You might also like
- Quality Improvement in Health CareDocument7 pagesQuality Improvement in Health CareFarihaNo ratings yet
- 50 Studies Every Anesthesiologist Shoud Know 2019Document305 pages50 Studies Every Anesthesiologist Shoud Know 2019pcut100% (2)
- Core Concepts in Clinical Infectious Diseases (CCCID)From EverandCore Concepts in Clinical Infectious Diseases (CCCID)Rating: 5 out of 5 stars5/5 (2)
- Sepsis - Definitions - Pathophysiology - and Challenge of Bedside MGMTDocument271 pagesSepsis - Definitions - Pathophysiology - and Challenge of Bedside MGMTJacob Dougherty100% (1)
- Chang Sepsis and Septic ShockDocument19 pagesChang Sepsis and Septic ShockPediatria UDec 2020No ratings yet
- The Unique Characteristics of COVID-19 Coagulopathy: Review Open AccessDocument8 pagesThe Unique Characteristics of COVID-19 Coagulopathy: Review Open AccessRobert MargineanNo ratings yet
- s-0039-1694995Document7 pagess-0039-1694995Cristhian ZamoraNo ratings yet
- Coagulopatia y Sepsis EngDocument10 pagesCoagulopatia y Sepsis Engadrian mendoza croesNo ratings yet
- Source Control in Emergency General SurgeryDocument21 pagesSource Control in Emergency General SurgerylaviniaNo ratings yet
- 7 CID POR SEPSI Iba2020Document7 pages7 CID POR SEPSI Iba2020anaNo ratings yet
- The Role of Endotoxin in Septic Shock: Perspective Open AccessDocument7 pagesThe Role of Endotoxin in Septic Shock: Perspective Open AccessYaxkin NikNo ratings yet
- Rationale For Sequential Extracorporeal Therapy (SET) in SepsisDocument15 pagesRationale For Sequential Extracorporeal Therapy (SET) in SepsisIsrael Villalba FonsecaNo ratings yet
- jcm-10-00877 InvestigaçãoDocument33 pagesjcm-10-00877 InvestigaçãoLucas Monteiro LopesNo ratings yet
- Disseminated Intravascular Coagulopathy DICDocument24 pagesDisseminated Intravascular Coagulopathy DICMassimiliano MalerbaNo ratings yet
- Thromboembolic Disease in COVID-19 Patients: A Brief Narrative ReviewDocument10 pagesThromboembolic Disease in COVID-19 Patients: A Brief Narrative ReviewSteven PutraNo ratings yet
- Targeting Inflammation For The Treatment of Diabetic Kidney Disease: A Five-Compartment Mechanistic ModelDocument17 pagesTargeting Inflammation For The Treatment of Diabetic Kidney Disease: A Five-Compartment Mechanistic ModelIrvin MarcelNo ratings yet
- Anticoagulant Therapy Timing in SepsisDocument7 pagesAnticoagulant Therapy Timing in SepsisRashellya RasyidaNo ratings yet
- Caldas Et Al. (2021)Document13 pagesCaldas Et Al. (2021)Kesley PabloNo ratings yet
- Disfunção Organica PDFDocument6 pagesDisfunção Organica PDFribasguilhermino5366No ratings yet
- A Novel Treatment Approach To The Novel Coronavirus: An Argument For The Use of Therapeutic Plasma Exchange For Fulminant COVID-19Document3 pagesA Novel Treatment Approach To The Novel Coronavirus: An Argument For The Use of Therapeutic Plasma Exchange For Fulminant COVID-19Kristina ZumbanaNo ratings yet
- The Role of SOCS Proteins in The Development of Virus-Induced Hepatocellular CarcinomaDocument10 pagesThe Role of SOCS Proteins in The Development of Virus-Induced Hepatocellular CarcinomaFawzi RahmanNo ratings yet
- Sepsis Associated EncephalopathyDocument12 pagesSepsis Associated EncephalopathyAsim RanaNo ratings yet
- Diagnosis of Sepsis-Induced Disseminated Intravascularcoagulation and CoagulopathyDocument10 pagesDiagnosis of Sepsis-Induced Disseminated Intravascularcoagulation and CoagulopathyDwika AudiyanandaNo ratings yet
- Diagnosis of Sepsis Induced DicDocument10 pagesDiagnosis of Sepsis Induced DicDwika AudiyanandaNo ratings yet
- A Longitudinal Change of Syndecan-1 Predicts Risk of Acute Respiratory Distress Syndrome and Cumulative Fluid Balance in Patients With Septic Shock - A Preliminary StudyDocument9 pagesA Longitudinal Change of Syndecan-1 Predicts Risk of Acute Respiratory Distress Syndrome and Cumulative Fluid Balance in Patients With Septic Shock - A Preliminary StudyPIR BanjarmasinNo ratings yet
- Fisiopatologia Sepsis 2021 Parte 1 PDFDocument9 pagesFisiopatologia Sepsis 2021 Parte 1 PDFrubramNo ratings yet
