Professional Documents
Culture Documents
Med Social
Uploaded by
qandrew2201Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Med Social
Uploaded by
qandrew2201Copyright:
Available Formats
ORIGINAL ARTICLE
Ultra-Processed Foods Consumption Increases the Risk
of Hypertension in Adults: A Systematic Review and
Meta-Analysis
Mei Wang,1,2,3,4,* Xinyi Du,1,2,3,4,* Wei Huang,1,2,3,4 and Yong Xu1,2,3,4,
Downloaded from https://academic.oup.com/ajh/article/35/10/892/6617679 by guest on 03 November 2023
BACKGROUND ratio: 1.23; 95% CI: 1.11, 1.37; P = 0.034). Furthermore, analyses were
Effect of ultra-processed foods (UPFs) consumption on health has performed based on gender, study design, exposure assessment,
attracted widespread attention in recent years. However, the re- outcome assessment, body mass index, energy intake, and phys-
lationship between UPFs consumption and hypertension is un- ical activity, which suggested that the results remained statistically
clear. This meta-analysis was conducted to analyze the above significant.
association.
CONCLUSIONS
METHODS Our findings suggested that UPFs might have detrimental effects on
We systematically searched PubMed, Embase, and Cochrane Library the incidence of hypertension in the general population. Although
for all relevant studies published up to 31 January 2022 without lan- current evidence is limited, it cannot be denied that reducing con-
guage limitation. The random-effects model was selected to pool the sumption of UPFs may contribute to decrease the risk of chronic
effect sizes and 95% confidence intervals (CIs). noncommunicable diseases.
RESULTS Keywords: blood pressure; hypertension; systematic review and meta-
Nine observational studies involving 111,594 participants were in- analysis; ultra-processed foods.
cluded. Results from this meta-analysis showed that higher UPFs
consumption significantly increased the risk of hypertension (odds https://doi.org/10.1093/ajh/hpac069
With the rapid development in the technology related to as oils, butter, sugar, and salt; (iii) processed foods, such as bottled
food production and processing, the global food system has vegetables, canned fish, fruits in syrup, cheeses, and freshly made
undergone significant changes in the past decades.1,2 Ultra- breads; (iv) UPFs, such as sausages, savory packaged snacks,
processed foods (UPFs) rich in sugar and saturated fats domi- reconstituted meat products.4 At the highest end of the pro-
nate the food supplies of high-income countries, and that UPFs cessing spectrum, UPFs are characteristically energy dense, high
consumption is now rapidly increasing in middle-income in unhealthy types of fat, refined starches, free sugars and salt,
countries, which might attribute to its availability, afforda- and poor sources of protein, dietary fiber, and micronutrients,5,6
bility, and marketability.3 Additionally, UPFs are considered many of these nutritional features being directly related to ad-
to be the major source of energy in most countries.2 verse health. Moreover, ultra-processed products are made to
To study the effect of food processing on nutritional quality and be hyperpalatable and attractive, with long shelf-life, and able to
health, the NOVA classification system, most widely used system be consumed anywhere, anytime.7 Therefore, UPFs have almost
for studying food processing, classifies foods into 4 groups based replaced the minimally processed food and freshly prepared
on the extent and purpose of food processing: (i) unprocessed dishes, and are high popularity worldwide.8
or minimally processed foods, such as fruits, offal, eggs, milk, The evidence so far has demonstrated that UPFs are asso-
fungi, algae, and water; (ii) processed culinary ingredients, such ciated with unhealthy dietary nutrient profiles and several
1Department of Endocrinology and Metabolism, Affiliated Hospital of
*These authors have contributed equally to this work and share first
authorship. Southwest Medical University, Luzhou, Sichuan, China; 2Luzhou Key
Laboratory of Cardiovascular and Metabolic Diseases, Department of
Correspondence: Yong Xu (xywyll@swmu.edu.cn). Endocrinology and Metabolism, the Affiliated Hospital of Southwest
Medical University, Luzhou, Sichuan, China; 3Sichuan Clinical
Initially submitted April 22, 2022; accepted for publication June 18, Research Center for Nephropathy, Department of Endocrinology and
2022; online publication June 24, 2022. Metabolism, Luzhou, Sichuan, China; 4Metabolic Vascular Disease Key
Laboratory of Sichuan Province, Department of Endocrinology and
Metabolism, Luzhou, Sichuan, China.
© The Author(s) 2022. Published by Oxford University Press on
behalf of American Journal of Hypertension, Ltd. All rights reserved.
For permissions, please e-mail: journals.permissions@oup.com
892 American Journal of Hypertension 35(10) October 2022
Ultra-processed Foods and Hypertension
noncommunicable chronic diseases.8 Several observational Exclusion criteria
studies have found that UPFs significantly increase the risk
of cardiovascular diseases,9,10 all-cause mortality,11,12 over- The exclusion criteria were as follows: (i) duplicate
weight and obesity,13,14 cancers,15,16 and depression.17,18 reports; (ii) not population-based studies; (iii) case
In contrast, there is evidence that consumption of cer- reports, comments, reviews, and conference summary;
tain unprocessed or minimally processed foods, such as (iv) nonobservational design; (v) not examined the associ-
whole grains, fruits, and vegetables, is inversely associated ation between UPFs and the risk of hypertension; (vi) not
with weight gain.19–21 Recently, possible relationships be- provided the relevant effect sizes and corresponding 95%
tween UPFs and hypertension are being more widespread confidence; and (vii) unavailable full text or incomplete
concerns. Some studies assessed the association between data.
intake of UPFs and hypertension,22–30 but the findings are
inconsistent. Therefore, a full understanding of the effect of Selection and data extraction
UPFs consumption on hypertension is greatly necessary.
Downloaded from https://academic.oup.com/ajh/article/35/10/892/6617679 by guest on 03 November 2023
Although 2 recent systematic reviews assessed the asso- The titles and abstracts were screened independently
ciation between UPFs consumption and hypertension,31,32 by 2 authors (MW and XYD). Then the full texts were
some limitations would not be ignored. The results of reviewed based on inclusion and exclusion criteria. Any
previous studies showed that there was no statistically disagreement was resolved by the third party through ne-
significant association between UPFs consumption and hy- gotiation. Studies would be included in this meta-analysis if
pertension,31 or it only reviewed the studies on UPFs con- they examined the relationship between UPFs and the risk
sumption and hypertension without quantitative analysis.32 of hypertension in populations, and provided outcomes of
As a result, the association between UPFs consumption and hypertension and their risk estimates and 95% CIs. The fol-
hypertension remains unclear. Therefore, we aimed to con- lowing data from eligible published articles were extracted:
duct a comprehensive meta-analysis and systematic review (i) first author’s last name; (ii) year of publication; (iii)
of observational studies to assess the relationship between type of study design; (iv) study location; (v) number of
UPFs consumption and hypertension in adults. participants; (vi) age range and gender; (vii) duration of
follow-up for cohort studies; (viii) primary outcomes; (ix)
the most adjusted risk estimates (risk ratio, hazard ratio,
METHODS and OR) and corresponding 95% CIs; and (x) the covariates
This meta-analysis was conducted based on the Preferred used for adjustment.
Reporting Items for Systematic Reviews and Meta-Analyses
(PRISMA) guideline33 (Supplementary Table S1 online). Assessment of study quality
Ethical approval was not necessary because this study was
meta-analysis of published studies. Two investigators (MW and XYD) separately assessed
the quality of included articles using the Newcastle-Ottawa
scale (NOS) which was adapted for cross-sectional and co-
Search strategy and study selection hort studies. The NOS includes selection, comparability, and
We conducted a comprehensive literature search for outcome. Studies with NOS scores 1–3 stars indicated poor
all potentially relevant observational studies in PubMed, quality, NOS scores 4–6 stars indicated fair quality, and NOS
Embase, and Cochrane Library up to 31 January 2022 with scores 7–9 stars indicated high quality.34
no restriction on language. The search-relevant keywords
are as follows: ([Ultra processed foods OR Ultraprocessed Statistical analysis
foods OR Ultra-processed foods OR Processed foods] AND
[Hypertension OR Blood pressure]). We also examined rel- We equated hazard ratio and risk ratio with OR in this
evant original studies and review articles to search for other meta-analysis.35 The potential sources of heterogeneity
eligible studies. The search strategy is given in detail in between studies were assessed by using the Q test and I2
Supplementary Table S2 online. statistics,36 and I2 > 50% or P < 0.05 indicated significant het-
erogeneity. The random-effect model would be selected to
Inclusion criteria pool the effect sizes and corresponding 95% CIs if there was
significant heterogeneity. Otherwise, the fixed-effect model
Studies were included if they met the following explicit was employed. In order to further investigate whether the
criteria: (i) the type of research was observational studies relationship between UPFs and incidence of diabetes mel-
(such as cohort, cross-sectional, and case–control studies); litus and hypertension was biased by some specific factors
(ii) they were population-based studies; (iii) participants (e.g., study design, type of diseases, gender, continent, expo-
were ≥18 years old at baseline; (iv) the exposure interested sure assessment, outcome assessment, sample size, follow-up
was UPFs (as defined by the NOVA classification system); time, and adjustments [such as body mass index, energy in-
(v) the primary outcome of interest was hypertension; and take, and physical activity]), we conducted the subgroup
(vi) data provided as risk ratio, hazard ratio, or odds ratio analyses based on above factors. All statistical analyses were
(OR) and corresponding 95% confidence intervals (CIs) for conducted with Stata software (version 12.0, Stata Corp LP,
the risk of hypertension. College Station, TX).
