You might also like
- A Rare and Fatal Case of Nasogastric Tube.492Document1 pageA Rare and Fatal Case of Nasogastric Tube.492Stefania Szeibert-KerekesNo ratings yet
- Unexplained Ascites, A Sign For Neuroendocrine Carcinoma: Case ReportDocument3 pagesUnexplained Ascites, A Sign For Neuroendocrine Carcinoma: Case ReportsandzatNo ratings yet
- Tumor in The Pancreatic Head: A Case ReportDocument2 pagesTumor in The Pancreatic Head: A Case ReportAnti TjahyaNo ratings yet
- Tumor in The Pancreatic Head: A Case ReportDocument2 pagesTumor in The Pancreatic Head: A Case ReportAnti TjahyaNo ratings yet
- A Giant Simple Hepatic Cyst With Chronic ConstipationDocument2 pagesA Giant Simple Hepatic Cyst With Chronic ConstipationJapanese Journal of Gastroenterology and HepatologyNo ratings yet
- Lecture 3.5 Acute Abdomen in Gastrointenstinal-Dr. Adeodatus Yudha Handaya, SP.-KBD (2020)Document63 pagesLecture 3.5 Acute Abdomen in Gastrointenstinal-Dr. Adeodatus Yudha Handaya, SP.-KBD (2020)stefany huangNo ratings yet
- Dynamic CT Findings of A Polypoid Gastric - ChrisnaDocument4 pagesDynamic CT Findings of A Polypoid Gastric - ChrisnaferonicaNo ratings yet
- 97438-Article Text-254324-1-10-20131121Document2 pages97438-Article Text-254324-1-10-20131121June Faith HacheroNo ratings yet
- PancreatoblastomaDocument16 pagesPancreatoblastomaDr Farman AliNo ratings yet
- DuodenalcarcinoidDocument5 pagesDuodenalcarcinoidMudassar SattarNo ratings yet
- An Enteral Therapy Containing MCT and Hydrolyzed Peptides Reduces Postprandial Pain Associated With Chronic PancreatitisDocument5 pagesAn Enteral Therapy Containing MCT and Hydrolyzed Peptides Reduces Postprandial Pain Associated With Chronic PancreatitisSandra RodriguezNo ratings yet
- 2020 Paper SplenicDocument5 pages2020 Paper SplenicLauburu CrossNo ratings yet
- Ca 3Document4 pagesCa 3TUGAS ILMIAHNo ratings yet
- Gallbladder Carcinoma Presenting As Right Upper Quadrant Pain: A Case ReportDocument19 pagesGallbladder Carcinoma Presenting As Right Upper Quadrant Pain: A Case ReportMacky YongcoNo ratings yet
- Ce 48 291Document6 pagesCe 48 291Siska HarapanNo ratings yet
- Cancro GastricoDocument6 pagesCancro GastricoDani SNo ratings yet
- Groove Pancreatitis: A Rare Case SeriesDocument4 pagesGroove Pancreatitis: A Rare Case SeriesJothiprasad VenkatesanNo ratings yet
- HepatomaDocument33 pagesHepatomaRozen RyuhaNo ratings yet
- Clinical+Algorithms+in+General+Surgery Gastric CancerDocument3 pagesClinical+Algorithms+in+General+Surgery Gastric CancerGeorge GeorgakisNo ratings yet
- Radiol 2018181353Document9 pagesRadiol 2018181353Dev KansaraNo ratings yet
- Mixed Adenoneuroendocrine Carcinoma of The Gallbladder: Case PresentationDocument3 pagesMixed Adenoneuroendocrine Carcinoma of The Gallbladder: Case PresentationGeorgiana WltNo ratings yet
- Sister Mary Joseph Nodule As Cutaneous.9Document3 pagesSister Mary Joseph Nodule As Cutaneous.9Fernando MartinezNo ratings yet
- Hepatobiliary and Pancreatic: Recurrent Pancreatitis Caused by A Solid Pseudopapillary Neoplasm of The PancreasDocument1 pageHepatobiliary and Pancreatic: Recurrent Pancreatitis Caused by A Solid Pseudopapillary Neoplasm of The PancreasIvan Louis ToledoNo ratings yet
- ACPGBI CRC Part 2Document9 pagesACPGBI CRC Part 2NevilleNo ratings yet
