FukatoVol8No3 PDFDocument10 pages189-198 FukatoVol8No3 PDFIndah YulantariNo ratings yet
- PhysicalTreatments v4n1p25 en PDFDocument9 pagesPhysicalTreatments v4n1p25 en PDFFadma PutriNo ratings yet
- A Structured Physiotherapy Treatment Model Can Provide Rapid Relief To Patients Who Qualify For Lumbar Disc Surgery: A Prospective Cohort StudyDocument8 pagesA Structured Physiotherapy Treatment Model Can Provide Rapid Relief To Patients Who Qualify For Lumbar Disc Surgery: A Prospective Cohort StudyQuiroprácticaParaTodosNo ratings yet
- Treating Lumbar SpondylosisDocument10 pagesTreating Lumbar SpondylosisDiyya Awaliah Nurhakiimah IbrahimNo ratings yet
- Maik SLR and Slump Stretching With LBP Neural TensionDocument9 pagesMaik SLR and Slump Stretching With LBP Neural TensionFallahPhysioNo ratings yet
- Demi Rel 2019Document7 pagesDemi Rel 2019Luis Miguel Cardona VelezNo ratings yet
- Effect of Lumbar Stabilization and Dynamic LumbarDocument9 pagesEffect of Lumbar Stabilization and Dynamic LumbarwladjaNo ratings yet
- Brazilian Journal of Physical TherapyDocument9 pagesBrazilian Journal of Physical TherapyWahdina PratamaNo ratings yet
- Clinical StudyDocument9 pagesClinical StudyJavierAntonioMéndezNo ratings yet
- Vikranth .G .R Lawrence Mathias Mohd Meraj Ghori: BackgroundDocument8 pagesVikranth .G .R Lawrence Mathias Mohd Meraj Ghori: BackgroundSekar AyuNo ratings yet
- Conservative Management of A Young Adult With Hip ArthrosisDocument9 pagesConservative Management of A Young Adult With Hip ArthrosisKanika SinhaNo ratings yet
- Neuromuscular Training in PFPS Protocol BMC 2014Document10 pagesNeuromuscular Training in PFPS Protocol BMC 2014Michele GonçalvesNo ratings yet
- Journal Pre-Proof: Clinical BiomechanicsDocument20 pagesJournal Pre-Proof: Clinical BiomechanicsAanggi JiihanNo ratings yet
- Lumbopelvic Stabilization Exercises and Mckenzie Method in Low Back Pain Due To Disc Protrusion: A Blind Randomized Clinical TrialDocument12 pagesLumbopelvic Stabilization Exercises and Mckenzie Method in Low Back Pain Due To Disc Protrusion: A Blind Randomized Clinical TrialZahra SativaniNo ratings yet
- 24 - JPTS 2012 156Document4 pages24 - JPTS 2012 156Βιβιλάκη ΓεωργίαNo ratings yet
- Stroke 2 RCTDocument6 pagesStroke 2 RCTArdhyan ArdhyanNo ratings yet
- The Effect of Spinal Exercises On H-Reflex in Subjects With Lumbosacral RadiculopathyDocument5 pagesThe Effect of Spinal Exercises On H-Reflex in Subjects With Lumbosacral RadiculopathyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 1809 2950 FP 21 04 00320Document7 pages1809 2950 FP 21 04 00320Susana SantanaNo ratings yet
- 2002 PDFDocument6 pages2002 PDFIMaa Wati AlbiizzahNo ratings yet
- Journal PPT - Imt 3Document39 pagesJournal PPT - Imt 3Iqbal KhanNo ratings yet
- Bernard 2020Document11 pagesBernard 2020JesusNavarrete97No ratings yet
- Effects of A 16-Week Pilates Exercises Training Program For Isometric Trunk Extension and Flexion StrengthDocument9 pagesEffects of A 16-Week Pilates Exercises Training Program For Isometric Trunk Extension and Flexion StrengthDiana Magnavita MouraNo ratings yet
- Short-And Long-Term Effects of Exercise On Neck Muscle Function in Cervical Radiculopathy: A Randomized Clinical TrialDocument9 pagesShort-And Long-Term Effects of Exercise On Neck Muscle Function in Cervical Radiculopathy: A Randomized Clinical Trialvidisanjaya21No ratings yet