- s13017 020 00343 yDocument10 pagess13017 020 00343 yPintakasari WNo ratings yet
- antibiotics-13-00046 (1)Document38 pagesantibiotics-13-00046 (1)FatiaNo ratings yet
- Effect of Intravenous Clarithromycin in Patients With Sepsis, Respiratory and Multiple Organ Dysfunction Syndrome: A Randomized Clinical TrialDocument11 pagesEffect of Intravenous Clarithromycin in Patients With Sepsis, Respiratory and Multiple Organ Dysfunction Syndrome: A Randomized Clinical TrialwiwiNo ratings yet
- Multiple Organ Dysfunction Syndrome in Sepsis: 16 Mei 2016 BackgroundDocument6 pagesMultiple Organ Dysfunction Syndrome in Sepsis: 16 Mei 2016 BackgroundrahayuNo ratings yet
- Extending The Host Response' Paradigm From Sepsis To Cardiogenic Shock: Evidence, Limitations and OpportunitiesDocument14 pagesExtending The Host Response' Paradigm From Sepsis To Cardiogenic Shock: Evidence, Limitations and OpportunitiesHelder LezamaNo ratings yet
- Bioengineering 11 00256Document13 pagesBioengineering 11 00256jamel-shamsNo ratings yet
- Trombocitopenia Trombotica Por VacunasDocument9 pagesTrombocitopenia Trombotica Por VacunasGerardo de Gyves AvilaNo ratings yet
- Targeting Hypoxia in The Tumor Microenvironment ADocument16 pagesTargeting Hypoxia in The Tumor Microenvironment AViviana OrellanaNo ratings yet
- Update On Disseminated Intravascular Coagulation: When To Consider It, When To Expect It, When To Treat ItDocument9 pagesUpdate On Disseminated Intravascular Coagulation: When To Consider It, When To Expect It, When To Treat ItYulia RahmawatiNo ratings yet
- Biomarkers in Sepsis A Current Review of New TechnologiesDocument7 pagesBiomarkers in Sepsis A Current Review of New Technologiesrleon746No ratings yet
- Vascular leak in sepsisDocument15 pagesVascular leak in sepsisAli JENDOUBINo ratings yet
- jacobi2002Document6 pagesjacobi2002Oswaldo MascareñasNo ratings yet
- The Management of Intra Abdominal Infections From A Global Perspective 2017 WSES Guidelines For Management of Intra Abdominal InfectionsDocument34 pagesThe Management of Intra Abdominal Infections From A Global Perspective 2017 WSES Guidelines For Management of Intra Abdominal InfectionsJuan CastroNo ratings yet
- DefinitionofdicDocument9 pagesDefinitionofdicDwika AudiyanandaNo ratings yet
- s13054 020 03273 yDocument13 pagess13054 020 03273 yAndi Tiara S. AdamNo ratings yet
- Cytokine Septic ShockDocument13 pagesCytokine Septic ShockEduardo ChanonaNo ratings yet
- Articulo Cientifico de MeningitisDocument14 pagesArticulo Cientifico de Meningitis11-MH-HU-JACKELINE DELIA ESPINOZA MONTERONo ratings yet
- 2021-The Roles of Platelets in COVID-19-associated Coagulopathy and Vaccine-Induced Immune Thrombotic ThrombocytopeniaDocument9 pages2021-The Roles of Platelets in COVID-19-associated Coagulopathy and Vaccine-Induced Immune Thrombotic Thrombocytopeniaseguridadyambiente641No ratings yet
- Disseminated Intravascular Coagulation and Implications For Medical-Surgical NursesDocument5 pagesDisseminated Intravascular Coagulation and Implications For Medical-Surgical Nursesancours100% (1)
- International Wound Journal - 2016 - Li - Vascular Assessment of Wound Healing A Clinical ReviewDocument10 pagesInternational Wound Journal - 2016 - Li - Vascular Assessment of Wound Healing A Clinical Reviewapi-654112138No ratings yet
- 12Document11 pages12monica mahechaNo ratings yet
- Coagulop CovidDocument11 pagesCoagulop CovidbacchiocchipaoloNo ratings yet
- MODS in Sepsis: Organ Dysfunction and PathophysiologyDocument27 pagesMODS in Sepsis: Organ Dysfunction and Pathophysiologyترياق الأملNo ratings yet
- Coagulation Abnormalities in SepsisDocument7 pagesCoagulation Abnormalities in SepsisFajar YuniftiadiNo ratings yet
- Wa0005.Document10 pagesWa0005.Edward ElBuenoNo ratings yet
- Las Trampas Extracelulares de Neutrófilos Inducidas Por El Microambiente Hipóxico en El Cáncer Gástrico Aumentan El Crecimiento TumoralDocument17 pagesLas Trampas Extracelulares de Neutrófilos Inducidas Por El Microambiente Hipóxico en El Cáncer Gástrico Aumentan El Crecimiento TumoralCristhian RodriguezNo ratings yet