- Tumor - Duodenal - 2022Document4 pagesTumor - Duodenal - 2022Berenice SanchezNo ratings yet
- Fonc 13 1155233Document6 pagesFonc 13 1155233Setiaty PandiaNo ratings yet
- JGH 13174Document9 pagesJGH 13174samudraandiNo ratings yet
- 175 700 1 PBDocument2 pages175 700 1 PBEva ParamithaNo ratings yet
- Clinical Utility of MRCP in Biliary Disease.2653Document2 pagesClinical Utility of MRCP in Biliary Disease.2653Ilham BelgaNo ratings yet
- Synchronous Pancreatic Neuroendocrine Tumor and Pancreatic Cyst A Case ReportDocument4 pagesSynchronous Pancreatic Neuroendocrine Tumor and Pancreatic Cyst A Case ReportWorld Journal of Clinical SurgeryNo ratings yet
- A Case of Breast Cancer Metastasis To Gi TractDocument4 pagesA Case of Breast Cancer Metastasis To Gi TractbecksNo ratings yet
- 492 568 1 SMnjsjsdjsDocument4 pages492 568 1 SMnjsjsdjsZidna MazayatulNo ratings yet
- Diagnosis and Management of Chronic PancreatitisDocument8 pagesDiagnosis and Management of Chronic PancreatitiscarmenNo ratings yet
- Pancreatic Adenocarcinoma Mimicking PseudocystDocument3 pagesPancreatic Adenocarcinoma Mimicking PseudocystInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Ovarian CancerDocument3 pagesOvarian Cancerasoly giovanoNo ratings yet
- 010 - Past - Present - and-Future-Management-of-Locali - 2023 - Surgical-Oncology-ClinicDocument17 pages010 - Past - Present - and-Future-Management-of-Locali - 2023 - Surgical-Oncology-ClinicDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Radiation Proctitis Major Case Study Powerpoint FinalizedDocument22 pagesRadiation Proctitis Major Case Study Powerpoint Finalizedapi-634988720No ratings yet
- PA - Gastroenterology - 2013 - Jun - 144 (6) - 1272Document10 pagesPA - Gastroenterology - 2013 - Jun - 144 (6) - 1272Lourianne NcNo ratings yet
- Seminar: Definition of Chronic PancreatitisDocument14 pagesSeminar: Definition of Chronic PancreatitisCarlos Alberto Torres LópezNo ratings yet
- Fibrolamellar Variant of Hepatocellular Carcinoma in A Young FemaleDocument3 pagesFibrolamellar Variant of Hepatocellular Carcinoma in A Young FemaleIKIKIKIKIKI999999No ratings yet
- Caz Bun 7Document2 pagesCaz Bun 7Dumitru RadulescuNo ratings yet
- (The Clinics - Surgery) Steve Behrman MD FACS, Ron Martin MD FACS - Modern Concepts in Pancreatic Surgery, An Issue of Surgical Clinics, 1e (2013, Elsevier)Document197 pages(The Clinics - Surgery) Steve Behrman MD FACS, Ron Martin MD FACS - Modern Concepts in Pancreatic Surgery, An Issue of Surgical Clinics, 1e (2013, Elsevier)Yee Wei HoongNo ratings yet
- 2007-03 - Intestinal Autotransplantation For Adenocarcinoma of Pancreas Involving The Mesenteric Root - Our Experience and Literature Review PDFDocument3 pages2007-03 - Intestinal Autotransplantation For Adenocarcinoma of Pancreas Involving The Mesenteric Root - Our Experience and Literature Review PDFNawzad SulayvaniNo ratings yet
- Ly2016ly2016 001Document2 pagesLy2016ly2016 001363331272No ratings yet
- Clinical ManagementDocument10 pagesClinical Managementpruebaprueba321765No ratings yet
- International Journal of Surgery Case ReportsDocument4 pagesInternational Journal of Surgery Case ReportsSulaeman Andrianto SusiloNo ratings yet
- Primary Gastric Choriocarcinoma: A Case Report and Review of The LiteratureDocument4 pagesPrimary Gastric Choriocarcinoma: A Case Report and Review of The LiteratureFeby HidasariNo ratings yet