American Journal of Hypertension 35(10) October 2022 893
Wang et al.
RESULTS Sensitivity analysis
Literature search and study characteristics Sensitivity analysis indicated that none of the included
studies had significant impact on the results of the meta-
We initially identified 1004 relevant articles from analysis (Figure 3).
PubMed, Embase, and Cochrane Library database. Finally,
9 articles met the inclusion criteria were included in this
meta-analysis after excluding duplicates, unrelated arti- Publication bias
cles, reviews, meta-analyses, and other studies. The pro- The Begg’s rank correlation test and the Egger’s regression
cess of literature screening is provided in the flow chart test confirmed that there was no publication bias for hyper-
(Figure 1). All of the included studies were observational, tension (P = 0.348 and P = 0.247, respectively). As shown in
including 4 cohort studies25,26,29,30 and 5 cross-sectional Figure 4, the funnel plots were symmetrical, which revealed
studies.22–24,27,28 Two studies were conducted in the United no clear publication bias.
States,22,24 2 in Canada,23,27 2 in Brazil,29,30 1 in Spain,25 1
Downloaded from https://academic.oup.com/ajh/article/35/10/892/6617679 by guest on 03 November 2023
in Mexico,26 and 1 in Lebanon.28 Eight studies included
both men and women, 1 study only included women. DISCUSSION
For exposure assessment, 6 studies used food-frequency
questionnaire as exposure assessment tools,22,25,26,28–30 In our meta-analysis, we systematically summarized
while 3 studies were based on 24-hour dietary recall or the current published observational studies examining the
records.23,24,27 The characteristics of all included studies association between UPFs consumption and the risk of
are shown in Table 1. hypertension.
The result suggested that higher consumption of UPFs
significantly increased the risk of hypertension in adults.
UPFs consumption and the risk of hypertension Subgroup analyses, conducted based on study design, sample
size, geographical location, body mass index, energy intake,
Nine studies, including 4 cohort studies and 5 cross-sec- and physical activity, indicated that the results remained re-
tional studies, explored the effect of UPFs consumption on markable correlation between UPFs consumption and risk
the incidence of hypertension. Results of the meta-analysis of hypertension.
of 9 studies indicated that higher consumption of UPFs As the subgroup analysis showed, there was no association
was significantly associated with incidence of hypertension between UPFs consumption and hypertension in females,
(pooled OR: 1.23; 95% CI: 1.11, 1.37; I2 = 51.9%, P = 0.034), although based on only 1 study.26 The potential explana-
and the statistical heterogeneity was moderate with an I2 of tion may be that the ratio of energy contribution of UPFs
51.9% (Figure 2). Furthermore, analyses were performed in different countries may variable. For instance, the ratio
based on gender, study design, exposure assessment, out- of energy contribution of UPFs is 62% in the United States
come assessment, body mass index, energy intake, and but 29% in Chile, which perhaps causes the difference of in-
physical activity, which suggested that the results remained cidence of hypertension related to UPFs consumption.7,37
statistically significant (Table 2). Besides, the effect of UPFs on health may be cumulative
outcome over a long period of time but not captured in
short term. Moreover, education and income may also be
important factors to influence the result because the study
was conducted based on Mexican Teachers’ Cohort. Future
studies are needed to explore the effect of UPF consumption
on hypertension of different genders.
Our findings of a positive association between higher in-
take of UPFs and hypertension are consistent with previous
studies. A recent meta-analysis of observational studies
showed that sugar-sweetened beverages, which are part of
the definition of UPFs, are considered to be significantly as-
sociated with hypertension, as well as obesity, T2DM, and
all-cause mortality.38 It is reported that participants with
higher intake of UPFs had a greater risk of overweight and
obesity compared with participants with lower intake of
UPFs.39 And it is well known that obesity is considered as an
important risk factor for hypertension.
Recently, several potential mechanisms have been suggested
to explain the association between UPFs intake and the risk of
hypertension. As we mentioned earlier, UPFs are nutritionally
unbalanced due to high levels of free/added sugars, saturated
Figure 1. Flow diagram for the selection of eligible observational and trans-fatty acids, and low levels of protein, dietary fiber,
articles. and micronutrients. These differences in nutrient content of
894 American Journal of Hypertension 35(10) October 2022
Table 1. Characteristics of included studies in this meta-analysis
Study Sample Exposure Diagnostic criteria for Study
Study ID Country design size Age Sex Comparison Exposure Reference assessment hypertension quality Adjustment
Nardocci Canada Cross- 13,608 ≥19 M + F Q3 vs. Q1 ≥58.7% of ≤38.5% of 24-Hour Self-declared AH— 7 stars Age, sex, smoking
et al.27 sectional TE TE dietary answer to question status, physical
recall on long-term activity, education,
health conditions income, residential
diagnosed by area, immigrant status,
healthcare provider: alcohol consumption,
“Do you have residential area, and
diabetes/ indigenous identity.
high blood
pressure?”
Rezende- Brazil Cohort 1,221 35.2 M + F Q5 vs. Q1 34.6%– 0.8%– FFQ Self-declared medical 8 stars Gender, age, marital
Alves 76.2% 16.6% of diagnosis or use of status, skin color, per
et al.29 of TE TE antihypertensive or capita income, physical
self-declared high activity, smoking,
BP (≥130/80 mm obesity, family history
Hg) according to of hypertension, and
recent cutoff points energy intake.
proposed by ACC/
AHA.
Mendonça Spain Cohort 14,790 36.3 M + F Q3 vs. Q1 NR NR FFQ Self-declared medical 8 stars Sex, age, physical
et al.25 diagnosis. activity, hours of TV
watching, baseline
BMI, smoking status,
use of analgesics,
following a special
diet at baseline, family
history of hypertension,
hypercholesterolemia,
alcohol consumption,
total energy intake,
olive oil intake,
consumption of fruits,
and vegetables.
Ivancovsky- United Cross- 789 58.83 ± 6.58 M + F Q4 vs. Q1 NR NR FFQ Systolic BP/diastolic 8 stars Age, gender, BMI, saturate
Wajcman States sectional BP ≥130/80 mm Hg fatty acids and protein
et al. 22 and/or medication. intake, physical activity,
coffee, and fibers.
Scaranni Brazil Cohort 8,754 35–74 M + F Q3 vs. Q1 15% of TE 35% of TE FFQ Measurement of BP 8 stars Age, sex, color or race,
et al.30 (SBP ≥140 mm Hg education, physical
or DBP ≥90 mm activity, smoking, alcohol
Hg) and use of consumption, Na intake
antihypertensive in measured by 12-hour
previous 2 weeks. urine sample, total daily
energy intake.
Lavigne- Canada Cross- 811 ≥18 M + F Q5 vs. Q1 83% of TE 21.1% of 24-Hour Measurement of BP 7 stars Age, sex, area of
Robichaud sectional TE dietary (SBP ≥130 mm Hg residence, current
et al. 23 recall or DBP ≥85 mm smoker, alcohol drinker,
Hg). and total dietary energy
intake.
American Journal of Hypertension 35(10) October 2022
895
Ultra-processed Foods and Hypertension
Downloaded from https://academic.oup.com/ajh/article/35/10/892/6617679 by guest on 03 November 2023
896
Wang et al.
Table 1. Continued
Study Sample Exposure Diagnostic criteria for Study
Study ID Country design size Age Sex Comparison Exposure Reference assessment hypertension quality Adjustment
Nasreddine Lebanon Cross- 302 ≥18 M + F Q4 vs. Q1 NR NR FFQ Measurement of BP 8 stars Age, gender, marital
et al.28 sectional (SBP ≥130 mm Hg status, BMI, area of
or DBP ≥85 mm residence, level of
Hg). education, income,
smoking status,
physical activity,
and total energy
intake.
American Journal of Hypertension 35(10) October 2022
Martínez United Cross- 6,385 ≥20 M + F Q5 vs. Q1 >71% of <40% of 24-Hour Measurement of BP 7 stars Sex, age, race/ethnicity,
Steele States sectional TE TE dietary (SBP ≥130 mm ratio of family income to
et al.24 recall Hg and/or DBP poverty and educational
≥85 mm Hg) or attainment + current
currently taking smoking status, and
antihypertensive physical activity.
medication.
Monge Mexico Cohort 64,934 ≥25 F Q5 vs. Q1 ≤20% of >45% of FFQ Self-declared medical 7 stars Age, indigenous,
et al.26 TE TE diagnosis or use of internet access,
antihypertensive. insurance, family
history of hypertension,
menopausal status,
smoking, physical
activity, energy intake,
and multivitamin
intake.
