You might also like
- Principle and Practice of Cardiac Mechanic For Assessing LV FunctionDocument33 pagesPrinciple and Practice of Cardiac Mechanic For Assessing LV FunctionSofia Kusumadewi100% (1)
- Arterial Stiffness-1Document21 pagesArterial Stiffness-1yoeldp100% (2)
- Wrist & HandDocument102 pagesWrist & Handeashoor100% (2)
- Aortic Stenosis: Teaching CourseDocument37 pagesAortic Stenosis: Teaching CourseDana BursacovschiNo ratings yet
- Aspects of Hearing Aids Fitting ProceduresDocument150 pagesAspects of Hearing Aids Fitting ProceduresakNo ratings yet
- Sl2. Maintain Safety and Security of The Ship's Crew and Passengers and The PDFDocument8 pagesSl2. Maintain Safety and Security of The Ship's Crew and Passengers and The PDFDaraNo ratings yet
- 12 Ida Jean OrlandoDocument10 pages12 Ida Jean OrlandoAntonio Calleja IINo ratings yet
- The Role of Imaging in Hypertensive Heart DiseaseDocument7 pagesThe Role of Imaging in Hypertensive Heart DiseasePradipta ShivaNo ratings yet
- Diagnosis: Imaging of Valvular Heart Disease in Heart FailureDocument9 pagesDiagnosis: Imaging of Valvular Heart Disease in Heart FailureAudini BerbasariNo ratings yet
- The Role of Echocardiographic Study in Patients With Chronic Kidney DiseaseDocument9 pagesThe Role of Echocardiographic Study in Patients With Chronic Kidney DiseaseshodhgangaNo ratings yet
- ECG and VCG in Left Ventricular Hypertrophy LVHDocument78 pagesECG and VCG in Left Ventricular Hypertrophy LVHNguyen TuanNo ratings yet
- 1 PBDocument13 pages1 PBme1921No ratings yet
- Otterstad 1996Document11 pagesOtterstad 199669262650irinaNo ratings yet
- Cramariuc 2016Document43 pagesCramariuc 201669262650irinaNo ratings yet
- Diastolic Heart Failure A Disorder of The Elderly Patient - 46PDocument46 pagesDiastolic Heart Failure A Disorder of The Elderly Patient - 46PproctaNo ratings yet
- Atherosclerosis and Stable Ihd-HorvathDocument60 pagesAtherosclerosis and Stable Ihd-HorvathTaarik DookieNo ratings yet
- Myocardial Work in Nonobstructive Hypertrophic Cardiomyopathy: Implications For OutcomeDocument8 pagesMyocardial Work in Nonobstructive Hypertrophic Cardiomyopathy: Implications For Outcomeme1921No ratings yet
- Underwriting LVH 1992Document6 pagesUnderwriting LVH 1992Nisa FjrNo ratings yet
- 01 HYP 0000236550 90214 1cDocument6 pages01 HYP 0000236550 90214 1cJefriantoNo ratings yet
- Nihms 5948Document31 pagesNihms 5948mimiNo ratings yet
- De Baat 2021Document7 pagesDe Baat 2021Dhan RamadhanNo ratings yet
- JR 1 - Mutia ChairaniDocument6 pagesJR 1 - Mutia ChairaniirsyadilfikriNo ratings yet
- Friesen 2013Document2 pagesFriesen 2013ritu10maliNo ratings yet
- Ehac 504Document13 pagesEhac 504Raudha Dani RahmalisaNo ratings yet
- Edited Cardiovascular Evaluation in Patients Undergo Non-Cardiac Surgery - Gadis Virza - Dr. Nur HaryonoDocument26 pagesEdited Cardiovascular Evaluation in Patients Undergo Non-Cardiac Surgery - Gadis Virza - Dr. Nur HaryonoFikriYTNo ratings yet
- O Brien Et Al 2020 Left Ventricular Mass and Wall Thickness Measurements Using Echocardiography and Cardiac Mri inDocument7 pagesO Brien Et Al 2020 Left Ventricular Mass and Wall Thickness Measurements Using Echocardiography and Cardiac Mri inS Ram KishoreNo ratings yet
- ICRJ-Validation of Cornell Product As A Method of Assessing Left Ventricular HypertrophyDocument5 pagesICRJ-Validation of Cornell Product As A Method of Assessing Left Ventricular Hypertrophysamir raflaNo ratings yet
- Leong2015 Hub Total Waktu Iskemik LVMD Dan AritmiaDocument8 pagesLeong2015 Hub Total Waktu Iskemik LVMD Dan AritmiaauliaNo ratings yet
- Eht 179Document10 pagesEht 179fauzibigbossNo ratings yet
- Cardiopatia HipertroficaDocument6 pagesCardiopatia HipertroficaPaulo Eduardo CampanaNo ratings yet
- Ehv 738Document10 pagesEhv 738Andreina AcevedoNo ratings yet
- Georgio Poul Ou 2010Document16 pagesGeorgio Poul Ou 2010ireneaureliaNo ratings yet
