You might also like
- Risk Management and the Emergency Department: Executive Leadership for Protecting Patients and HospitalsFrom EverandRisk Management and the Emergency Department: Executive Leadership for Protecting Patients and HospitalsNo ratings yet
- 11 ArticuloDocument9 pages11 ArticuloNia MoonNo ratings yet
- Data Makes the Difference: The Smart Nurse's Handbook for Using Data to Improve CareFrom EverandData Makes the Difference: The Smart Nurse's Handbook for Using Data to Improve CareNo ratings yet
- Patient Safety in The NICUDocument10 pagesPatient Safety in The NICUINGRID YISEL IDROBO AGREDONo ratings yet
- Attributable To The Use of Medications (: Near MissesDocument4 pagesAttributable To The Use of Medications (: Near MissesdudijohNo ratings yet
- Jurnal LainDocument22 pagesJurnal LainBudi ArsanaNo ratings yet
- Reporting Medical Errors To Improve Patient Safety: A Survey of Physicians in Teaching HospitalsDocument7 pagesReporting Medical Errors To Improve Patient Safety: A Survey of Physicians in Teaching HospitalsDanily Faith VillarNo ratings yet
- Improving Medicines Management Guide Prevents HarmDocument49 pagesImproving Medicines Management Guide Prevents HarmSulfia ArifahNo ratings yet
- Wrong Medication Near-Miss Analysis (NursingDocument10 pagesWrong Medication Near-Miss Analysis (NursingMaina PeterNo ratings yet
- Medication Error Patients Admitted To Medical Ward in Primary Hospital, Ethiopia: Prospective Obserbetional StudyDocument18 pagesMedication Error Patients Admitted To Medical Ward in Primary Hospital, Ethiopia: Prospective Obserbetional StudybezieNo ratings yet
- Polypharmacy and Drug-Related Problems Among People Living With HIV-AIDS - A Single-Center Experience (#577802) - 735759Document8 pagesPolypharmacy and Drug-Related Problems Among People Living With HIV-AIDS - A Single-Center Experience (#577802) - 735759LauraNo ratings yet
- Hewison NURSES IDENTIFICATION AND REPORTING OF MEDICATION ERRORS Journal Clinical NursingDocument17 pagesHewison NURSES IDENTIFICATION AND REPORTING OF MEDICATION ERRORS Journal Clinical NursingCatrin_HutaurukNo ratings yet
- Medication Errors in An Intensive Care Unit: OriginalresearchDocument10 pagesMedication Errors in An Intensive Care Unit: OriginalresearchFauziah AizulNo ratings yet
- Journal Pone 0249531Document16 pagesJournal Pone 0249531Integração da Assistência à Saúde Militar (INASMIL)No ratings yet
- Abostrofic SytosisDocument17 pagesAbostrofic Sytosisasaad biqaiNo ratings yet
- Principle of Medication SafetyDocument8 pagesPrinciple of Medication SafetyChakra PuspitaNo ratings yet
- Effects of A Patient Handover Intervention On Rates of Medical ErrorsDocument3 pagesEffects of A Patient Handover Intervention On Rates of Medical ErrorsRobMarvinNo ratings yet
- Adverse Drug Reactions Among Children Over A 10-Year Period: ArticleDocument14 pagesAdverse Drug Reactions Among Children Over A 10-Year Period: ArticleJamille GarciaNo ratings yet
- Overconfidence As A Cause of Diagnostic Error in Medicine PDFDocument22 pagesOverconfidence As A Cause of Diagnostic Error in Medicine PDFIulianZaharescuNo ratings yet
- Diagnostic Errors - UpToDateDocument23 pagesDiagnostic Errors - UpToDateJoyce SumagaysayNo ratings yet
- Medication Error Factors, Safety Guideline System, Flow of Drug Usage, and Code of Conduct To Prevent Medication ErrorDocument5 pagesMedication Error Factors, Safety Guideline System, Flow of Drug Usage, and Code of Conduct To Prevent Medication ErrorskyNo ratings yet
- Jurnal Medical SafetyDocument14 pagesJurnal Medical SafetyMARWAH MARWAHNo ratings yet
- 210 1437 1 PB LibreDocument62 pages210 1437 1 PB Librezozorina21No ratings yet
- Medication Error Research PaperDocument5 pagesMedication Error Research Paperafeaoebid100% (3)
- Pharm Paper FinalDocument8 pagesPharm Paper FinalAnamta AkhtarNo ratings yet
- Zhan 2005, ADR Consultas AmbulatoriasDocument7 pagesZhan 2005, ADR Consultas AmbulatoriasCarlos Fernando Montes MondragónNo ratings yet
- OverconfidenceDocument22 pagesOverconfidencejjffmmllNo ratings yet