Abbreviations: AH, arterial hypertension; BMI, body mass index; BP, blood pressure; DBP, diastolic blood pressure; F, females; FFQ, food-frequency questionnaire; M, males; NR, not
reported; SBP, systolic blood pressure; TE, total energy.
Downloaded from https://academic.oup.com/ajh/article/35/10/892/6617679 by guest on 03 November 2023
Ultra-processed Foods and Hypertension
Downloaded from https://academic.oup.com/ajh/article/35/10/892/6617679 by guest on 03 November 2023
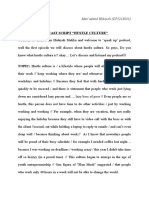
Figure 2. Forest plot of the association between consumption of ultra-processed foods (UPFs) and hypertension using a random-effects model. Meta-
analysis of the data from the 9 included studies demonstrated that higher consumption of UPFs significantly increased the risk of hypertension.
UPFs may play an important role in these mechanisms. Firstly, vitamins, and minerals,53 which may also contribute to the de-
highly processed foods tend to have higher levels of refined velopment of diabetes mellitus and hypertension.
carbohydrates, which are quickly absorbed into the blood- Another potential mechanism may be associated with
stream, leading to high glycemic load (GL),40 the latter may the wide range of additives added to UPFs and chem-
activate return-related neural circuits (such as the striatum) ical compounds formed during their manufacturing
similar to addictive substances and increase cravings and processes or released from their packaging materials. For
hunger, thereby leading to an increase in energy intake,41–43 example, emulsifiers (e.g., carboxymethylcellulose and
which is associated with higher hypertension prevalence, in- polysorbate-80), detergent-like molecules that are a ubiq-
cidence, and greater increases in blood pressure. Besides, uitous component of processed foods, may affect the
diets high in carbohydrate might elevate insulin secretion and gut microbiome and promote colitis and metabolic syn-
promote the partitioning of energy toward storage as fat; in drome.54 Long-term consumption of artificial sweeteners
response, hunger and appetite increases.44 And excessive in- might accelerate atherosclerosis and senescence via impair-
take of fat also contributes to weight gain and the risk of over- ment of function and structure of apolipoprotein A–I and
weight or obesity, the latter being recognized as an important high-density lipoprotein.55 High levels of polycyclic aro-
risk factor for cardiovascular diseases. Several studies have matic hydrocarbons have also been shown to be positively
shown that UPFs and beverages (e.g., confectionery snacks, associated with hypertension.56,57 Acrylamide and acrolein
sugar-sweetened beverages, and cakes) might contain rela- produced during food heat treatments were linked to an
tively high levels of glucose-derived advanced glycation end increased risk of cardiovascular diseases.58,59 However, it still
products, the latter enhancing oxidative stress and initiating remains unclear what plays a leading role in the association.
inflammatory responses, which over time could lead to or ac- It is urgent to need a better understanding of what really
celerate vascular diseases.9,45–47 Moreover, data from animal matters and how various aspects influence those impacts.
experimental studies suggested that fructose may increase Our study provided comprehensive evidence of the nega-
blood pressure by stimulating uric acid,48 inhibiting endothe- tive influence of UPFs intake on hypertension. The findings
lial nitric oxide synthase system,49,50 stimulating sympathetic indicate that more efforts should be put into reducing the
nervous system,51 or directly increasing sodium absorption in high consumption of UPFs, and attach importance to
the intestinal tract.52 Additionally, sodium is one of the main promoting healthy and sustainable dietary habits.
ingredients added in the process of producing ready-to-eat
food such as processed meat,4,29,53 and it is well established that Strengths and limitations
avoiding excessive sodium consumption is crucial to prevent
hypertension and to reduce cardiovascular risk. Furthermore, Our meta-analysis provides the most comprehensive as-
intake of UPFs is associated with low intake of protein, fiber, sessment on the associations of UPFs consumption with
American Journal of Hypertension 35(10) October 2022 897
Wang et al.
Table 2. Subgroup analyses of consumption of ultra-processed
foods (UPFs) and risk of hypertension
No. of
Subgroups studies OR (95% CI) I2 % P
All 9 1.23 (1.11–1.37) 51.9 0.034
Design
Cohort 4 1.16 (1.03–1.32) 55.20 0.082
Cross-sectional 5 1.35 (1.11–1.64) 44.30 0.127
Sex
M+F 8 1.27 (1.17–1.38) 14.50 0.317
Downloaded from https://academic.oup.com/ajh/article/35/10/892/6617679 by guest on 03 November 2023
M — — — —
F 1 0.98 (0.84–1.14) — —
Sample size Figure 3. Sensitivity analysis of all included studies.
≥10,000 3 1.22 (0.96–1.54) 83.4 0.002
<10,000 6 1.24 (1.13–1.36) 0.00 0.576
Exposure assessment
FFQ 6 1.20 (1.06–1.37) 51.00 0.069
Food record 3 1.29 (1.01–1.65) 61.8 0.073
Continent
Europe 1 1.21 (1.06–1.38) — —
Asia 1 3.10 (0.58–16.61) — —
North America 5 1.23 (1.01–1.50) 72.20 0.006
South America 2 1.26 (1.10–1.44) 0.00 0.580
Outcome assessment
Measured 5 1.23 (1.11–1.35) 0.00 0.486
Self-reported 4 1.24 (1.02–1.51) 76.80 0.005
BMI
Yes 2 1.58 (1.11–2.24) 0.00 0.420 Figure 4. Funnel plot evaluating the publication bias for associa-
tion between the intake of ultra-processed foods (UPFs) and the risk of
No 7 1.21 (1.08–1.35) 55.80 0.035 hypertension.
Energy intake
Yes 6 1.16 (1.03–1.30) 40.20 0.137 UPFs consumption was not exactly the same in the included
No 3 1.39 (1.12–1.72) 60.60 0.079 studies of this meta-analysis, which made these comparisons
less straightforward; thus, we could only obtain a quantita-
Physical activity
tive rate of the association between the UPFs consumption
Yes 8 1.24 (1.11–1.39) 56.50 0.024 and hypertension but not a specific range. Finally, subgroup
No 1 0.99 (0.59–1.67) — — meta-analyses by common study characteristic do not com-
pletely eliminate substantial heterogeneity across studies.
Abbreviations: BMI, body mass index; CI, confidence interval; F, Improved analyses should be carried out as more informa-
females; FFQ, food-frequency questionnaire; M, males; OR, odds tion becomes available in the future.
ratio. Based on our findings, consumption of UPFs is signifi-
cantly associated with an increased risk of hypertension in
hypertension. Moreover, studies involving a large number adults. As the current evidence is limited, more longitudinal
of participants are expected to provide sufficient statis- studies and intervention studies are needed in the future to
tical power to examine the relationship between UPF and further explore the potential association between UPFs con-
hypertension. Nevertheless, there are also several limita- sumption and hypertension.
tions to be acknowledged. Firstly, our meta-analysis was
based on observational studies and thus some unmeasured
confounding factors may have various degrees of influence SUPPLEMENTARY MATERIAL
on the results. Secondly, the studies included in this meta-
analysis were used to assess UPFs consumption through Supplementary data are available at American Journal of
food-frequency questionnaire, food recording, and 24-hour Hypertension online.
recall, which are likely to recall bias. Thirdly, the definition of Supplementary Table 1. PRISMA checklist.
898 American Journal of Hypertension 35(10) October 2022
Ultra-processed Foods and Hypertension
Supplementary Table 2. Search strategy to identify ob- 8. Forouzanfar MH, Afshin A, Alexander LT, Anderson HR, Bhutta ZA,
servational studies reporting the association between ultra- Biryukov S, Brauer M, Burnett R, Cercy K, Charlson FJ, Cohen AJ,
Dandona L, Estep K, Ferrari AJ, Frostad JJ, Fullman N, Gething PW,
processed foods (UPFs) consumption and hypertension. Godwin WW, Griswold M, Hay SI, Kinfu Y, Kyu HH, Larson HJ,
Liang X, Lim SS, Liu PY, Lopez AD, Lozano R, Marczak L, Mensah GA,
Mokdad AH, Moradi-Lakeh M, Naghavi M, Neal B, Reitsma MB,
Roth GA, Salomon JA, Sur PJ, Vos T, Wagner JA, Wang H, Zhao Y,
FUNDING
Zhou M, Aasvang GM, Abajobir AA, Abate KH, Abbafati C, Abbas KM,
Abd-Allah F, Abdulle AM, Abera SF, Abraham B, Abu-Raddad LJ,
This study was supported by the Sichuan Science and Abyu GY, Adebiyi AO, Adedeji IA, Ademi Z, Adou AK, Adsuar JC,
Technology Program, Sichuan, China (grant numbers: Agardh EE, Agarwal A, Agrawal A, Kiadaliri AA, Ajala ON,
2020YFS0456 and 2019YFS0537) and the Luzhou-Southwest Akinyemiju TF, Al-Aly Z, Alam K, Alam NKM, Aldhahri SF,
Medical University cooperation project, Luzhou, Sichuan, Aldridge RW, Alemu ZA, Ali R, Alkerwi Aa, Alla F, Allebeck P,
Alsharif U, Altirkawi KA, Martin EA, Alvis-Guzman N, Amare AT,
China (grant number: 2018LZXNYD—PT01). Amberbir A, Amegah AK, Amini H, Ammar W, Amrock SM,
Andersen HH, Anderson BO, Antonio CAT, Anwari P, Ärnlöv J,
Downloaded from https://academic.oup.com/ajh/article/35/10/892/6617679 by guest on 03 November 2023
Artaman A, Asayesh H, Asghar RJ, Assadi R, Atique S, Avokpaho EFGA,
Awasthi A, Quintanilla BPA, Azzopardi P, Bacha U, Badawi A,
Bahit MC, Balakrishnan K, Barac A, Barber RM, Barker-Collo SL,
ACKNOWLEDGMENTS Bärnighausen T, Barquera S, Barregard L, Barrero LH, Basu S, Batis C,
Bazargan-Hejazi S, Beardsley J, Bedi N, Beghi E, Bell B, Bell ML,
We thank all participants from the Department of Bello AK, Bennett DA, Bensenor IM, Berhane A, Bernabé E, Betsu BD,
Endocrinology and Metabolism, the Affiliated Hospital Beyene AS, Bhala N, Bhansali A, Bhatt S, Biadgilign S, Bikbov B,
of Southwest Medical University for their assistance and Bisanzio D, Bjertness E, Blore JD, Borschmann R, Boufous S,
Bourne RRA, Brainin M, Brazinova A, Breitborde NJK, Brenner H,
support. Broday DM, Brugha TS, Brunekreef B, Butt ZA, Cahill LE, Calabria B,
Campos-Nonato IR, Cárdenas R, Carpenter DO, Carrero JJ, Casey DC,
Castañeda-Orjuela CA, Rivas JC, Castro RE, Catalá-López F, Chang J-
AUTHORS’ CONTRIBUTIONS C, Chiang PP-C, Chibalabala M, Chimed-Ochir O, Chisumpa VH,
Chitheer AA, Choi J-YJ, Christensen H, Christopher DJ, Ciobanu LG,
Coates MM, Colquhoun SM, Manzano AGC, Cooper LT,
Y.X. and W.H. were involved in the whole conception and Cooperrider K, Cornaby L, Cortinovis M, Crump JA, Cuevas-Nasu L,
design process of the study. M.W. and X.D. contributed to Damasceno A, Dandona R, Darby SC, Dargan PI, das Neves J, Davis AC,
the selection of literature and participated in the process Davletov K, de Castro EF, De la Cruz-Góngora V, De Leo D,
of literature quality evaluation, data extraction, and anal- Degenhardt L, Del Gobbo LC, del Pozo-Cruz B, Dellavalle RP,
ysis. M.W. wrote the paper. Y.X. and W.H. commented on Deribew A, Jarlais DCD, Dharmaratne SD, Dhillon PK, Diaz-Torné C,
Dicker D, Ding EL, Dorsey ER, Doyle KE, Driscoll TR, Duan L,
the manuscript. All authors read and approved the final Dubey M, Duncan BB, Elyazar I, Endries AY, Ermakov SP, Erskine HE,
manuscript. Eshrati B, Esteghamati A, Fahimi S, Faraon EJA, Farid TA, Farinha CSeS,
Faro A, Farvid MS, Farzadfar F, Feigin VL, Fereshtehnejad S-M,
Fernandes JG, Fischer F, Fitchett JRA, Fleming T, Foigt N, Foreman K,
Fowkes FGR, Franklin RC, Fürst T, Futran ND, Gakidou E, Garcia-
DISCLOSURE Basteiro AL, Gebrehiwot TT, Gebremedhin AT, Geleijnse JM,
Gessner BD, Giref AZ, Giroud M, Gishu MD, Giussani G, Goenka S,
The authors declared no conflict of interest. Gomez-Cabrera MC, Gomez-Dantes H, Gona P, Goodridge A,
Gopalani SV, Gotay CC, Goto A, Gouda HN, Gugnani HC, Guillemin F,
Guo Y, Gupta R, Gupta R, Gutiérrez RA, Haagsma JA, Hafezi-Nejad N,
Haile D, Hailu GB, Halasa YA, Hamadeh RR, Hamidi S, Handal AJ,
Hankey GJ, Hao Y, Harb HL, Harikrishnan S, Haro JM, Hassanvand MS,
REFERENCES Hassen TA, Havmoeller R, Heredia-Pi IB, Hernández-Llanes NF,
Heydarpour P, Hoek HW, Hoffman HJ, Horino M, Horita N,
1. Swinburn BA, Sacks G, Hall KD, McPherson K, Finegood DT, Hosgood HD, Hoy DG, Hsairi M, Htet AS, Hu G, Huang JJ, Husseini A,
Moodie ML, Gortmaker SL. The global obesity pandemic: shaped by Hutchings SJ, Huybrechts I, Iburg KM, Idrisov BT, Ileanu BV, Inoue M,
global drivers and local environments. Lancet 2011; 378:804–814. Jacobs TA, Jacobsen KH, Jahanmehr N, Jakovljevic MB, Jansen HAFM,
2. Zobel EH, Hansen TW, Rossing P, von Scholten BJ. Global changes in Jassal SK, Javanbakht M, Jayaraman SP, Jayatilleke AU, Jee SH, Jeemon P,
food supply and the obesity epidemic. Curr Obes Rep 2016; 5:449–455. Jha V, Jiang Y, Jibat T, Jin Y, Johnson CO, Jonas JB, Kabir Z, Kalkonde Y,
3. Monteiro CA, Moubarac JC, Cannon G, Ng SW, Popkin B. Ultra- Kamal R, Kan H, Karch A, Karema CK, Karimkhani C, Kasaeian A,
processed products are becoming dominant in the global food system. Kaul A, Kawakami N, Kazi DS, Keiyoro PN, Kemmer L, Kemp AH,
Obes Rev 2013; 14(Suppl 2):21–28. Kengne AP, Keren A, Kesavachandran CN, Khader YS, Khan AR,
4. Monteiro CA, Cannon G, Moubarac JC, Levy RB, Louzada MLC, Khan EA, Khan G, Khang Y-H, Khatibzadeh S, Khera S, Khoja TAM,
Jaime PC. The UN Decade of Nutrition, the NOVA food classifica- Khubchandani J, Kieling C, Kim C-i, Kim D, Kimokoti RW, Kissoon N,
tion and the trouble with ultra-processing. Public Health Nutr 2018; Kivipelto M, Knibbs LD, Kokubo Y, Kopec JA, Koul PA, Koyanagi A,
21:5–17. Kravchenko M, Kromhout H, Krueger H, Ku T, Defo BK,
5. Moubarac JC, Batal M, Louzada ML, Martinez Steele E, Monteiro CA. Kuchenbecker RS, Bicer BK, Kuipers EJ, Kumar GA, Kwan GF, Lal DK,
Consumption of ultra-processed foods predicts diet quality in Canada. Lalloo R, Lallukka T, Lan Q, Larsson A, Latif AA, Lawrynowicz AEB,
Appetite 2017; 108:512–520. Leasher JL, Leigh J, Leung J, Levi M, Li X, Li Y, Liang J, Liu S, Lloyd BK,
6. Martínez Steele E, Baraldi LG, Louzada ML, Moubarac JC, Logroscino G, Lotufo PA, Lunevicius R, MacIntyre M, Mahdavi M,
Mozaffarian D, Monteiro CA. Ultra-processed foods and added sugars Majdan M, Majeed A, Malekzadeh R, Malta DC, Manamo WAA,
in the US diet: evidence from a nationally representative cross-sectional Mapoma CC, Marcenes W, Martin RV, Martinez-Raga J, Masiye F,
study. BMJ Open 2016; 6:e009892. Matsushita K, Matzopoulos R, Mayosi BM, McGrath JJ, McKee M,
7. Poti JM, Braga B, Qin B. Ultra-processed food intake and obesity: what Meaney PA, Medina C, Mehari A, Mejia-Rodriguez F, Mekonnen AB,
really matters for health-processing or nutrient content? Curr Obes Rep Melaku YA, Memish ZA, Mendoza W, Mensink GBM, Meretoja A,
2017; 6:420–431. Meretoja TJ, Mesfin YM, Mhimbira FA, Millear A, Miller TR, Mills EJ,
American Journal of Hypertension 35(10) October 2022 899
Wang et al.
Mirarefin M, Misganaw A, Mock CN, Mohammadi A, Mohammed S, 14. Nardocci M, Leclerc BS, Louzada ML, Monteiro CA, Batal M,
Mola GLD, Monasta L, Hernandez JCM, Montico M, Morawska L, Moubarac JC. Consumption of ultra-processed foods and obesity in
Mori R, Mozaffarian D, Mueller UO, Mullany E, Mumford JE, Canada. Can J Public Health 2019; 110:4–14.
Murthy GVS, Nachega JB, Naheed A, Nangia V, Nassiri N, Newton JN, 15. Fiolet T, Srour B, Sellem L, Kesse-Guyot E, Allès B, Méjean C,
Ng M, Nguyen QL, Nisar MI, Pete PMN, Norheim OF, Norman RE, Deschasaux M, Fassier P, Latino-Martel P, Beslay M, Hercberg S,
Norrving B, Nyakarahuka L, Obermeyer CM, Ogbo FA, Oh I-H, Lavalette C, Monteiro CA, Julia C, Touvier M. Consumption of ultra-
Oladimeji O, Olivares PR, Olsen H, Olusanya BO, Olusanya JO, processed foods and cancer risk: results from NutriNet-Santé prospec-
Opio JN, Oren E, Orozco R, Ortiz A, Ota E, Pa M, Pana A, Park E-K, tive cohort. BMJ 2018; 360:k322.
Parry CD, Parsaeian M, Patel T, Caicedo AJP, Patil ST, Patten SB, 16. Romaguera D, Fernández-Barrés S, Gracia-Lavedán E, Vendrell E,
Patton GC, Pearce N, Pereira DM, Perico N, Pesudovs K, Petzold M, Azpiri M, Ruiz-Moreno E, Martín V, Gómez-Acebo I, Obón M,
Phillips MR, Piel FB, Pillay JD, Plass D, Polinder S, Pond CD, Pope CA, Molinuevo A, Fresán U, Molina-Barceló A, Olmedo-Requena R,
Pope D, Popova S, Poulton RG, Pourmalek F, Prasad NM, Qorbani M, Tardón A, Alguacil J, Solans M, Huerta JM, Ruiz-Dominguez JM,
Rabiee RHS, Radfar A, Rafay A, Rahimi-Movaghar V, Rahman M, Aragonés N, Fernández-Villa T, Dierssen-Sotos T, Moreno V,
Rahman MHU, Rahman SU, Rai RK, Rajsic S, Raju M, Ram U, Rana SM, Guevara M, Vanaclocha-Espi M, Lozano-Lorca M, Fernández-
Ranganathan K, Rao P, García CAR, Refaat AH, Rehm CD, Rehm J, Tardón G, Castaño-Vinyals G, Pérez-Gómez B, Molina AJ, Llorca J,
Reinig N, Remuzzi G, Resnikoff S, Ribeiro AL, Rivera JA, Roba HS, Gil L, Castilla J, Pollán M, Kogevinas M, Amiano P. Consumption of
Downloaded from https://academic.oup.com/ajh/article/35/10/892/6617679 by guest on 03 November 2023
Rodriguez A, Rodriguez-Ramirez S, Rojas-Rueda D, Roman Y, ultra-processed foods and drinks and colorectal, breast, and prostate
Ronfani L, Roshandel G, Rothenbacher D, Roy A, Saleh MM, cancer. Clin Nutr 2021; 40:1537–1545.
Sanabria JR, Sanchez-Riera L, Sanchez-Niño MD, Sánchez- 17. Adjibade M, Julia C, Allès B, Touvier M, Lemogne C, Srour B,
Pimienta TG, Sandar L, Santomauro DF, Santos IS, Sarmiento-Suarez R, Hercberg S, Galan P, Assmann KE, Kesse-Guyot E. Prospective associ-
Sartorius B, Satpathy M, Savic M, Sawhney M, Schmidhuber J, ation between ultra-processed food consumption and incident depres-
Schmidt MI, Schneider IJC, Schöttker B, Schutte AE, Schwebel DC, sive symptoms in the French NutriNet-Santé cohort. BMC Med 2019;
Scott JG, Seedat S, Sepanlou SG, Servan-Mori EE, Shaddick G, 17:78.
Shaheen A, Shahraz S, Shaikh MA, Levy TS, Sharma R, She J, 18. Gómez-Donoso C, Sánchez-Villegas A, Martínez-González MA, Gea A,
Sheikhbahaei S, Shen J, Sheth KN, Shi P, Shibuya K, Shigematsu M, Mendonça RD, Lahortiga-Ramos F, Bes-Rastrollo M. Ultra-processed
Shin M-J, Shiri R, Shishani K, Shiue I, Shrime MG, Sigfusdottir ID, food consumption and the incidence of depression in a Mediterranean
Silva DAS, Silveira DGA, Silverberg JI, Simard EP, Sindi S, Singh A, cohort: the SUN Project. Eur J Nutr 2020; 59:1093–1103.
Singh JA, Singh PK, Slepak EL, Soljak M, Soneji S, Sorensen RJD, 19. Mozaffarian D, Hao T, Rimm EB, Willett WC, Hu FB. Changes in diet
Sposato LA, Sreeramareddy CT, Stathopoulou V, Steckling N, Steel N, and lifestyle and long-term weight gain in women and men. N Engl J
Stein DJ, Stein MB, Stöckl H, Stranges S, Stroumpoulis K, Sunguya BF, Med 2011; 364:2392–2404.
Swaminathan S, Sykes BL, Szoeke CEI, Tabarés-Seisdedos R, 20. Bertoia ML, Mukamal KJ, Cahill LE, Hou T, Ludwig DS, Mozaffarian D,
Takahashi K, Talongwa RT, Tandon N, Tanne D, Tavakkoli M, Taye BW, Willett WC, Hu FB, Rimm EB. Changes in intake of fruits and vegetables
Taylor HR, Tedla BA, Tefera WM, Tegegne TK, Tekle DY, Terkawi AS, and weight change in United States men and women followed for up
Thakur JS, Thomas BA, Thomas ML, Thomson AJ, Thorne-Lyman AL, to 24 years: analysis from three prospective cohort studies. PLoS Med
Thrift AG, Thurston GD, Tillmann T, Tobe-Gai R, Tobollik M, Topor- 2015; 12:e1001878.
Madry R, Topouzis F, Towbin JA, Tran BX, Dimbuene ZT, Tsilimparis N, 21. Alinia S, Hels O, Tetens I. The potential association between fruit intake
Tura AK, Tuzcu EM, Tyrovolas S, Ukwaja KN, Undurraga EA, and body weight—a review. Obes Rev 2009; 10:639–647.
Uneke CJ, Uthman OA, van Donkelaar A, van Os J, Varakin YY, 22. Ivancovsky-Wajcman D, Fliss-Isakov N, Webb M, Bentov I, Shibolet O,
Vasankari T, Veerman JL, Venketasubramanian N, Violante FS, Kariv R, Zelber-Sagi S. Ultra-processed food is associated with features
Vollset SE, Wagner GR, Waller SG, Wang JL, Wang L, Wang Y, of metabolic syndrome and non-alcoholic fatty liver disease. Liver Int
Weichenthal S, Weiderpass E, Weintraub RG, Werdecker A, 2021; 41:2635–2645.
Westerman R, Whiteford HA, Wijeratne T, Wiysonge CS, Wolfe CDA, 23. Lavigne-Robichaud M, Moubarac JC, Lantagne-Lopez S, Johnson-
Won S, Woolf AD, Wubshet M, Xavier D, Xu G, Yadav AK, Yakob B, Down L, Batal M, Laouan Sidi EA, Lucas M. Diet quality indices in
Yalew AZ, Yano Y, Yaseri M, Ye P, Yip P, Yonemoto N, Yoon S-J, relation to metabolic syndrome in an Indigenous Cree (Eeyouch)
Younis MZ, Yu C, Zaidi Z, Zaki MES, Zhu J, Zipkin B, Zodpey S, population in northern Québec, Canada. Public Health Nutr 2018;
Zuhlke LJ, Murray CJL. Global, regional, and national comparative risk 21:172–180.
assessment of 79 behavioural, environmental and occupational, and 24. Martínez Steele E, Juul F, Neri D, Rauber F, Monteiro CA. Dietary share
metabolic risks or clusters of risks, 1990–2015: a systematic analysis for of ultra-processed foods and metabolic syndrome in the US adult pop-
the Global Burden of Disease Study 2015. Lancet 2016; ulation. Prev Med 2019; 125:40–48.
388:1659–1724. 25. Mendonça RD, Lopes AC, Pimenta AM, Gea A, Martinez-
9. Srour B, Fezeu LK, Kesse-Guyot E, Allès B, Méjean C, Andrianasolo RM, Gonzalez MA, Bes-Rastrollo M. Ultra-processed food consumption
Chazelas E, Deschasaux M, Hercberg S, Galan P, Monteiro CA, Julia C, and the incidence of hypertension in a Mediterranean cohort: the
Touvier M. Ultra-processed food intake and risk of cardiovascular di- Seguimiento Universidad de Navarra Project. Am J Hypertens 2017;
sease: prospective cohort study (NutriNet-Santé). BMJ 2019; 365:l1451. 30:358–366.
10. Bonaccio M, Di Castelnuovo A, Costanzo S, De Curtis A, Persichillo M, 26. Monge A, Silva Canella D, López-Olmedo N, Lajous M, Cortés-
Sofi F, Cerletti C, Donati MB, de Gaetano G, Iacoviello L. Ultra- Valencia A, Stern D. Ultraprocessed beverages and processed meats
processed food consumption is associated with increased risk of all- increase the incidence of hypertension in Mexican women. Br J Nutr
cause and cardiovascular mortality in the Moli-sani Study. Am J Clin 2021; 126:600–611.