- Agustus Monitoring HemodinamikDocument61 pagesAgustus Monitoring HemodinamikFikriYTNo ratings yet
- Effect of Right Ventricular Function and Pulmonary Pressures On Heart Failure PrognosisDocument7 pagesEffect of Right Ventricular Function and Pulmonary Pressures On Heart Failure PrognosisMatthew MckenzieNo ratings yet
- Imaging of Myocardial Fibrosis and ItsDocument9 pagesImaging of Myocardial Fibrosis and ItsGaal PinNo ratings yet
- 17 PDFDocument11 pages17 PDFruryNo ratings yet
- Left Ventricular Remodeling in Heart FailureDocument11 pagesLeft Ventricular Remodeling in Heart FailureSabrinaAyuPutriNo ratings yet
- J Jacc 2013 08 1622Document6 pagesJ Jacc 2013 08 1622Triệu Khánh VinhNo ratings yet
- Jeac123 PDFDocument3 pagesJeac123 PDFRaquel AguilarNo ratings yet
- Magdy El-Masry Prof. of Cardiology Tanta UniversityDocument55 pagesMagdy El-Masry Prof. of Cardiology Tanta UniversityPrabJot SinGhNo ratings yet
- 9 Articulo3Document22 pages9 Articulo3paredesparrabrendalizbethNo ratings yet
- Case Report - Deep Vein Thrombosis in Patient With Acute Heart Failure Due To Chemotherapy Induced CardiomyopathyDocument15 pagesCase Report - Deep Vein Thrombosis in Patient With Acute Heart Failure Due To Chemotherapy Induced CardiomyopathyAbdurrohman IzzuddinNo ratings yet
- Constrictive Pericarditis: Role of Echocardiography and Magnetic Resonance ImagingDocument14 pagesConstrictive Pericarditis: Role of Echocardiography and Magnetic Resonance ImagingsunprizeproductionNo ratings yet
- J JCMG 2020 06 040Document10 pagesJ JCMG 2020 06 040Andrés MoreanoNo ratings yet
- Burrage-Ferreira2020 Article CardiovascularMagneticResonancDocument13 pagesBurrage-Ferreira2020 Article CardiovascularMagneticResonancsebas paezNo ratings yet
- 22 (Global Burden Diseases 2004)Document9 pages22 (Global Burden Diseases 2004)DianNo ratings yet
- Rheumatology 2006 Maksimovi Iv26 31Document6 pagesRheumatology 2006 Maksimovi Iv26 31Thio GifarnoNo ratings yet
- Echocardiography in End-Stage Renal Disease: Azin Alizadehasl and Anita SadeghpourDocument4 pagesEchocardiography in End-Stage Renal Disease: Azin Alizadehasl and Anita SadeghpourindahNo ratings yet
- High Total Leukocyte Count and Heart Failure After Myocardial InfarctionDocument10 pagesHigh Total Leukocyte Count and Heart Failure After Myocardial InfarctionRJMNo ratings yet
- Diab 1Document12 pagesDiab 1marsim92No ratings yet
- Ecr 16 E05Document8 pagesEcr 16 E05melon segerNo ratings yet
- Prognostic Role of Subclinical Left Ventricular Systolic Dysfunction Evaluated by Speckle-Tracking Echocardiography in Rheumatoid ArthritisDocument10 pagesPrognostic Role of Subclinical Left Ventricular Systolic Dysfunction Evaluated by Speckle-Tracking Echocardiography in Rheumatoid ArthritisEmanuel NavarreteNo ratings yet
- Right Ventricular Injury in ST-Elevation Myocardial InfarctionDocument9 pagesRight Ventricular Injury in ST-Elevation Myocardial InfarctionRismarini AsantiNo ratings yet
- Wellen's Syndrome: Mohan GameshDocument28 pagesWellen's Syndrome: Mohan Gameshmyolie wuNo ratings yet
- Chapter 61 Stable IHD PDFDocument45 pagesChapter 61 Stable IHD PDFJamil BaternaNo ratings yet
- Severe Hyperkalemia Can The Electrocardiogram Risk Stratify For Short-Term Adverse EventsDocument9 pagesSevere Hyperkalemia Can The Electrocardiogram Risk Stratify For Short-Term Adverse EventsCavalerul Mesei CromaticeNo ratings yet
- Classification of HT Goal of Therapy Lifestyle Modifications Pharmacological Therapy Management HT ConclusionDocument82 pagesClassification of HT Goal of Therapy Lifestyle Modifications Pharmacological Therapy Management HT ConclusionBima Ewando KabanNo ratings yet
- Echocardiographic Outcomes After Transcatheter Lea Et Approximation in Patients With Secondary Mitral RegurgitationDocument11 pagesEchocardiographic Outcomes After Transcatheter Lea Et Approximation in Patients With Secondary Mitral RegurgitationAbdul Gafur MarzukiNo ratings yet
- Patterns of Myocardial Late Enhancement: Typical and Atypical FeaturesDocument9 pagesPatterns of Myocardial Late Enhancement: Typical and Atypical FeaturesRicardo VallejoNo ratings yet
- 02 Identification of Shock in The ERDocument13 pages02 Identification of Shock in The ERMartin Miguel AmorNo ratings yet
- Mark H. Drazner: The Progression of Hypertensive Heart DiseaseDocument9 pagesMark H. Drazner: The Progression of Hypertensive Heart DiseaseAflifia Birruni SabilaNo ratings yet
- High Prevalence of Subclinical Left Ventricular Dysfunction in Patients With Psoriatic ArthritisDocument8 pagesHigh Prevalence of Subclinical Left Ventricular Dysfunction in Patients With Psoriatic ArthritisEmanuel NavarreteNo ratings yet
- Surgical Coronary Revascularization Who, What, WhenDocument68 pagesSurgical Coronary Revascularization Who, What, WhenAlaaGaballaNo ratings yet
- BU NestleDocument26 pagesBU Nestlescribd_mariumNo ratings yet
- Takashima 2016Document15 pagesTakashima 2016Fatih HarisNo ratings yet
- A Novel Approach For Iron DeficiencyDocument15 pagesA Novel Approach For Iron DeficiencyMahyar MehrNo ratings yet
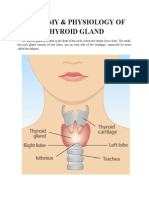
- Anatomy & Physiology of Thyroid GlandDocument5 pagesAnatomy & Physiology of Thyroid GlandJohnpaul DelapenaNo ratings yet
- Drug Study Hepa BDocument3 pagesDrug Study Hepa BKwebblekop JordiNo ratings yet
- Fix A Nator A Fixed Bionator Technique ArticleDocument6 pagesFix A Nator A Fixed Bionator Technique ArticleOrtho OrganizersNo ratings yet
- Savulescu - Is The Sale of Body Parts WrongDocument2 pagesSavulescu - Is The Sale of Body Parts WrongNoelle CaballeraNo ratings yet
- V2 N2 JITED P03 - Uma Devi T - Stress ManagementDocument19 pagesV2 N2 JITED P03 - Uma Devi T - Stress ManagementDev UdiataNo ratings yet
- Pioneers in Thyroid Surgery ARTICLEDocument12 pagesPioneers in Thyroid Surgery ARTICLESandu AlexandraNo ratings yet
- Pangestuti, Arifin - 2018 - Medicinal and Health Benefit Effects of Functional Sea CucumbersDocument11 pagesPangestuti, Arifin - 2018 - Medicinal and Health Benefit Effects of Functional Sea CucumbersGREESTYNo ratings yet
- 2017 RETA Conference RAGAGEPDocument33 pages2017 RETA Conference RAGAGEPArdago LenggaNo ratings yet
- Al Chami 2015Document4 pagesAl Chami 2015Zurya UdayanaNo ratings yet
- Enoxaparin Info SheetDocument7 pagesEnoxaparin Info SheetjafarkassimNo ratings yet
- 2011 Conference Book FinalDocument44 pages2011 Conference Book FinalIBWC1609No ratings yet
- Filariasis Lymphatic FilariasisDocument22 pagesFilariasis Lymphatic FilariasisNurfanida Natasya MNo ratings yet
- DEPED School FormsDocument30 pagesDEPED School FormsMayette ManigosNo ratings yet
- World Health DayDocument18 pagesWorld Health DayRamandeep KaurNo ratings yet
- WHO - Traditional Medicine - Growing Needs & PotentialDocument6 pagesWHO - Traditional Medicine - Growing Needs & PotentialDonny LoNo ratings yet
- KLKPD Kls XI Chapter 1, GanjilDocument12 pagesKLKPD Kls XI Chapter 1, GanjilFriski FriskiNo ratings yet
- Ramos V CA (MR)Document41 pagesRamos V CA (MR)nobocNo ratings yet
- Brightening Face Scrub - Sun BumDocument1 pageBrightening Face Scrub - Sun BumindiNo ratings yet
- 1 s2.0 S0753332217349909 MainDocument11 pages1 s2.0 S0753332217349909 MainBadiu ElenaNo ratings yet
- 1 Term Paper: BIMARU StatesDocument16 pages1 Term Paper: BIMARU StatesDivyansh NegiNo ratings yet
- Accelerated and Personalized Therapy For Heart Failure With Reduced Ejection FractionDocument15 pagesAccelerated and Personalized Therapy For Heart Failure With Reduced Ejection FractiondrguillermomoNo ratings yet
- Fotona Dynamis Brochure Fotona 2 WebDocument21 pagesFotona Dynamis Brochure Fotona 2 WebAferNo ratings yet
- PACES23 Scenario Videos - Consultation With SurrogateDocument5 pagesPACES23 Scenario Videos - Consultation With Surrogatesam SamehNo ratings yet