You might also like
- Detox and Heal Your SelfDocument48 pagesDetox and Heal Your SelfKajsaNo ratings yet
- Nclex RN Test - Free Nclex RN Test HelpDocument7 pagesNclex RN Test - Free Nclex RN Test Helppasstest1234No ratings yet
- Jaundice NotesDocument8 pagesJaundice NotesDanielle Jann Manio ConcepcionNo ratings yet
- Doctor Profile Format Dr. Sarika Trimbak Shinde, MSDocument3 pagesDoctor Profile Format Dr. Sarika Trimbak Shinde, MSSwapnil JaikarNo ratings yet
- Liver Function Lecture NotesDocument9 pagesLiver Function Lecture NotesMarie Bernadette DigoNo ratings yet
- Lecture Notes: Clinical Chemistry of LiverDocument38 pagesLecture Notes: Clinical Chemistry of LivershehnilaNo ratings yet
- Risk Assessment Water Tank Cleaning 2023Document3 pagesRisk Assessment Water Tank Cleaning 2023Karan SuleNo ratings yet
- Hyperbilirubinemia: West Visayas State University College of Medicine Neonatal Intensive Care UnitDocument49 pagesHyperbilirubinemia: West Visayas State University College of Medicine Neonatal Intensive Care UnitDonna LabaniegoNo ratings yet
- ResumeDocument2 pagesResumeapi-283008119No ratings yet
- Concepts of Jaundice by DR SarmaDocument53 pagesConcepts of Jaundice by DR SarmaAmanuel Maru100% (3)
- Biochemical Functions of The LiverDocument25 pagesBiochemical Functions of The LiverSaifNo ratings yet
- Post Mature Neonate, Infant of Diabetic and Substance Abuse MotherDocument14 pagesPost Mature Neonate, Infant of Diabetic and Substance Abuse MotherShilpa JoshiNo ratings yet
- BIOCHEM Jaundice FinalDocument54 pagesBIOCHEM Jaundice FinalJohnRobynDiezNo ratings yet
- Neonatal Jaundice CmeDocument39 pagesNeonatal Jaundice CmeGideon K. Mutai100% (1)
- Basic Nursing PharmacologyDocument78 pagesBasic Nursing PharmacologyLloyd Rafael EstabilloNo ratings yet
- Hypertensive UrgencyDocument8 pagesHypertensive UrgencyTony A.No ratings yet
- HB Degradation: D.Hythem SaeedDocument34 pagesHB Degradation: D.Hythem Saeedsamar yousif mohamed100% (1)
- A-Plus HospitalIncome and HospitalIncome Extra Brochure 201306 v2Document8 pagesA-Plus HospitalIncome and HospitalIncome Extra Brochure 201306 v2nusthe2745No ratings yet
- Heme Degradation & HyperbilirubinemiasDocument27 pagesHeme Degradation & HyperbilirubinemiasIMDCBiochemNo ratings yet
- The Liver and Its DisordersDocument41 pagesThe Liver and Its Disordersreuben kwotaNo ratings yet
- Transcutaneous Bilirubin DNB PDF 2023Document46 pagesTranscutaneous Bilirubin DNB PDF 2023Rishabh MasutaNo ratings yet
- Liver FunctionDocument45 pagesLiver Functionpuno ric100% (1)
- IJRPR7994Document6 pagesIJRPR7994rifa iNo ratings yet
- Jaundice (Icterus) 2015: DR A.A.MokhtarDocument49 pagesJaundice (Icterus) 2015: DR A.A.MokhtarAbdelrahman MokhtarNo ratings yet
- Bilirubin Metabolism and HyperbilirubinaemiasDocument35 pagesBilirubin Metabolism and HyperbilirubinaemiasEuphrasiaNo ratings yet
- Concepts of Jaundice by DR SarmaDocument53 pagesConcepts of Jaundice by DR SarmamainztreamNo ratings yet
- Metabolism of Bilirubin and Bile Salt SynthesisDocument34 pagesMetabolism of Bilirubin and Bile Salt SynthesisKumail LakraNo ratings yet
- Final Jaundice1Document43 pagesFinal Jaundice1ahmad solehinNo ratings yet
- Jaundice FinalDocument30 pagesJaundice FinalFrances GrefalNo ratings yet
- Liver Function Mazen 1Document24 pagesLiver Function Mazen 1Ahmed GaberNo ratings yet
- 212 Spring 2005 Heme DegradationDocument17 pages212 Spring 2005 Heme Degradationcockatoo_whiteNo ratings yet
- 57-Overview of Approach To HyperbilirubinemiaDocument21 pages57-Overview of Approach To Hyperbilirubinemiakushraj khandelwalNo ratings yet
- CLINICAL CHEMISTRY OF LIVER (New)Document18 pagesCLINICAL CHEMISTRY OF LIVER (New)haidernadhem57No ratings yet
- Clase 3 HepatogramaDocument9 pagesClase 3 HepatogramajuanpbagurNo ratings yet
- Jaundice Classification and DiagnosisDocument46 pagesJaundice Classification and DiagnosisKhadijaNo ratings yet
- Neonatal JaundiceDocument54 pagesNeonatal JaundiceTheresa MendoncaNo ratings yet
- Jaundice: DR: Ramy A. SamyDocument42 pagesJaundice: DR: Ramy A. Samyoscar3spurgeonNo ratings yet
- J Mpsur 2017 09 012Document7 pagesJ Mpsur 2017 09 012riffarsyad100% (1)
- Neonatal JaundiceDocument95 pagesNeonatal JaundiceChidi MbatuegwuNo ratings yet
- Chapter - 3-Clinical ChemistryDocument43 pagesChapter - 3-Clinical Chemistryyasin oumerNo ratings yet
- 06 Bilirubin Metabolism016Document28 pages06 Bilirubin Metabolism016Arif NabeelNo ratings yet
- Clinical Approach To Jaundice (GSH)Document19 pagesClinical Approach To Jaundice (GSH)handikaNo ratings yet
- Heme Degradation & HyperbilirubinemiasDocument30 pagesHeme Degradation & HyperbilirubinemiasSubhi MishraNo ratings yet
- 16-01 - Jaundice & Amp Evaluation of Abnormal Liver Biochemical TestsDocument16 pages16-01 - Jaundice & Amp Evaluation of Abnormal Liver Biochemical TestsSergio VasquezNo ratings yet
- 19.neonatal JaundiceDocument42 pages19.neonatal JaundiceWilhellmuss MaukaNo ratings yet
- Evaluation of Abnormal Liver Function Tests: ReviewDocument7 pagesEvaluation of Abnormal Liver Function Tests: ReviewfedlyNo ratings yet
- Pathophysiology of Laboratory Abnormalities in Liver DisordersDocument55 pagesPathophysiology of Laboratory Abnormalities in Liver DisordersYudha fedrian AKNo ratings yet
- Liver Function Test (TSB)Document25 pagesLiver Function Test (TSB)shafyd ramdanNo ratings yet
- M. JaundiceDocument9 pagesM. JaundiceRoselle Joy D. RosalejosNo ratings yet
- IMS: Jaundice: ME218 & ME119Document84 pagesIMS: Jaundice: ME218 & ME119huda zainalNo ratings yet
- Research ProposalDocument5 pagesResearch ProposalZablon KodilaNo ratings yet
- Obstructive Jaundice BMJlearningmoduleDocument26 pagesObstructive Jaundice BMJlearningmodulesamudraandiNo ratings yet
- Isolated Elevated BilirubinDocument4 pagesIsolated Elevated BilirubinRajabu KhalidNo ratings yet
- L6 - Bilirubin MetabolismDocument28 pagesL6 - Bilirubin Metabolismyouservezeropurpose113No ratings yet
- Bilirubin Metabolism Applied Physiology PDFDocument6 pagesBilirubin Metabolism Applied Physiology PDFRenata SetyariantikaNo ratings yet
- 5 - JaundiceDocument16 pages5 - JaundiceHamzehNo ratings yet
- Concepts of Jaundice by DR SarmaDocument53 pagesConcepts of Jaundice by DR Sarmacrazymo299No ratings yet
- Astu by Assefa Weldu & Atnikut Mengesh Moderated by DR .Document23 pagesAstu by Assefa Weldu & Atnikut Mengesh Moderated by DR .Meseret Hamer ZewdieNo ratings yet
- Physiology and Pathology BILIRUBIN SINTESISDocument9 pagesPhysiology and Pathology BILIRUBIN SINTESISIda Bagus SaktianaNo ratings yet
- Clinical Chemistry of Liver-4th Level-3!12!2012Document39 pagesClinical Chemistry of Liver-4th Level-3!12!2012Sena YadesaNo ratings yet
- Neonatal Jaundice: Zilpa, AMODocument44 pagesNeonatal Jaundice: Zilpa, AMOmarco luenaNo ratings yet
- 23.12.2022 - Metabolism of Heme and BilirubinDocument4 pages23.12.2022 - Metabolism of Heme and BilirubinMuhammed GaribovNo ratings yet
- Differential Diagnosis of JaundiceDocument4 pagesDifferential Diagnosis of JaundiceVirag PatilNo ratings yet
- Jaundice - StatPearls - NCBI BookshelfDocument11 pagesJaundice - StatPearls - NCBI BookshelfCONSTANTIUS AUGUSTONo ratings yet
- Hereditary Jaundice Cap125Document90 pagesHereditary Jaundice Cap125BarDFNo ratings yet
- Liver Chemistry and Function Tests: Daniel S. PrattDocument11 pagesLiver Chemistry and Function Tests: Daniel S. PrattAnişoara FrunzeNo ratings yet
- Physiology for General Surgical Sciences Examination (GSSE)From EverandPhysiology for General Surgical Sciences Examination (GSSE)S. Ali MirjaliliNo ratings yet
- International Textbook of Diabetes MellitusFrom EverandInternational Textbook of Diabetes MellitusR. A. DeFronzoNo ratings yet
- Review Article Intrathecal Drug Spread: G. Hocking and J. A. W. WildsmithDocument11 pagesReview Article Intrathecal Drug Spread: G. Hocking and J. A. W. WildsmithHalim SudonoNo ratings yet
- ImmunogeneticsDocument26 pagesImmunogeneticsOanaDorofteNo ratings yet
- Evidence Base Practice: Submitted To: Maam Fizza, 3868Document6 pagesEvidence Base Practice: Submitted To: Maam Fizza, 3868Ambreen TariqNo ratings yet
- Price ListDocument119 pagesPrice ListDanielNo ratings yet
- Practical Worksheet Animal StructureDocument11 pagesPractical Worksheet Animal StructureGHOFARI SABIUL HAQ TAUFIQURRAHMAN 1No ratings yet
- Hilton Et Al, 1997 (Ab To BSA) PDFDocument10 pagesHilton Et Al, 1997 (Ab To BSA) PDFFarkhanda SadafNo ratings yet
- Tait Acute and Critical Care in Adult Nursing 3e Chapter 1Document36 pagesTait Acute and Critical Care in Adult Nursing 3e Chapter 1robinmilton1998No ratings yet
- Micro Lab 11Document3 pagesMicro Lab 11goatsecksNo ratings yet
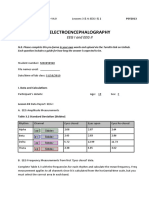
- L03 - 04 EEG MondayDocument10 pagesL03 - 04 EEG MondayShawn SequeiraNo ratings yet
- Pathology Quality ManualDocument40 pagesPathology Quality ManualInn MironNo ratings yet
- Hyperbaric Oxygen Therapy (Hbot) : Presented by DR Manu Bhaskaran NairDocument55 pagesHyperbaric Oxygen Therapy (Hbot) : Presented by DR Manu Bhaskaran NairMahipal Reddy NimmalaNo ratings yet
- Post-ACLS Megacode Flashcards - QuizletDocument9 pagesPost-ACLS Megacode Flashcards - QuizletMaya LaPradeNo ratings yet
- Conectys Clinic ProceduresDocument13 pagesConectys Clinic Proceduresjmmos207064No ratings yet
- Muscle & Nerve Volume 31 Issue 5 2005 (Doi 10 - CopiarDocument5 pagesMuscle & Nerve Volume 31 Issue 5 2005 (Doi 10 - CopiarMatthew PhillipsNo ratings yet
- 1976 - Johansson, Berglund, Kjellman - Comparison of IgE Values As Determined by Different Solid Phase Radioimmunoassay MethodsDocument9 pages1976 - Johansson, Berglund, Kjellman - Comparison of IgE Values As Determined by Different Solid Phase Radioimmunoassay Methodspond_1993No ratings yet
- 1 - FMGE Dec GH VersionDocument14 pages1 - FMGE Dec GH VersionHarshit SharmaNo ratings yet
- Fictional Character With DisorderDocument7 pagesFictional Character With DisordermugdhaNo ratings yet
- Tumor Traktus UrogenitalDocument23 pagesTumor Traktus UrogenitalganmarifNo ratings yet
- Great Medical Doctor CV ExampleDocument1 pageGreat Medical Doctor CV ExampleEkvan DanangNo ratings yet
- Postoperative Complications PDFDocument21 pagesPostoperative Complications PDFDoctor's BettaNo ratings yet
- The Four Stages of LaborDocument12 pagesThe Four Stages of LaborEdrea Aquino MendezNo ratings yet