Nutr 2021; 113:446–455. 27. Nardocci M, Polsky JY, Moubarac JC. Consumption of ultra-processed
11. Blanco-Rojo R, Sandoval-Insausti H, López-Garcia E, Graciani A, foods is associated with obesity, diabetes and hypertension in Canadian
Ordovás JM, Banegas JR, Rodríguez-Artalejo F, Guallar-Castillón P. adults. Can J Public Health 2021; 112:421–429.
Consumption of ultra-processed foods and mortality: a National 28. Nasreddine L, Tamim H, Itani L, Nasrallah MP, Isma’eel H, Nakhoul NF,
Prospective Cohort in Spain. Mayo Clin Proc 2019; 94:2178–2188. Abou-Rizk J, Naja F. A minimally processed dietary pattern is associ-
12. Rico-Campà A, Martínez-González MA, Alvarez-Alvarez I, ated with lower odds of metabolic syndrome among Lebanese adults.
Mendonça RD, de la Fuente-Arrillaga C, Gómez-Donoso C, Bes- Public Health Nutr 2018; 21:160–171.
Rastrollo M. Association between consumption of ultra-processed 29. Rezende-Alves K, Hermsdorff HHM, Miranda AEDS, Lopes ACS,
foods and all cause mortality: SUN prospective cohort study. BMJ 2019; Bressan J, Pimenta AM. Food processing and risk of hypertension:
365:l1949. Cohort of Universities of Minas Gerais, Brazil (CUME Project). Public
13. Mendonça RD, Pimenta AM, Gea A, de la Fuente-Arrillaga C, Martinez- Health Nutr 2021; 24:4071–4079.
Gonzalez MA, Lopes AC, Bes-Rastrollo M. Ultraprocessed food con- 30. Scaranni PODS, Cardoso LO, Chor D, Melo ECP, Matos SMA, Giatti L,
sumption and risk of overweight and obesity: the University of Navarra Barreto SM, da Fonseca MJM. Ultra-processed foods, changes in blood
Follow-Up (SUN) cohort study. Am J Clin Nutr 2016; 104:1433–1440. pressure and incidence of hypertension: the Brazilian Longitudinal
900 American Journal of Hypertension 35(10) October 2022
Ultra-processed Foods and Hypertension
Study of Adult Health (ELSA-Brasil). Public Health Nutr 2021; 44. Hall KD. A review of the carbohydrate-insulin model of obesity. Eur J
24:3352–3360. Clin Nutr 2017; 71:323–326.
31. Pagliai G, Dinu M, Madarena MP, Bonaccio M, Iacoviello L, Sofi F. 45. Takeuchi M, Takino J, Furuno S, Shirai H, Kawakami M, Muramatsu M,
Consumption of ultra-processed foods and health status: a systematic Kobayashi Y, Yamagishi S. Assessment of the concentrations of various
review and meta-analysis. Br J Nutr 2021; 125:308–318. advanced glycation end-products in beverages and foods that are com-
32. Barbosa SS, Sousa LCM, de Oliveira Silva DF, Pimentel JB, monly consumed in Japan. PLoS One 2015; 10:e0118652.
Evangelista KCMS, Lyra CO, Lopes MMGD, Lima SCVC. A systematic 46. Uribarri J, Stirban A, Sander D, Cai W, Negrean M, Buenting CE,
review on processed/ultra-processed foods and arterial hypertension in Koschinsky T, Vlassara H. Single oral challenge by advanced glycation
adults and older people. Nutrients 2022; 14:1215. end products acutely impairs endothelial function in diabetic and
33. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, nondiabetic subjects. Diabetes Care 2007; 30:2579–2582.
Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, 47. Sharma C, Kaur A, Thind SS, Singh B, Raina S. Advanced glycation end-
Glanville J, Grimshaw JM, Hrobjartsson A, Lalu MM, Li T, Loder EW, products (AGEs): an emerging concern for processed food industries. J
Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Food Sci Technol 2015; 52:7561–7576.
Tricco AC, Welch VA, Whiting P, Moher D. The PRISMA 2020 state- 48. Feig DI, Soletsky B, Johnson RJ. Effect of allopurinol on blood pres-
ment: an updated guideline for reporting systematic reviews. Int J Surg sure of adolescents with newly diagnosed essential hypertension: a
2021; 88:105906. randomized trial. JAMA 2008; 300:924–932.
Downloaded from https://academic.oup.com/ajh/article/35/10/892/6617679 by guest on 03 November 2023
34. Askari M, Heshmati J, Shahinfar H, Tripathi N, Daneshzad E. Ultra- 49. Glushakova O, Kosugi T, Roncal C, Mu W, Heinig M, Cirillo P, Sánchez-
processed food and the risk of overweight and obesity: a systematic re- Lozada LG, Johnson RJ, Nakagawa T. Fructose induces the inflamma-
view and meta-analysis of observational studies. Int J Obes (Lond) 2020; tory molecule ICAM-1 in endothelial cells. J Am Soc Nephrol 2008;
44:2080–2091. 19:1712–1720.
35. Shivappa N, Godos J, Hebert JR, Wirth MD, Piuri G, Speciani AF, 50. Zhao CX, Xu X, Cui Y, Wang P, Wei X, Yang S, Edin ML, Zeldin DC,
Grosso G. Dietary inflammatory index and colorectal cancer risk-a Wang DW. Increased endothelial nitric-oxide synthase expression
meta-analysis. Nutrients 2017; 9:1043. reduces hypertension and hyperinsulinemia in fructose-treated rats. J
36. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta- Pharmacol Exp Ther 2009; 328:610–620.
analysis. Stat Med 2002; 21:1539–1558. 51. Brito JO, Ponciano K, Figueroa D, Bernardes N, Sanches IC,
37. Slimani N, Deharveng G, Southgate DA, Biessy C, Chajès V, Irigoyen MC, De Angelis K. Parasympathetic dysfunction is associated
van Bakel MM, Boutron-Ruault MC, McTaggart A, Grioni S, with insulin resistance in fructose-fed female rats. Braz J Med Biol Res
Verkaik-Kloosterman J, Huybrechts I, Amiano P, Jenab M, Vignat J, 2008; 41:804–808.
Bouckaert K, Casagrande C, Ferrari P, Zourna P, Trichopoulou A, 52. Singh AK, Amlal H, Haas PJ, Dringenberg U, Fussell S, Barone SL,
Wirfält E, Johansson G, Rohrmann S, Illner AK, Barricarte A, Engelhardt R, Zuo J, Seidler U, Soleimani M. Fructose-induced hyper-
Rodríguez L, Touvier M, Niravong M, Mulligan A, Crowe F, Ocké MC, tension: essential role of chloride and fructose absorbing transporters
van der Schouw YT, Bendinelli B, Lauria C, Brustad M, Hjartåker A, PAT1 and Glut5. Kidney Int 2008; 74:438–447.
Tjønneland A, Jensen AM, Riboli E, Bingham S. Contribution of highly 53. Louzada MLDC, Ricardo CZ, Steele EM, Levy RB, Cannon G,
industrially processed foods to the nutrient intakes and patterns of mid- Monteiro CA. The share of ultra-processed foods determines the
dle-aged populations in the European Prospective Investigation into overall nutritional quality of diets in Brazil. Public Health Nutr 2018;
Cancer and Nutrition study. Eur J Clin Nutr 2009; 63(Suppl 4):S206–S225. 21:94–102.
38. Qin P, Li Q, Zhao Y, Chen Q, Sun X, Liu Y, Li H, Wang T, Chen X, 54. Chassaing B, Koren O, Goodrich JK, Poole AC, Srinivasan S,
Zhou Q, Guo C, Zhang D, Tian G, Liu D, Qie R, Han M, Huang S, Ley RE, Gewirtz AT. Dietary emulsifiers impact the mouse gut mi-
Wu X, Li Y, Feng Y, Yang X, Hu F, Hu D, Zhang M. Sugar and artificially crobiota promoting colitis and metabolic syndrome. Nature 2015;
sweetened beverages and risk of obesity, type 2 diabetes mellitus, hy- 519:92–96.
pertension, and all-cause mortality: a dose-response meta-analysis of 55. Jang W, Jeoung NH, Cho KH. Modified apolipoprotein (apo) A–I
prospective cohort studies. Eur J Epidemiol 2020; 35:655–671. by artificial sweetener causes severe premature cellular senescence
39. Moradi S, Entezari MH, Mohammadi H, Jayedi A, Lazaridi AV, and atherosclerosis with impairment of functional and structural
Kermani MAH, Miraghajani M. Ultra-processed food consumption properties of apoA–I in lipid-free and lipid-bound state. Mol Cells
and adult obesity risk: a systematic review and dose-response meta- 2011; 31:461–470.
analysis. Crit Rev Food Sci Nutr 2021:1–12. 56. Stallings-Smith S, Mease A, Johnson TM, Arikawa AY. Exploring
40. Schulte EM, Avena NM, Gearhardt AN. Which foods may be addictive? the association between polycyclic aromatic hydrocarbons and
The roles of processing, fat content, and glycemic load. PLoS One 2015; diabetes among adults in the United States. Environ Res 2018;
10:e0117959. 166:588–594.
