0% found this document useful (0 votes)
875 views1 pageClinical Abstract Application Form
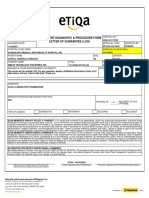
This document contains an application form for a medical report from a hospital or clinic. It notes that the form must be completed by the patient or their legal guardian if the patient is under 18. It authorizes the doctor in charge to provide a detailed medical report including test results to the insurance company for the patient's insurance application. The patient or guardian must sign the form and it must be witnessed by another person providing their signature and contact details.
Uploaded by
cachoydapCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
875 views1 pageClinical Abstract Application Form
This document contains an application form for a medical report from a hospital or clinic. It notes that the form must be completed by the patient or their legal guardian if the patient is under 18. It authorizes the doctor in charge to provide a detailed medical report including test results to the insurance company for the patient's insurance application. The patient or guardian must sign the form and it must be witnessed by another person providing their signature and contact details.
Uploaded by
cachoydapCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd