You might also like
- Endoscopy in Pediatric Inflammatory Bowel DiseaseFrom EverandEndoscopy in Pediatric Inflammatory Bowel DiseaseLuigi Dall'OglioNo ratings yet
- Mangement of Thyroglossal Duct CystDocument3 pagesMangement of Thyroglossal Duct CystmohamedhazemelfollNo ratings yet
- Management of Thyroglossal Duct Cyst PDocument3 pagesManagement of Thyroglossal Duct Cyst Pnugroho2212No ratings yet
- Chist Canal TireoglosDocument7 pagesChist Canal TireoglosAurel OctavianNo ratings yet
- Recurrent Thyroglossal Duct Cysts: A 15-Year Review of Presentation, Management and Outcomes From A Tertiary Paediatric InstitutionDocument6 pagesRecurrent Thyroglossal Duct Cysts: A 15-Year Review of Presentation, Management and Outcomes From A Tertiary Paediatric InstitutionTasia RozakiahNo ratings yet
- Jcem 0458Document8 pagesJcem 0458abigailNo ratings yet
- Simultaneous Papillary Carcinoma in Thyroglossal Duct Cyst and ThyroidDocument5 pagesSimultaneous Papillary Carcinoma in Thyroglossal Duct Cyst and ThyroidOncologiaGonzalezBrenes Gonzalez BrenesNo ratings yet
- Fsurg 07 609852Document5 pagesFsurg 07 609852Nayibe Avila MNo ratings yet
- Thyroglossal Duct Cyst in The Suprasternal RegionDocument3 pagesThyroglossal Duct Cyst in The Suprasternal RegionKhairuman anandaNo ratings yet
- Thyroglossal Duct Cyst Carcinoma WithDocument8 pagesThyroglossal Duct Cyst Carcinoma WithM Ali AdrianNo ratings yet
- Primary Ciliary Dyskinesia: An Update On Clinical Aspects, Genetics, Diagnosis, and Future Treatment StrategiesDocument13 pagesPrimary Ciliary Dyskinesia: An Update On Clinical Aspects, Genetics, Diagnosis, and Future Treatment StrategiesMarceloCorralesNo ratings yet
- Aps 25 14Document6 pagesAps 25 14Mehul JainNo ratings yet
- Thyroglossal Duct Cyst - More Than Just An Embryological RemnantDocument4 pagesThyroglossal Duct Cyst - More Than Just An Embryological RemnantkancutpaulkadotNo ratings yet
- Undescended Testis: Ravibindu RanawakaDocument2 pagesUndescended Testis: Ravibindu RanawakaBrianne LeeNo ratings yet
- A Decade of Management of Subdural Haematoma in Children Aged 2 To 24 Months Hospitalized at The Paediatric Neurosurgery Department of La Timone Children's HospitalDocument8 pagesA Decade of Management of Subdural Haematoma in Children Aged 2 To 24 Months Hospitalized at The Paediatric Neurosurgery Department of La Timone Children's HospitalEditor IJTSRDNo ratings yet
- Rjac 338Document2 pagesRjac 338tarmohamed.muradNo ratings yet
- Achondroplasia Natural History Study (CLARITY)Document7 pagesAchondroplasia Natural History Study (CLARITY)jakelinelagoadvNo ratings yet
- Empiema en NiñosDocument5 pagesEmpiema en NiñosMarbel CreusNo ratings yet
- Ho Et Al 2022 Management of Descending Necrotizing Mediastinitis A Severe Complication of Deep Neck Infection Based OnDocument8 pagesHo Et Al 2022 Management of Descending Necrotizing Mediastinitis A Severe Complication of Deep Neck Infection Based OncharlaayasyafefiNo ratings yet
- Trans Cath Closure PDADocument9 pagesTrans Cath Closure PDAinnefarissaNo ratings yet
- 1 s2.0 S0021755722000055 MainDocument6 pages1 s2.0 S0021755722000055 MainUsee TvNo ratings yet