- HIPECDocument38 pagesHIPECPrasanth NarayananNo ratings yet
- Can The Computed Tomography Severity Index Be A Prognostic Tool in Acute Gallstone-Induced PancreatitisDocument4 pagesCan The Computed Tomography Severity Index Be A Prognostic Tool in Acute Gallstone-Induced PancreatitisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Metastatic Pancreatic Carcinoid Tumor With GOODocument10 pagesMetastatic Pancreatic Carcinoid Tumor With GOOMohamed HadzriNo ratings yet
- 1.2.2. Emergency Abdominal ImagingDocument51 pages1.2.2. Emergency Abdominal ImagingNoura AdzmiaNo ratings yet
- CE (Ra1) F (KM) PF1 (AKA KM) GC (Su SL) PN (SL)Document3 pagesCE (Ra1) F (KM) PF1 (AKA KM) GC (Su SL) PN (SL)qrscentralNo ratings yet
- Cancer GastricoDocument8 pagesCancer GastricoAlex Escobar GavilánNo ratings yet
- Esophageal DiseasesDocument3 pagesEsophageal DiseasesAdilMoumnaNo ratings yet
- Friday Green Surgery Presentation: Anooj PatelDocument32 pagesFriday Green Surgery Presentation: Anooj PatelaNo ratings yet
- Paraneoplastic Hypercalcaemia As A Cause of Unexplained Renal Impairment in A Patient With Seminoma A Case ReportDocument5 pagesParaneoplastic Hypercalcaemia As A Cause of Unexplained Renal Impairment in A Patient With Seminoma A Case Reportkshwel.pNo ratings yet
- DCR 64 1471Document8 pagesDCR 64 1471juan uribeNo ratings yet
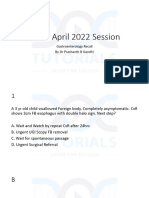
- INI SS April 2022 Gastro RecallDocument106 pagesINI SS April 2022 Gastro Recallgirishkiran23No ratings yet
- 6 Day Pediatric PancreatitisDocument16 pages6 Day Pediatric PancreatitisShreyash HaritwalNo ratings yet
- Current Challenges with their Evolving Solutions in Surgical Practice in West Africa: A ReaderFrom EverandCurrent Challenges with their Evolving Solutions in Surgical Practice in West Africa: A ReaderNo ratings yet
- Contemporary India and The WorldDocument1 pageContemporary India and The WorldApurva SinghNo ratings yet
- Framing Marriage: Consumption, Morality A N D Sexuality in Hum Aapke HainkaunDocument85 pagesFraming Marriage: Consumption, Morality A N D Sexuality in Hum Aapke HainkaunApurva SinghNo ratings yet
- E-Commerce Is Fast Becoming The Default Option For Shopping in India - The Economic TimesDocument7 pagesE-Commerce Is Fast Becoming The Default Option For Shopping in India - The Economic TimesApurva SinghNo ratings yet
- Drafting SampleDocument3 pagesDrafting SampleApurva SinghNo ratings yet
- Century of The Self Transcript: Part One: Happiness MachinesDocument55 pagesCentury of The Self Transcript: Part One: Happiness MachinesApurva SinghNo ratings yet
- Builders Association of IndiaDocument9 pagesBuilders Association of IndiaApurva SinghNo ratings yet
- Schedule For External Examination - October 2018 and April 2019 Season - BA-BBA. LL.B. - Academic Year 2018-19Document4 pagesSchedule For External Examination - October 2018 and April 2019 Season - BA-BBA. LL.B. - Academic Year 2018-19Apurva SinghNo ratings yet
- Diabetes Dan PJK, Farmasi DR - DjokoDocument39 pagesDiabetes Dan PJK, Farmasi DR - DjokoimbangNo ratings yet
- Simplify Insulin Therapy With Co-FormulationDocument26 pagesSimplify Insulin Therapy With Co-FormulationNatasha LaurentiaNo ratings yet
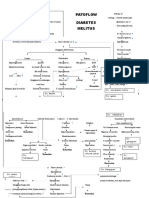
- Pathway DMDocument2 pagesPathway DMBang KiraNo ratings yet
- Benedict's and Heat and Acetic Acid TestDocument2 pagesBenedict's and Heat and Acetic Acid Testgilissa100% (1)
- OET Practice Reading Test Part A:: The ContinuesDocument8 pagesOET Practice Reading Test Part A:: The ContinuesPrasoon PremrajNo ratings yet
- Lack of Knowledge On Diabetes Management or Blood Glucose ManagementDocument2 pagesLack of Knowledge On Diabetes Management or Blood Glucose ManagementDanica Kate GalleonNo ratings yet
- Type 2 Diabetes in The Young The Evolving EpidemicDocument15 pagesType 2 Diabetes in The Young The Evolving EpidemicrodtobingNo ratings yet
- Ginni Rani NewDocument41 pagesGinni Rani NewEkta RajputNo ratings yet
- DR Che Writing Correction Oet General NoteDocument139 pagesDR Che Writing Correction Oet General NoteNitesh GandhiNo ratings yet
- Diabetes AssignmentDocument8 pagesDiabetes AssignmentMildred Obeng AgyeiwaaNo ratings yet
- Gestational Diabetes - Case Study 2Document13 pagesGestational Diabetes - Case Study 2Bb RabbitNo ratings yet
- Journal - A Review of Diabetes MellitusDocument6 pagesJournal - A Review of Diabetes Mellitusifaans16No ratings yet
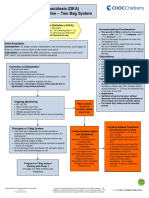
- Diabetic Ketoacidosis Care GuidelineDocument5 pagesDiabetic Ketoacidosis Care GuidelineRahma DhNo ratings yet
- 6.diabetes Education in ChilDocument9 pages6.diabetes Education in ChilWahyu Dwi NugrohoNo ratings yet
- Diabetic Prevention ProjectDocument6 pagesDiabetic Prevention ProjectStephen NdireNo ratings yet
- Capillary Blood Glucose TestingDocument4 pagesCapillary Blood Glucose TestingJUVIELY PREMACIONo ratings yet
- Protocol 005Document18 pagesProtocol 005Abo-ahmed ElmasryNo ratings yet
- Risk of OSA in DM Type 2 PatientsDocument9 pagesRisk of OSA in DM Type 2 Patientskryshna maqNo ratings yet
- Diabetic KetoacidosisDocument5 pagesDiabetic KetoacidosisJamie IllmaticNo ratings yet
- Hypoglycemia After Gastric Bypass Surgery. Current Concepts and Controversies 2018Document12 pagesHypoglycemia After Gastric Bypass Surgery. Current Concepts and Controversies 2018Rio RomaNo ratings yet
- Uae SST Notes (PT-3)Document2 pagesUae SST Notes (PT-3)Vanessa DamaniNo ratings yet
- The Pancreas: Anatomy and FunctionsDocument10 pagesThe Pancreas: Anatomy and FunctionsPunx RamoneNo ratings yet
- (Đề thi có 04 trang) Thời gian làm bài: 60 phút không kể thời gian phát đềDocument5 pages(Đề thi có 04 trang) Thời gian làm bài: 60 phút không kể thời gian phát đềMon MonNo ratings yet
- 418rle-M2-Ru9 Case Scenario Dka Vs HhsDocument4 pages418rle-M2-Ru9 Case Scenario Dka Vs Hhs1S VILLEGAS GabrielNo ratings yet
- Drugs For Diabetes (Part 1)Document6 pagesDrugs For Diabetes (Part 1)حوراء عارف الموسويNo ratings yet
- GUANTIA Activity Proposal - BIKING For WELLNESSDocument7 pagesGUANTIA Activity Proposal - BIKING For WELLNESSJofit DayocNo ratings yet
- Antidiabetic Potential of Acanthaceae Family: Review ArticleDocument8 pagesAntidiabetic Potential of Acanthaceae Family: Review ArticleWulan Klsb6No ratings yet
- Bio-Rad D-10 Dual ProgramDocument15 pagesBio-Rad D-10 Dual ProgramMeesam AliNo ratings yet
- APJTBMPublicationDocument7 pagesAPJTBMPublicationsiti zuhri ramdaniNo ratings yet
- Hypoglycemia in NewbornDocument10 pagesHypoglycemia in Newbornmaxim tomuNo ratings yet