41. Lennerz BS, Alsop DC, Holsen LM, Stern E, Rojas R, Ebbeling CB, 57. Lee TW, Kim DH, Ryu JY. Association between urinary polycyclic
Goldstein JM, Ludwig DS. Effects of dietary glycemic index on brain aromatic hydrocarbons and hypertension in the Korean population:
regions related to reward and craving in men. Am J Clin Nutr 2013; data from the Second Korean National Environmental Health Survey
98:641–647. (2012–2014). Sci Rep 2020; 10:17142.
42. Thornley S, McRobbie H, Eyles H, Walker N, Simmons G. The obesity 58. Zhang Y, Huang M, Zhuang P, Jiao J, Chen X, Wang J, Wu Y. Exposure
epidemic: is glycemic index the key to unlocking a hidden addiction? to acrylamide and the risk of cardiovascular diseases in the National
Med Hypotheses 2008; 71:709–714. Health and Nutrition Examination Survey 2003–2006. Environ Int
43. Ebbeling CB, Leidig MM, Sinclair KB, Hangen JP, Ludwig DS. A 2018; 117:154–163.
reduced-glycemic load diet in the treatment of adolescent obesity. Arch 59. Feroe AG, Attanasio R, Scinicariello F. Acrolein metabolites, diabetes
Pediatr Adolesc Med 2003; 157:773–779. and insulin resistance. Environ Res 2016; 148:1–6.
American Journal of Hypertension 35(10) October 2022 901
You might also like
- Sremanakova Et Al-2018-Journal of Human Nutrition and DieteticsDocument11 pagesSremanakova Et Al-2018-Journal of Human Nutrition and DieteticsLulu BadriyahNo ratings yet
- Jurnal 1Document11 pagesJurnal 1Melda astrika sianiparNo ratings yet
- Agodi Et Al, 2018Document16 pagesAgodi Et Al, 2018Jesana LopesNo ratings yet
- DBT y Obs SarcopenicaDocument8 pagesDBT y Obs SarcopenicaestesiesundriveNo ratings yet
- Dairy Products and Health A Review of The Epidemiological EvidenceDocument6 pagesDairy Products and Health A Review of The Epidemiological EvidenceShell WattieNo ratings yet
- Effect of Eating Even or Odd Number of Dates, On Blood Glucose LevelDocument5 pagesEffect of Eating Even or Odd Number of Dates, On Blood Glucose LevelAlaaGaballaNo ratings yet
- Ultra-Processed Food Consumption and Metabolic Disease Risk: An Umbrella Review of Systematic Reviews With Meta-Analyses of Observational StudiesDocument16 pagesUltra-Processed Food Consumption and Metabolic Disease Risk: An Umbrella Review of Systematic Reviews With Meta-Analyses of Observational StudiesFernando Franco VargasNo ratings yet
- Fendo 13 1007557Document9 pagesFendo 13 1007557Isini sehansa amarathungaNo ratings yet
- 1 s2.0 S1051227619300020 MainDocument9 pages1 s2.0 S1051227619300020 MainRomário de Macedo EspíndolaNo ratings yet
- Ultraprocessed Foods and Excess Heart Age Among Us AdultsDocument10 pagesUltraprocessed Foods and Excess Heart Age Among Us AdultsSaionara FranciscoNo ratings yet
- Association of Dietary Pattern and Body Weight With Blood Pressure in Jiangsu Province, ChinaDocument8 pagesAssociation of Dietary Pattern and Body Weight With Blood Pressure in Jiangsu Province, ChinaNoval FarlanNo ratings yet
- Fruit and Vegetables Consumption and Incident HypertensionDocument8 pagesFruit and Vegetables Consumption and Incident HypertensionNathalia Rose Fransisca KarmaNo ratings yet
- Saturated Fat and Heart Disease American Journal of Clinical NutritionDocument12 pagesSaturated Fat and Heart Disease American Journal of Clinical Nutritionjackjensen2852No ratings yet
- Sugar and Artificially Sweetened Beverages Linked To Obesity: A Systematic Review and Meta-AnalysisDocument8 pagesSugar and Artificially Sweetened Beverages Linked To Obesity: A Systematic Review and Meta-AnalysisLorena ErnstNo ratings yet
- Fu RongDocument9 pagesFu RongTín NguyễnNo ratings yet
- Impact of Diet Composition On Blood GlucDocument51 pagesImpact of Diet Composition On Blood GlucNarasimha Pavan BNo ratings yet
- Chocolate Good For The Heart and BrainDocument8 pagesChocolate Good For The Heart and BrainVladimir ComagicNo ratings yet
- The Consumption of Milk and Dairy Foods and The IncidenceDocument15 pagesThe Consumption of Milk and Dairy Foods and The IncidenceZNNo ratings yet
- Atherosclerosis: Contents Lists Available atDocument9 pagesAtherosclerosis: Contents Lists Available atAngelica Scherlowski FassulaNo ratings yet
- Stress Hyperglycaemia in Critically Ill Patients and The Subsequent Risk of Diabetes: A Systematic Review and Meta-AnalysisDocument9 pagesStress Hyperglycaemia in Critically Ill Patients and The Subsequent Risk of Diabetes: A Systematic Review and Meta-Analysisnq qalbyNo ratings yet
- A 14-Cohort Meta-AnalysisDocument10 pagesA 14-Cohort Meta-AnalysisA'sHaikalNo ratings yet
- Fimmu 13 863640Document9 pagesFimmu 13 863640nugroho agung cahyonoNo ratings yet
- Dietary Habits of Wroclaw Medical UDocument10 pagesDietary Habits of Wroclaw Medical UJonah reiNo ratings yet
- PIIS2589537023000172Document12 pagesPIIS2589537023000172Gerry FonziNo ratings yet
- Serum Uric Acid Levels and Metabolic Indices inDocument9 pagesSerum Uric Acid Levels and Metabolic Indices indyane VatriciaNo ratings yet
- Prospective Study of Major Dietary Patterns and Risk of CoronaryDocument10 pagesProspective Study of Major Dietary Patterns and Risk of CoronaryJohn SammutNo ratings yet
- Journal Pre-Proofs: Diabetes Research and Clinical PracticeDocument35 pagesJournal Pre-Proofs: Diabetes Research and Clinical PracticeAzmafiNo ratings yet
- Song 2014Document11 pagesSong 2014Ayssa WitjaksonoNo ratings yet
- Jurnal 2Document10 pagesJurnal 2YulianiNo ratings yet
- Nutrients 12 00878Document13 pagesNutrients 12 00878Ardian AshadiNo ratings yet
- Comparison of High vs. Normal/Low Protein Diets On Renal Function in Subjects Without Chronic Kidney Disease: A Systematic Review and Meta-AnalysisDocument13 pagesComparison of High vs. Normal/Low Protein Diets On Renal Function in Subjects Without Chronic Kidney Disease: A Systematic Review and Meta-AnalysisAlex FabianNo ratings yet
- Novel Pathological Implications of Serum Uric Acid - 2023 - Diabetes Research AnDocument8 pagesNovel Pathological Implications of Serum Uric Acid - 2023 - Diabetes Research Analerta.bfcmNo ratings yet
- 2014 Article 157 PDFDocument18 pages2014 Article 157 PDFNabillah MukhlisNo ratings yet
- Prospective Investigation of Major Dietary PatternsDocument7 pagesProspective Investigation of Major Dietary PatternsJohn SammutNo ratings yet
- Ultra Processed Foods and Cardiovascular Diseases Poten - 2021 - Advances in NuDocument8 pagesUltra Processed Foods and Cardiovascular Diseases Poten - 2021 - Advances in NuMauricio RebolloNo ratings yet
- Di̇et CancerDocument9 pagesDi̇et Canceraselecz345No ratings yet
- Nmaa 108Document20 pagesNmaa 108fidya ardinyNo ratings yet
- Bmjopen 2016 014736Document6 pagesBmjopen 2016 014736puskesmas patuk satuNo ratings yet
- Diabetes research and clinical practice publishes global estimates of diabetes prevalenceDocument11 pagesDiabetes research and clinical practice publishes global estimates of diabetes prevalenceTiara Jauhara AzzahraNo ratings yet
- Hubungan Antara Kadar Asam Urat Dengan Indeks Massa Tubuh... (Ulfa F, Zuraida Z, Enggar W)Document10 pagesHubungan Antara Kadar Asam Urat Dengan Indeks Massa Tubuh... (Ulfa F, Zuraida Z, Enggar W)Enggar WijayantiNo ratings yet
- Journal of Critical Care: Biao Wang, MD, Gang Chen, MD, Yifei Cao, MD, Jiping Xue, MD, Jia Li, MD, Yunfu Wu, MDDocument5 pagesJournal of Critical Care: Biao Wang, MD, Gang Chen, MD, Yifei Cao, MD, Jiping Xue, MD, Jia Li, MD, Yunfu Wu, MDpramastutiNo ratings yet
- Wu Et Al., 2022 Association - Dietary - Spermidine - All-Cause - MortalityDocument9 pagesWu Et Al., 2022 Association - Dietary - Spermidine - All-Cause - MortalityPatrícia Felix ÁvilaNo ratings yet
- 337.1 s2.0 S0002916522046718 MainDocument10 pages337.1 s2.0 S0002916522046718 MaintereNo ratings yet
- Coffee Drinking Reduces Risk of Endometrial CancerDocument29 pagesCoffee Drinking Reduces Risk of Endometrial CancerMonica SáezNo ratings yet
- Buah Sayur5Document27 pagesBuah Sayur5AviasiNo ratings yet
- Diet Soft Drink Consumption Is Associated With The Metabolic Syndrome: A Two Sample ComparisonDocument18 pagesDiet Soft Drink Consumption Is Associated With The Metabolic Syndrome: A Two Sample ComparisonPK MilkyNo ratings yet
- Vegetarian, Vegan Diets Linked to Lower Heart Disease, Cancer RiskDocument50 pagesVegetarian, Vegan Diets Linked to Lower Heart Disease, Cancer RiskFilipa FerreiraNo ratings yet
- Prevalence and Predictors of Gastritis Among Patients Attending Health Care Facilities in Jazan, KSADocument8 pagesPrevalence and Predictors of Gastritis Among Patients Attending Health Care Facilities in Jazan, KSAShirleyNo ratings yet
- Efficacy of Dietary Interventions in End-Stage Renal Disease Patients A Systematic ReviewDocument13 pagesEfficacy of Dietary Interventions in End-Stage Renal Disease Patients A Systematic ReviewKhusnu Waskithoningtyas NugrohoNo ratings yet
- 1 s2.0 S2001037021000751 Main PDFDocument27 pages1 s2.0 S2001037021000751 Main PDFغاز الشمالNo ratings yet
- Review ArticleDocument9 pagesReview ArticlefelipetheNo ratings yet
- Artigo POX TXDocument18 pagesArtigo POX TXescoladealimentacao2No ratings yet
- (Diabetes - Metabolism Research and Reviews 2017-Dec 19 Vol. 34 Iss. 2) Hou, Xuhong - Chen, Peizhu - Hu, Gang - Chen, Yue - Chen, Siyu - Wu, - Distribution and Related Factors of CardiomDocument32 pages(Diabetes - Metabolism Research and Reviews 2017-Dec 19 Vol. 34 Iss. 2) Hou, Xuhong - Chen, Peizhu - Hu, Gang - Chen, Yue - Chen, Siyu - Wu, - Distribution and Related Factors of CardiomEshetu WondimuNo ratings yet
- 2020 UPFs Obesity Metaanalysis IJODocument12 pages2020 UPFs Obesity Metaanalysis IJOKelly Viviana Gaitan OyolaNo ratings yet
- Veronese, N 2019Document8 pagesVeronese, N 2019Nicolás MurilloNo ratings yet
- Whole Grains May Lower Liver Cancer RiskDocument11 pagesWhole Grains May Lower Liver Cancer RiskrahmaNo ratings yet
- 2017 Article 405Document11 pages2017 Article 405Kornelis AribowoNo ratings yet
- Sugar-Sweetened Beverages and Weight Gain in Children and Adults: A Systematic Review and Meta-AnalysisDocument19 pagesSugar-Sweetened Beverages and Weight Gain in Children and Adults: A Systematic Review and Meta-AnalysisLorena ErnstNo ratings yet
- Consumption of Sugars, Sugary Foods, And Sugary Beverages in Relation to Adiposity- Related Cancer Risk in the Framingham Offspring Cohort (1991–2013)Document12 pagesConsumption of Sugars, Sugary Foods, And Sugary Beverages in Relation to Adiposity- Related Cancer Risk in the Framingham Offspring Cohort (1991–2013)Maria Vitória Cota de AbreuNo ratings yet
- First Responders: The Heroes Who Answer Emergency CallsDocument11 pagesFirst Responders: The Heroes Who Answer Emergency CallsDIANA MARIE MOTA ABREUNo ratings yet
- Kounis Syndrome A Pediatric PerspectiveDocument10 pagesKounis Syndrome A Pediatric PerspectiveAna Belén Artero CastañoNo ratings yet
- Ovate PDFDocument11 pagesOvate PDFAriPratiwiNo ratings yet
- Mobility - RIOSDocument122 pagesMobility - RIOSangemcpo08No ratings yet
- Specialized Group Homes For Persons With Severe or Profound Mental Retardation and Serious Problem Behaviour in EnglandDocument18 pagesSpecialized Group Homes For Persons With Severe or Profound Mental Retardation and Serious Problem Behaviour in EnglandDeborah RiskinNo ratings yet
- Medically Compromised Patients in Prosthodontics - 818 (Autosaved)Document22 pagesMedically Compromised Patients in Prosthodontics - 818 (Autosaved)Suraj ShahNo ratings yet
- 2017 (Laporan Pelayanan Rawat Jalan Dr. Ida Ayu Anom Margareni)Document11 pages2017 (Laporan Pelayanan Rawat Jalan Dr. Ida Ayu Anom Margareni)Anggi RiyaniNo ratings yet
- A Century of Biological-Weapons Programs (1915-2015) : Reviewing The EvidenceDocument26 pagesA Century of Biological-Weapons Programs (1915-2015) : Reviewing The EvidenceCaio CesarNo ratings yet
- Pharma Laboratory ExperimentsDocument34 pagesPharma Laboratory Experimentsapi-3748748100% (4)
- Case Presentation - Group 9 - B - Medix Medical HospitalDocument31 pagesCase Presentation - Group 9 - B - Medix Medical HospitalChantemayne VillanuevaNo ratings yet
- Community Question Bank (N.a)Document41 pagesCommunity Question Bank (N.a)Sumaya AfifyNo ratings yet
- Patients Profile M 3Document4 pagesPatients Profile M 3Longyapon Sheena StephanieNo ratings yet
- Pneumothoraks Jurnal RadiologiDocument9 pagesPneumothoraks Jurnal RadiologiRachmi MerrinaNo ratings yet
- Microbiologist: 3.1.5 Isolation & Gram StainingDocument5 pagesMicrobiologist: 3.1.5 Isolation & Gram Stainingapi-534896073No ratings yet
- Addressing Barriers, Stigma and Discrimination Surrounding HIV and Viral HepatitisDocument17 pagesAddressing Barriers, Stigma and Discrimination Surrounding HIV and Viral HepatitisAlemayehu KebedeNo ratings yet
- Nejmoa1901814 AppendixDocument29 pagesNejmoa1901814 AppendixMuhammad AbdurrosyidNo ratings yet
- Guidelines for diagnosing and treating hypothyroidismDocument43 pagesGuidelines for diagnosing and treating hypothyroidismJoseAbdalaNo ratings yet
- امتحان ENT دفعة ٣١Document14 pagesامتحان ENT دفعة ٣١محمد عبد القاهر السروريNo ratings yet
- Garner 1511222Document17 pagesGarner 1511222Bj LongNo ratings yet
- Activity - Nutrition On The Internet Worksheet 3Document2 pagesActivity - Nutrition On The Internet Worksheet 3Carlo FernandoNo ratings yet
- Heavenly Spa MenuDocument2 pagesHeavenly Spa MenuDeTaaliNo ratings yet
- Comprehensive Geriatric Assessment FormDocument13 pagesComprehensive Geriatric Assessment FormJojo Binay0% (1)
- Uts Advocacy PaperDocument11 pagesUts Advocacy PaperPlu AldiniNo ratings yet
- A Study of Stigma and Discrimination Towards People Living With Hiv/AidsDocument20 pagesA Study of Stigma and Discrimination Towards People Living With Hiv/Aidsmusamuwaga100% (1)
- Laporan Jaga Perina Selasa Malam EditDocument15 pagesLaporan Jaga Perina Selasa Malam EditmuhammadrikiNo ratings yet
- PBL Modul 2 TropisDocument31 pagesPBL Modul 2 TropiskasmaNo ratings yet
- OVPR FY20Q1 Proposal List PDFDocument45 pagesOVPR FY20Q1 Proposal List PDFtsuregiNo ratings yet
- Traditional Zootherapeutic Uses in The Treatment of Asthma by The Ethnic Groups of Assam, IndiaDocument5 pagesTraditional Zootherapeutic Uses in The Treatment of Asthma by The Ethnic Groups of Assam, IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Nursing Process Assessment (Revised Jones Criteria (American Heart Association)Document32 pagesNursing Process Assessment (Revised Jones Criteria (American Heart Association)Mamot MotNo ratings yet
- Podcast Script "Hustle Culture" OPENING: Haiii I'am Hidayah Malika and Welcome To Speak Up' PodcastDocument3 pagesPodcast Script "Hustle Culture" OPENING: Haiii I'am Hidayah Malika and Welcome To Speak Up' PodcastMas'adatul HidayahNo ratings yet