- Long Term (10 Year) Outcomes and Prognostic FactorDocument8 pagesLong Term (10 Year) Outcomes and Prognostic FactorNICOLÁS DANIEL SANCHEZ HERNANDEZNo ratings yet
- 8 Pseudocyst of Pinna and Its Treatment With Surgical Deroofing - An Experience at Tertiary Hospitals 2013Document13 pages8 Pseudocyst of Pinna and Its Treatment With Surgical Deroofing - An Experience at Tertiary Hospitals 2013solikin ikinNo ratings yet
- Prenatal Ultrasound Parameters in Single Suture CraniosynostosisDocument9 pagesPrenatal Ultrasound Parameters in Single Suture CraniosynostosisLuisNo ratings yet
- EcheverríaSepúlveda2022 Article TheUndescendedTestisInChildrenDocument11 pagesEcheverríaSepúlveda2022 Article TheUndescendedTestisInChildrenMELVIN JOHNNo ratings yet
- Suprasellar and Recurrent Pediatric Craniopharyngiomas: Expanding Indications For The Extended Endoscopic Transsphenoidal ApproachDocument9 pagesSuprasellar and Recurrent Pediatric Craniopharyngiomas: Expanding Indications For The Extended Endoscopic Transsphenoidal Approachbenjamin6macindewar6No ratings yet
- Chen 2017Document6 pagesChen 2017dewa gede eka yuditiraNo ratings yet
- BAaadDocument5 pagesBAaadekalospratamaNo ratings yet
- 319-Article Text-419-1-10-20200520Document5 pages319-Article Text-419-1-10-20200520InnafaradinaNo ratings yet
- Surgical Treatment of Thalamic Tumors in ChildrenDocument11 pagesSurgical Treatment of Thalamic Tumors in ChildrenPavel SebastianNo ratings yet
- 10 5799-Ahinjs 01 2012 04 0203-104197Document4 pages10 5799-Ahinjs 01 2012 04 0203-104197rani kadekNo ratings yet
- Sub MandibleDocument6 pagesSub Mandibledaniel pasaribuNo ratings yet
- A Serious Complicatıon of Liver Hydatid Cysts in Children: Cystobiliary FistulasDocument10 pagesA Serious Complicatıon of Liver Hydatid Cysts in Children: Cystobiliary Fistulasronald cespedesNo ratings yet
- Aydin 2017Document7 pagesAydin 2017Berry BancinNo ratings yet
- 2228 PDFDocument4 pages2228 PDFMohsinAminNo ratings yet
- 2020 Article 2459Document9 pages2020 Article 2459Chong ArthinantNo ratings yet
- Multiple-Suture Nonsyndromic Craniosynostosis: Early and Effective Management Using Endoscopic TechniquesDocument9 pagesMultiple-Suture Nonsyndromic Craniosynostosis: Early and Effective Management Using Endoscopic TechniquesKiky Martha A.No ratings yet
- Neonatal Respiratory System Updates 2020Document824 pagesNeonatal Respiratory System Updates 2020link_wolfloboNo ratings yet
- AsianJNeurosurg8121-7546405 205744Document8 pagesAsianJNeurosurg8121-7546405 205744WildaHanimNo ratings yet
- Subglottic Stenosis SGSDocument7 pagesSubglottic Stenosis SGSJose ManuelNo ratings yet
- Indications For Surgery in Acute Mastoiditis and Their Complications in ChildrenDocument47 pagesIndications For Surgery in Acute Mastoiditis and Their Complications in ChildrenantiNo ratings yet
- When The Limp Has A Dietary Cause - A Retrospective Study On Scurvy in A Tertiary Italian Pediatric HospDocument9 pagesWhen The Limp Has A Dietary Cause - A Retrospective Study On Scurvy in A Tertiary Italian Pediatric HospgistaluvikaNo ratings yet
- Thyroglossal Duct Cyst & Sistrunk: A Case Series: July 2015Document6 pagesThyroglossal Duct Cyst & Sistrunk: A Case Series: July 2015Victor Joel Rios GonzalesNo ratings yet
- Kist Tiro GlosusDocument6 pagesKist Tiro GlosusKhairuman FitrahNo ratings yet
- Abdomen: International Abstracts of Pediatric Surgery 593Document1 pageAbdomen: International Abstracts of Pediatric Surgery 593Yohanes WilliamNo ratings yet
- Factors Affecting The Approaches and Complications of Surgery inDocument8 pagesFactors Affecting The Approaches and Complications of Surgery inAlin VázquezNo ratings yet
- Clinicopathological Study of Thyroglossal Cyst 2j3c1n18asDocument5 pagesClinicopathological Study of Thyroglossal Cyst 2j3c1n18asd202020315No ratings yet
- 10 1097@scs 0000000000003278Document3 pages10 1097@scs 0000000000003278Meva'a RogerNo ratings yet
- Number: 0420: Please See Amendment For Pennsylvania Medicaid at The End of This CPBDocument19 pagesNumber: 0420: Please See Amendment For Pennsylvania Medicaid at The End of This CPBAryanto AntoNo ratings yet
- Journal of Pediatric SurgeryDocument6 pagesJournal of Pediatric SurgeryEkaNo ratings yet
- International Journal of Pediatric OtorhinolaryngologyDocument7 pagesInternational Journal of Pediatric OtorhinolaryngologyAndi SuhriyanaNo ratings yet
- Comparison of Recurrence of Pterygium Following Excision by Bare Sclera Technique With and Without Mitomycin CDocument80 pagesComparison of Recurrence of Pterygium Following Excision by Bare Sclera Technique With and Without Mitomycin CShoaib AbbasNo ratings yet
- Shunting in Tuberculous Meningitis A NeuDocument4 pagesShunting in Tuberculous Meningitis A NeumirmasottNo ratings yet
- Mikropenis Dan UDTDocument4 pagesMikropenis Dan UDTOcy BikeNo ratings yet
- Wu Et Al 2020 Descending Necrotizing Mediastinitis Analysis of 9 Cases in Our HospitalDocument4 pagesWu Et Al 2020 Descending Necrotizing Mediastinitis Analysis of 9 Cases in Our HospitalcharlaayasyafefiNo ratings yet
- 1 SM PDFDocument5 pages1 SM PDFHary RahmanNo ratings yet
- Niu 2019Document7 pagesNiu 2019Dazz MiitNo ratings yet
- Potdar 2020Document8 pagesPotdar 2020Christian Leonardo Molina HinojosaNo ratings yet
- Jurnal AnisaDocument5 pagesJurnal AnisaNisaNo ratings yet
- Role of Bleomycin Sclerotherapy As A Non-Surgical Method For The Treatment of Cystic Hygroma of Head and Neck Region-An Institutional StudyDocument7 pagesRole of Bleomycin Sclerotherapy As A Non-Surgical Method For The Treatment of Cystic Hygroma of Head and Neck Region-An Institutional StudyMinh ChíNo ratings yet
- About Alok Industries: Insolvency FilingDocument4 pagesAbout Alok Industries: Insolvency FilingHarshit GuptaNo ratings yet
- Oracle Optimized Solution For Backup and RecoveryDocument37 pagesOracle Optimized Solution For Backup and Recoverywish_newNo ratings yet
- InstitutionalismDocument15 pagesInstitutionalismLowel DalisayNo ratings yet
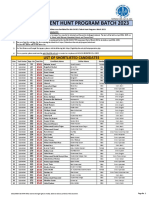
- Iba Ogdcl Talent Hunt Program Batch 2023: List of Shortlisted CandidatesDocument30 pagesIba Ogdcl Talent Hunt Program Batch 2023: List of Shortlisted CandidatesSomil KumarNo ratings yet
- 2017-18 Annual Report - California YMCA Youth & GovernmentDocument16 pages2017-18 Annual Report - California YMCA Youth & GovernmentRichard HsuNo ratings yet
- Security Administration GuideDocument416 pagesSecurity Administration GuideCauã VinhasNo ratings yet
- Vak Dec. '21 PDFDocument28 pagesVak Dec. '21 PDFMuralidharanNo ratings yet
- Sworn Statement - TemarioDocument1 pageSworn Statement - Temariozyphora grace trillanesNo ratings yet
- Financial Analysts - Occupational Outlook Handbook - U.S. Bureau of Labor StatisticsDocument6 pagesFinancial Analysts - Occupational Outlook Handbook - U.S. Bureau of Labor StatisticsHannah Denise BatallangNo ratings yet
- Computer Networks Notes (17CS52) PDFDocument174 pagesComputer Networks Notes (17CS52) PDFKeerthiNo ratings yet
- Frontier Fiesta Association Scholarships: University of Houston Incoming FreshmanDocument1 pageFrontier Fiesta Association Scholarships: University of Houston Incoming Freshmanapi-269999191No ratings yet
- Chordu Piano Chords Ede Lobas Chordsheet Id - JBQiUlO0NDU PDFDocument3 pagesChordu Piano Chords Ede Lobas Chordsheet Id - JBQiUlO0NDU PDFKaren RochaNo ratings yet
- Facts:: Villarosa, Joan Cristine 2015-1635Document3 pagesFacts:: Villarosa, Joan Cristine 2015-1635Tin VillarosaNo ratings yet
- BAM Administration Guide 4.1.1Document940 pagesBAM Administration Guide 4.1.1Santiago Alexander Celín HueraNo ratings yet
- DMDave - Dungeons & Lairs 56 - Zombie Farmhouse - Free VersionDocument13 pagesDMDave - Dungeons & Lairs 56 - Zombie Farmhouse - Free VersionKarstenNo ratings yet
- QIS-ForM I, II, III Manufacturing FormatDocument9 pagesQIS-ForM I, II, III Manufacturing FormatAshish Gupta67% (3)
- Rule 119-127Document10 pagesRule 119-127xychotic100% (1)
- Confidentiality Statement 02Document1 pageConfidentiality Statement 02Herbert KaplanNo ratings yet
- ANSYS Meshing Users GuideDocument520 pagesANSYS Meshing Users GuideJayakrishnan P SNo ratings yet
- ClaimDocument107 pagesClaimSharmi SanthakumarNo ratings yet
- POLITICAL SYSTEM of USADocument23 pagesPOLITICAL SYSTEM of USAMahtab HusaainNo ratings yet
- Laura Lammasniemi - Law Dissertations - A Step-By-Step Guide-Routledge (2018)Document208 pagesLaura Lammasniemi - Law Dissertations - A Step-By-Step Guide-Routledge (2018)Rina DewiNo ratings yet
- Last Two Verse of Surah AlDocument5 pagesLast Two Verse of Surah AlMhonly MamangcaoNo ratings yet
- Candlestick Charting: Quick Reference GuideDocument24 pagesCandlestick Charting: Quick Reference GuideelisaNo ratings yet
- In This Chapter : Me, ShankarDocument20 pagesIn This Chapter : Me, ShankarPied AvocetNo ratings yet
- Full Download Test Bank For Cognitive Psychology 6th Edition Sternberg PDF Full ChapterDocument31 pagesFull Download Test Bank For Cognitive Psychology 6th Edition Sternberg PDF Full Chaptercadie.tutressrwwsn100% (15)
- United States v. Salvatore Salamone, 902 F.2d 237, 3rd Cir. (1990)Document6 pagesUnited States v. Salvatore Salamone, 902 F.2d 237, 3rd Cir. (1990)Scribd Government DocsNo ratings yet
- Atok-Big Wedge Assn. v. Atok-Big Wedge Co.,97 Phil, 294 '1995Document6 pagesAtok-Big Wedge Assn. v. Atok-Big Wedge Co.,97 Phil, 294 '1995Daniela Sandra AgootNo ratings yet
- Florentino V SupervalueDocument2 pagesFlorentino V SupervalueVener Angelo MargalloNo ratings yet
- PCA Case No. 2013-19Document43 pagesPCA Case No. 2013-19Joyen JimenezNo ratings yet