- Increasing Adverse Drug Reaction Reporting-How Can We Do BetterDocument15 pagesIncreasing Adverse Drug Reaction Reporting-How Can We Do Betterstacie010429No ratings yet
- Safe Pediatric AnesthesiaDocument24 pagesSafe Pediatric AnesthesiamdNo ratings yet
- 2000, Antonow J. Medication Error Reporting PediatriaDocument7 pages2000, Antonow J. Medication Error Reporting PediatriaFilipa Salvador SalvadorNo ratings yet
- Li Et Al-2007-Academic Emergency Medicine PDFDocument3 pagesLi Et Al-2007-Academic Emergency Medicine PDFMariaLisseth MoralesNo ratings yet
- 344 FullDocument6 pages344 FullIndah SundariNo ratings yet
- Almutary, Hayfa Lewis, Peter: C WilkinsDocument19 pagesAlmutary, Hayfa Lewis, Peter: C Wilkinsمالك مناصرةNo ratings yet
- Faktor Informasi ManajemenDocument26 pagesFaktor Informasi ManajemenRAHMA JUMILANo ratings yet
- 01 Risk in Pediatric AnesthesiaDocument11 pages01 Risk in Pediatric AnesthesiaOmar Sanchez PazNo ratings yet
- Clinical Practice Guideline Safe Medication Use.32Document39 pagesClinical Practice Guideline Safe Medication Use.32Edward ZiyachechaNo ratings yet
- Original Contributions: Ten Best Practices For Improving Emergency Medicine Provider-Nurse CommunicationDocument13 pagesOriginal Contributions: Ten Best Practices For Improving Emergency Medicine Provider-Nurse CommunicationRodrigoSachiFreitasNo ratings yet
- 1 s2.0 S2049080121000595 Main1Document6 pages1 s2.0 S2049080121000595 Main1Devina ArrandhikasariNo ratings yet
- Patient Reported BarriesDocument14 pagesPatient Reported Barriesdani catriaNo ratings yet
- The Percentage of Medication Errors Globally, and in Saudi ArabiaDocument7 pagesThe Percentage of Medication Errors Globally, and in Saudi ArabiaLeen alghamdNo ratings yet
- Life-Threatening Drug Interactions: What The Physician Needs To KnowDocument12 pagesLife-Threatening Drug Interactions: What The Physician Needs To Knowjuan daniel ayakaNo ratings yet
- HHS Public Access: US Emergency Department Visits For Outpatient Adverse Drug Events, 2013-2014Document26 pagesHHS Public Access: US Emergency Department Visits For Outpatient Adverse Drug Events, 2013-2014rosianaNo ratings yet
- EBP Deliverable Module 2Document6 pagesEBP Deliverable Module 2Marian SmithNo ratings yet
- Risk in Pediatric Anesthesia PDFDocument10 pagesRisk in Pediatric Anesthesia PDFWisnu PratamaNo ratings yet
- Nurse Perceptions of Medication ErrorsDocument9 pagesNurse Perceptions of Medication ErrorsMoisés PonceNo ratings yet
- Chapter 12 - Patient Safety - APIC Text OnlineDocument30 pagesChapter 12 - Patient Safety - APIC Text OnlineManalAbdelazizNo ratings yet
- Computerized ProgramDocument7 pagesComputerized ProgramfatiisaadatNo ratings yet
- Management of Obstetric Postpartum Hemorrhage A National Service Evaluation of Current Practice in The UKDocument7 pagesManagement of Obstetric Postpartum Hemorrhage A National Service Evaluation of Current Practice in The UKinggritdrdwirizkyNo ratings yet
- 2018 - Baraki Et AlDocument8 pages2018 - Baraki Et AlazeemathmariyamNo ratings yet
- Ijic PDFDocument7 pagesIjic PDFitalatif1No ratings yet
- Sessionsetal High Alert Meds 919 JANDocument15 pagesSessionsetal High Alert Meds 919 JANichabojanNo ratings yet
- The Effect of Emergency Department Crowding On Patient Outcomes: A Literature ReviewDocument4 pagesThe Effect of Emergency Department Crowding On Patient Outcomes: A Literature ReviewRohon EzekielNo ratings yet
- Nej Mo A 1306801Document11 pagesNej Mo A 1306801Anonymous 8w9QEGNo ratings yet
- PSJ - Volume 8 - Issue 1 - Pages 13-23Document11 pagesPSJ - Volume 8 - Issue 1 - Pages 13-23mauliana mardhira fauzaNo ratings yet
- Preventive Medicine Reports: Samuel R. Bunting, Brian A. Feinstein, Aniruddha Hazra, Neeral K. Sheth, Sarah S. GarberDocument9 pagesPreventive Medicine Reports: Samuel R. Bunting, Brian A. Feinstein, Aniruddha Hazra, Neeral K. Sheth, Sarah S. GarberKnowledge PepalaNo ratings yet
- Man 238Document10 pagesMan 238Ujjwal MaharjanNo ratings yet
- TH 16024Document10 pagesTH 16024dnoksNo ratings yet