- 1413 3555 Rbfis BJPT rbf20140158Document8 pages1413 3555 Rbfis BJPT rbf20140158Hector MiguelNo ratings yet
- Medicine: The Effect of Lumbar Stabilization and Walking Exercises On Chronic Low Back PainDocument10 pagesMedicine: The Effect of Lumbar Stabilization and Walking Exercises On Chronic Low Back Painmatiinu matiinuNo ratings yet
- Combination of Exercise and Advice Was Slightly Better Than Placebo For Subacute Low Back PainDocument1 pageCombination of Exercise and Advice Was Slightly Better Than Placebo For Subacute Low Back PainvinaymanNo ratings yet
- Dry Needling For Female Chronic Pelvic Pain A.3Document9 pagesDry Needling For Female Chronic Pelvic Pain A.3amnatul khairiNo ratings yet
- Cunha 2012Document4 pagesCunha 2012toaldoNo ratings yet
- Exercise and Nonspecific Low Back Pain A Literature ReviewDocument6 pagesExercise and Nonspecific Low Back Pain A Literature Reviewfvhj1y00No ratings yet
- Patients' Experience of Health Three Years After Structured Physiotherapy or Surgery For Lumbar Disc HerniationDocument8 pagesPatients' Experience of Health Three Years After Structured Physiotherapy or Surgery For Lumbar Disc HerniationsamNo ratings yet
- Case Report: Physical Therapy Management of Patients With Chronic Low Back Pain and Hip Abductor WeaknessDocument11 pagesCase Report: Physical Therapy Management of Patients With Chronic Low Back Pain and Hip Abductor WeaknessCleyber SantosNo ratings yet
- Kinesiofobia y Catastrofismo Del Dolor y PilatesDocument7 pagesKinesiofobia y Catastrofismo Del Dolor y Pilatescecilia martinezNo ratings yet
- 72-Article Text-135-1-10-20190522 PDFDocument7 pages72-Article Text-135-1-10-20190522 PDFestherNo ratings yet
- 72-Article Text-135-1-10-20190522 PDFDocument7 pages72-Article Text-135-1-10-20190522 PDFestherNo ratings yet
- Ocean Quest SSD Trainer Manual 2020Document109 pagesOcean Quest SSD Trainer Manual 2020Carmen LuckNo ratings yet
- UTC Building InfoDocument2 pagesUTC Building InfoWTVCNo ratings yet
- Gelofusine Solutionforinfusion MandatoryinformationDocument3 pagesGelofusine Solutionforinfusion Mandatoryinformationhanen.aymanNo ratings yet
- BA Euroflyer Direct Entry Pilot - Captain A320 at British AirwaysDocument1 pageBA Euroflyer Direct Entry Pilot - Captain A320 at British AirwaysdifjdjdjNo ratings yet
- Clinical Psychopharmacology Principles and Practice by S Nassir CompressedDocument600 pagesClinical Psychopharmacology Principles and Practice by S Nassir CompressedCátia Ramos100% (1)
- Neurotoxicity of Local Anesthetics in DentistryDocument7 pagesNeurotoxicity of Local Anesthetics in DentistryVinicíus PavaniNo ratings yet
- Fpsyg 12 601849Document16 pagesFpsyg 12 601849NOR BIBI MASLINA BINTI JUSOH MoeNo ratings yet
- Dwnload Full Managment Occupation Health and Safety 5th Edition Kevin Test Bank PDFDocument35 pagesDwnload Full Managment Occupation Health and Safety 5th Edition Kevin Test Bank PDFsinciputlateradiefk7u100% (7)
- Can Low-Fat Nutrition Labels Lead To Obesity PDFDocument15 pagesCan Low-Fat Nutrition Labels Lead To Obesity PDFSepti Lidya sariNo ratings yet
- Nur3116 Social Determinants of Health PaperDocument6 pagesNur3116 Social Determinants of Health Paperapi-578141969No ratings yet
- Pediatric Cardiology II Lecture SummaryDocument5 pagesPediatric Cardiology II Lecture SummaryMedisina101No ratings yet
