South/South West Hospital Group
Bantry General Hospital (AFFIX PATIENT LABEL HERE)
D CONSTIPATION
D DIARRHOEA
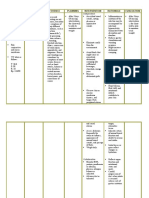
Related to: Interventions:
NURSING OUTCOME: BOWEL ELIMINATION Staff document each intervention during the shift, with a for
Tick relevant outcome indicator from the list. care given, N/A or for variance. For findings,
(i) Elimination pattern Control of bowel movements Stool colour document on the evaluation and record of MDT Communication
sheet as it occurs and sign date and time entry.
Stool soft and formed Ease of stool passage
Reassess as the patient’s condition dictates.
Passage of stool without aids
(i) Compromised Each date covers the 24-hour period from
Severely Substantially Moderately Mildly Not 0800-0800hrs
1 2 3 4 5
(ii) Blood in stool Mucous in stool Date:
Constipation Diarrhoea Pain with passage of stool
(ii) Severity
Severe Substantial Moderate Mild None
DAY DAY DAY DAY DAY DAY DAY
1 2 3 4 5
Patient’s overall rating on initial assessment (1-5) ................................................ Time:
Optimum nursing outcome target rating (1-5) ? .......................................................
How often is the rating to be measured ? ................................................................ NIGHT NIGHT NIGHT NIGHT NIGHT NIGHT NIGHT
Explain all procedures and care to patient and family as appropriate offering
psychological support and reassurance.
Bowel pattern is monitored and recorded daily.
Attend to personal hygiene needs as appropriate
maintaining dignity and privacy.
>If the patient is constipated, laxatives are administered as prescribed and
the patient’s response is monitored and recorded.
>If the patient is incontinent, appropriate incontinence aids are used
Type and size of aid _______________.
>If the patient has diarrhea, motion type is documented using the Bristol
Stool Chart.
> A referral for dietary assessment is completed.
sign once completed
If applicable,
> A 24 hourly fluid intake and output chart is maintained.
> Report abnormal clinical findings to Medical Team.
> Administer prescribed medications and monitor effectiveness of same.
> Record intake/output chart reporting any deviations from normal.
>If diarrhoea present, consider appropriate infection control interventions
as per BGH hospital policy. Liase with infection control CNS.
Nursing Outcome rating is? (insert rating where applicable)
Signed by
Countersigned by RN (if applicable)
Every effort has been made to ensure a Therapeutic Milieu
Date Nursing Diagnosis closed _________________ Signed ______________________ Countersigned _______________________
Date Nursing Diagnosis reopened (if applicable) _________________ Signed ______________________ Countersigned __________________
Date Nursing Diagnosis closed (if applicable) _________________ Signed ______________________ Countersigned _______________________
Ref: Nursing Diagnosis: Herdman and Kamitsuru, 2018: Nursing Outcomes Classification: Moorhead et al, 2018
� South/South West Hospital Group
Bantry General Hospital (AFFIX PATIENT LABEL HERE)
D CONSTIPATION
D DIARRHOEA
Related to: Interventions:
NURSING OUTCOME: BOWEL ELIMINATION Staff document each intervention during the shift, with a for
Tick relevant outcome indicator from the list. care given, N/A or for variance. For findings,
(i) Elimination pattern Control of bowel movements Stool colour document on the evaluation and record of MDT Communication
sheet as it occurs and sign date and time entry.
Stool soft and formed Ease of stool passage
Reassess as the patient’s condition dictates.
Passage of stool without aids
(i) Compromised Each date covers the 24-hour period from
Severely Substantially Moderately Mildly Not 0800-0800hrs
1 2 3 4 5
(ii) Blood in stool Mucous in stool Date:
Constipation Diarrhoea Pain with passage of stool
(ii) Severity
Severe Substantial Moderate Mild None
DAY DAY DAY DAY DAY DAY DAY
1 2 3 4 5
Patient’s overall rating on initial assessment (1-5) ................................................ Time:
Optimum nursing outcome target rating (1-5) ? .......................................................
How often is the rating to be measured ? ................................................................ NIGHT NIGHT NIGHT NIGHT NIGHT NIGHT NIGHT
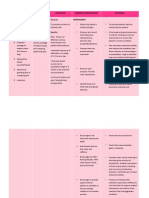
Explain all procedures and care to patient and family as appropriate offering
psychological support and reassurance.
Bowel pattern is monitored and recorded daily.
Attend to personal hygiene needs as appropriate
maintaining dignity and privacy.
>If the patient is constipated, laxatives are administered as prescribed and
the patient’s response is monitored and recorded.
>If the patient is incontinent, appropriate incontinence aids are used
Type and size of aid _______________.
>If the patient has diarrhea, motion type is documented using the Bristol
Stool Chart.
> A referral for dietary assessment is completed.
sign once completed
If applicable,
> A 24 hourly fluid intake and output chart is maintained.
> Report abnormal clinical findings to Medical Team.
> Administer prescribed medications and monitor effectiveness of same.
> Record intake/output chart reporting any deviations from normal.
>If diarrhoea present, consider appropriate infection control interventions
as per BGH hospital policy. Liase with infection control CNS.
Nursing Outcome rating is? (insert rating where applicable)
Signed by
Countersigned by RN (if applicable)
Every effort has been made to ensure a Therapeutic Milieu
Date Nursing Diagnosis closed _________________ Signed ______________________ Countersigned _______________________
Date Nursing Diagnosis reopened (if applicable) _________________ Signed ______________________ Countersigned __________________
Date Nursing Diagnosis closed (if applicable) _________________ Signed ______________________ Countersigned _______________________
Ref: Nursing Diagnosis: Herdman and Kamitsuru, 2018: Nursing Outcomes Classification: Moorhead et al, 2018