- Errores de Administración de Medicamentos 2021Document8 pagesErrores de Administración de Medicamentos 2021Jose Juan CoronaNo ratings yet
- WilliamsDocument4 pagesWilliamsRajesh KumarNo ratings yet
- Medication Errors:: Don't Let Them Happen To YouDocument6 pagesMedication Errors:: Don't Let Them Happen To YouPhuong Tran100% (1)
- Homework Tang KimHuyDocument2 pagesHomework Tang KimHuyseng songhaNo ratings yet
- Keys To The Spirit World (Empath U)Document53 pagesKeys To The Spirit World (Empath U)Ruthy Balot100% (1)
- Ge Msds Kleen Mct511 LDocument7 pagesGe Msds Kleen Mct511 LJean RisquezNo ratings yet
- Acutrak2 Radial Head Case StudyDocument2 pagesAcutrak2 Radial Head Case StudyDinesh KumarNo ratings yet
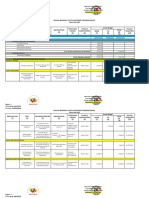
- ABYIP-2023 TemplateDocument3 pagesABYIP-2023 Templatejomar88% (26)
- My Asthma Action Plan: Recognising Symptoms and Taking ActionDocument2 pagesMy Asthma Action Plan: Recognising Symptoms and Taking ActionMallika EssamsettyNo ratings yet
- Benefits of Nordic WalkingDocument7 pagesBenefits of Nordic WalkingHuy ĐạtNo ratings yet
- Medical Clearance Letter TemplateDocument3 pagesMedical Clearance Letter TemplateSebastián CoronadoNo ratings yet
- Abnoramal ECGDocument20 pagesAbnoramal ECGImmanuelNo ratings yet
- Coe, & Vandegrift. 2015 (Youth Politics and Culture in Contemporary LA A Review)Document23 pagesCoe, & Vandegrift. 2015 (Youth Politics and Culture in Contemporary LA A Review)Alejandro MolinaNo ratings yet
- PTSD Economic CulturalDocument19 pagesPTSD Economic CulturalJason SnapeNo ratings yet
- Introduction To Consumer Behaviour: Oxford University Press Sample ChapterDocument51 pagesIntroduction To Consumer Behaviour: Oxford University Press Sample ChapterMuhammad Imran AwanNo ratings yet
- Job Hazard Analysis Safety ControlsDocument18 pagesJob Hazard Analysis Safety ControlsBNCH100% (3)
- 2014 Ion Exchange Cartridge Units RC 6500 PDFDocument2 pages2014 Ion Exchange Cartridge Units RC 6500 PDFKhang TrầnNo ratings yet
- Nutritious Philippine Herbs Combat MalnutritionDocument5 pagesNutritious Philippine Herbs Combat MalnutritionPeter Pantazia0% (1)
- Forced Abortions ExposedDocument26 pagesForced Abortions Exposedesorenson1No ratings yet
- Varda Muhlbauer, Joan C. Chrisler, Florence L. Denmark Eds. Women and Aging An International, Intersectional Power PerspectiveDocument182 pagesVarda Muhlbauer, Joan C. Chrisler, Florence L. Denmark Eds. Women and Aging An International, Intersectional Power PerspectivePaz TroncosoNo ratings yet
- MalariaDocument83 pagesMalariasarguss1467% (3)
- Oum Business School: Matriculation No: Identity Card No.: Telephone No.: E-Mail: Learning CentreDocument6 pagesOum Business School: Matriculation No: Identity Card No.: Telephone No.: E-Mail: Learning CentreInspire28No ratings yet
- Position PaperDocument2 pagesPosition Paperapi-340817333No ratings yet
- Sanskrit EssaysDocument4 pagesSanskrit Essaysafibzfwdkaesyf100% (2)
- RAPID Resources for Lowering Fertility and Achieving Sustainable Development in the PhilippinesDocument41 pagesRAPID Resources for Lowering Fertility and Achieving Sustainable Development in the PhilippinesLeyrra Paclibar DiduloNo ratings yet
- In (Ampinex, Clovilin, Vatacil)Document2 pagesIn (Ampinex, Clovilin, Vatacil)karenmichellelecarozNo ratings yet
- DFGHDocument6 pagesDFGHManuelEduardoSanchezSotoNo ratings yet
- What Is Moxibustion Acupuncturedrcmt PDFDocument3 pagesWhat Is Moxibustion Acupuncturedrcmt PDFStillingKruse2No ratings yet
- WIC Authorized Food List: Shopping GuideDocument17 pagesWIC Authorized Food List: Shopping GuideGanda PrajaNo ratings yet
- And Netflix Show, Ask The Storybots, Now Star in Their Own Board Books!Document2 pagesAnd Netflix Show, Ask The Storybots, Now Star in Their Own Board Books!kagnejukkeNo ratings yet
- Emotional ResilienceDocument3 pagesEmotional ResilienceGODEANU FLORIN100% (1)
- MCQsDocument10 pagesMCQsraguchandra7527100% (1)
- National Polio Lab ChecklistDocument12 pagesNational Polio Lab ChecklistSelaina NawadraNo ratings yet