- Subject: Submission of Deficient Information / Documents: F.No.10-10/2020-OTC) (M-82)Document107 pagesSubject: Submission of Deficient Information / Documents: F.No.10-10/2020-OTC) (M-82)Saad PathanNo ratings yet
- Beers Criteria Journal of Applied Pharmaceutical ScienceDocument8 pagesBeers Criteria Journal of Applied Pharmaceutical Sciencenurul.kusumawardani nurul.kusumawardaniNo ratings yet
- Debate US Initial Release Single Use PlasticsDocument226 pagesDebate US Initial Release Single Use Plasticsnamtran1066No ratings yet
- PRA Tool Box: 6.1. Brief Introduction To PRADocument16 pagesPRA Tool Box: 6.1. Brief Introduction To PRAfaisalNo ratings yet
- Natural Ways To Treat Hydrosalpinx (Blocked Fallopian Tube)Document11 pagesNatural Ways To Treat Hydrosalpinx (Blocked Fallopian Tube)drleetcmclinicNo ratings yet
- SF2 Daily Attendance ReportDocument3 pagesSF2 Daily Attendance ReportImelda Obdianela AmbeNo ratings yet
- DD - DA Li Ion MSDS U80277 2R2 - SDS 2018Document5 pagesDD - DA Li Ion MSDS U80277 2R2 - SDS 2018lintangscribdNo ratings yet
- Manufacturer:Shenzhen Zun Yi Pin Technology Co.,Ltd: User Manual -使用说明书Document9 pagesManufacturer:Shenzhen Zun Yi Pin Technology Co.,Ltd: User Manual -使用说明书Leandro Del GiudiceNo ratings yet
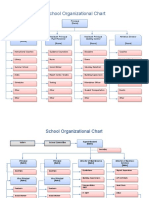
- School Organizational ChartDocument4 pagesSchool Organizational ChartislahNo ratings yet
- Accumulated Developmental Deficit Noel TylDocument7 pagesAccumulated Developmental Deficit Noel TylAycan ÖzenbaşNo ratings yet
- Research Proposal 4Document3 pagesResearch Proposal 4api-385647692No ratings yet
- Method Statement For PlasteringDocument14 pagesMethod Statement For Plasteringjameel100% (1)
- Graded RecitationDocument22 pagesGraded RecitationClara MaeNo ratings yet
- Openhrt 2021 001732Document9 pagesOpenhrt 2021 001732benypermadiNo ratings yet
- All India Institute of Medical SciencesDocument3 pagesAll India Institute of Medical SciencesNaresh BeatsNo ratings yet
- The Female Reproductive System: Dr. Emanuel Muro HkmuDocument41 pagesThe Female Reproductive System: Dr. Emanuel Muro HkmuMustafa DadahNo ratings yet
- Writing Sample 2Document9 pagesWriting Sample 2api-582848179No ratings yet
- [Journal of Autism and Childhood Schizophrenia vol. 49 iss. 6] Ng, Rowena_ Heinrich, Kimberley_ Hodges, Elise K. - Brief Report_ Neuropsychological Testing and Informant-Ratings of Children with Autism Spectrum Disorder, Atten - libgen.liDocument8 pages[Journal of Autism and Childhood Schizophrenia vol. 49 iss. 6] Ng, Rowena_ Heinrich, Kimberley_ Hodges, Elise K. - Brief Report_ Neuropsychological Testing and Informant-Ratings of Children with Autism Spectrum Disorder, Atten - libgen.ligustavNo ratings yet
- Microlife BP A3 Plus: EN ES FR IT DE TR PT NL GR ARDocument81 pagesMicrolife BP A3 Plus: EN ES FR IT DE TR PT NL GR ARYatzy Choi NekitoNo ratings yet























































































![[Journal of Autism and Childhood Schizophrenia vol. 49 iss. 6] Ng, Rowena_ Heinrich, Kimberley_ Hodges, Elise K. - Brief Report_ Neuropsychological Testing and Informant-Ratings of Children with Autism Spectrum Disorder, Atten - libgen.li](https://imgv2-1-f.scribdassets.com/img/document/596448205/149x198/c66e65b0ff/1710588633?v=1)