- Save Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryFrom EverandSave Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryNo ratings yet
- Allen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductFrom EverandAllen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductRating: 5 out of 5 stars5/5 (31)
- Healing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildFrom EverandHealing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildRating: 3.5 out of 5 stars3.5/5 (9)
- The Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsFrom EverandThe Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsNo ratings yet
- Alcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousFrom EverandAlcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousRating: 5 out of 5 stars5/5 (22)
- Sober Curious: The Blissful Sleep, Greater Focus, Limitless Presence, and Deep Connection Awaiting Us All on the Other Side of AlcoholFrom EverandSober Curious: The Blissful Sleep, Greater Focus, Limitless Presence, and Deep Connection Awaiting Us All on the Other Side of AlcoholRating: 4.5 out of 5 stars4.5/5 (127)
- Stop Drinking Now: The original Easyway methodFrom EverandStop Drinking Now: The original Easyway methodRating: 5 out of 5 stars5/5 (28)
- Breaking Addiction: A 7-Step Handbook for Ending Any AddictionFrom EverandBreaking Addiction: A 7-Step Handbook for Ending Any AddictionRating: 4.5 out of 5 stars4.5/5 (2)
- Stop Smoking with Allen Carr: Includes 70 minute audio epilogue read by AllenFrom EverandStop Smoking with Allen Carr: Includes 70 minute audio epilogue read by AllenRating: 5 out of 5 stars5/5 (61)
- Breathing Under Water: Spirituality and the Twelve StepsFrom EverandBreathing Under Water: Spirituality and the Twelve StepsRating: 4.5 out of 5 stars4.5/5 (41)
- Smart Phone Dumb Phone: Free Yourself from Digital AddictionFrom EverandSmart Phone Dumb Phone: Free Yourself from Digital AddictionRating: 5 out of 5 stars5/5 (11)
- The Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionFrom EverandThe Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionRating: 5 out of 5 stars5/5 (63)
- Allen Carr's Easy Way to Quit Smoking Without Willpower: The best-selling quit smoking method updated for the 21st centuryFrom EverandAllen Carr's Easy Way to Quit Smoking Without Willpower: The best-selling quit smoking method updated for the 21st centuryRating: 5 out of 5 stars5/5 (47)
- Total Dopamine Detox in 7 Easy Steps: Become the Master of Your Brain to Quit Your Phone Addiction, Porn Addiction, or Manage Your ADHDFrom EverandTotal Dopamine Detox in 7 Easy Steps: Become the Master of Your Brain to Quit Your Phone Addiction, Porn Addiction, or Manage Your ADHDRating: 4 out of 5 stars4/5 (8)
- Easyway Express: Stop Smoking and Quit E-CigarettesFrom EverandEasyway Express: Stop Smoking and Quit E-CigarettesRating: 5 out of 5 stars5/5 (15)
- Drop the Rock: Removing Character Defects: Steps Six and Seven (2nd. ed.)From EverandDrop the Rock: Removing Character Defects: Steps Six and Seven (2nd. ed.)Rating: 4.5 out of 5 stars4.5/5 (52)
- The Art of Self-Therapy: How to Grow, Gain Self-Awareness, and Understand Your EmotionsFrom EverandThe Art of Self-Therapy: How to Grow, Gain Self-Awareness, and Understand Your EmotionsRating: 5 out of 5 stars5/5 (1)
- Mommy Doesn't Drink Here Anymore: Getting Through the First Year of SobrietyFrom EverandMommy Doesn't Drink Here Anymore: Getting Through the First Year of SobrietyRating: 4.5 out of 5 stars4.5/5 (17)
- Recovery 2.0: Move Beyond Addiction and Upgrade Your LifeFrom EverandRecovery 2.0: Move Beyond Addiction and Upgrade Your LifeRating: 5 out of 5 stars5/5 (8)
- Allen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerFrom EverandAllen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerRating: 5 out of 5 stars5/5 (8)
- As Bill Sees It: Unique compilation of insightful and inspiring short contributions from A.A. co-founder Bill W.From EverandAs Bill Sees It: Unique compilation of insightful and inspiring short contributions from A.A. co-founder Bill W.Rating: 4.5 out of 5 stars4.5/5 (31)