- The Main Regularities of The Formation of The Syndrome of Systemic Inflammatory Reaction in Acetic Acid PoisoningDocument4 pagesThe Main Regularities of The Formation of The Syndrome of Systemic Inflammatory Reaction in Acetic Acid PoisoningCentral Asian StudiesNo ratings yet
- COVID-19 Infection: An Overview On Cytokine Storm and Related InterventionsDocument15 pagesCOVID-19 Infection: An Overview On Cytokine Storm and Related InterventionsArlinda Silva PrameswariNo ratings yet
- Messina Et Al-2022-Intensive Care Medicine ExperimentalDocument15 pagesMessina Et Al-2022-Intensive Care Medicine ExperimentalAna Belén Viteri luzuriagaNo ratings yet
- An Update On Targeted Therapies in Systemic SclerosisDocument14 pagesAn Update On Targeted Therapies in Systemic SclerosisJosé Javier Morales NúñezNo ratings yet
- How I Treat Disseminated Intravascular Coagulation 2017Document23 pagesHow I Treat Disseminated Intravascular Coagulation 2017SaidNo ratings yet
- BR J Haematol 2021 Adelborg Disseminated Intravascular CoagulationDocument16 pagesBR J Haematol 2021 Adelborg Disseminated Intravascular CoagulationSergio Alberto Sulub NavarreteNo ratings yet
- 2023 Article 1088Document18 pages2023 Article 1088Elizabeth Leonor Zamora MarcilloNo ratings yet
- Sepsis - The American Journal of Medicine (2007)Document11 pagesSepsis - The American Journal of Medicine (2007)Jmv VegaNo ratings yet
- JCM 12 03188 With CoverDocument24 pagesJCM 12 03188 With CoverNOTAS GINECONo ratings yet
- Vascular Responses to PathogensFrom EverandVascular Responses to PathogensFelicity N.E. GavinsNo ratings yet
- Current Concepts in The Management of Primary HypeDocument9 pagesCurrent Concepts in The Management of Primary Hypeoki harisandiNo ratings yet
- Bone Marrow Aspirate and Biopsy: A Pathologist's Perspective. II. Interpretation of The Bone Marrow Aspirate and BiopsyDocument49 pagesBone Marrow Aspirate and Biopsy: A Pathologist's Perspective. II. Interpretation of The Bone Marrow Aspirate and Biopsysarmad rizwanNo ratings yet
- How I Treat Disseminated Intravascular CoagulationDocument10 pagesHow I Treat Disseminated Intravascular CoagulationgiopscribdNo ratings yet
- Rubin 1992Document9 pagesRubin 1992oki harisandiNo ratings yet
- Cid PDFDocument21 pagesCid PDFPaola TabaresNo ratings yet
- Disseminated Intravascular Coagulation: A Practical ApproachDocument7 pagesDisseminated Intravascular Coagulation: A Practical Approachoki harisandiNo ratings yet
- Summary of RA treatment guideline recommendationsDocument10 pagesSummary of RA treatment guideline recommendationsoki harisandiNo ratings yet
- Disseminated Intravascular Coagulation: A Practical ApproachDocument7 pagesDisseminated Intravascular Coagulation: A Practical Approachoki harisandiNo ratings yet
- Wa0006 PDFDocument8 pagesWa0006 PDFAlejandro MerinoNo ratings yet
- Guidelines For Cryoprecipitate Transfusion: General ConsiderationsDocument5 pagesGuidelines For Cryoprecipitate Transfusion: General Considerationsoki harisandiNo ratings yet
- DT DKD Oki HDocument33 pagesDT DKD Oki Hoki harisandiNo ratings yet
- post-ACS DepressionDocument18 pagespost-ACS Depressionoki harisandiNo ratings yet
- Structure & Written Expression Test PrepDocument24 pagesStructure & Written Expression Test PrepyhoulhandhariNo ratings yet
- ARDS ClassificationDocument4 pagesARDS Classificationoki harisandiNo ratings yet
- Who Pain LadderDocument1 pageWho Pain LadderRezky 'kiki' Oktarianti SyahputriNo ratings yet
- Anginal EquivalentDocument20 pagesAnginal Equivalentoki harisandiNo ratings yet
- Makalah Yang Berjudul "MANAJEMEN PERSEDIAAN "Document24 pagesMakalah Yang Berjudul "MANAJEMEN PERSEDIAAN "van der b becksNo ratings yet
- The World Health Organization Three-Step Analgesic Ladder PDFDocument2 pagesThe World Health Organization Three-Step Analgesic Ladder PDFNanang HardiansyahNo ratings yet
- Practice Structure H PDFDocument6 pagesPractice Structure H PDFSyarief ZeinNo ratings yet
- Toefl 12345Document1 pageToefl 12345oki harisandiNo ratings yet
- Tips and Strategies On Structure and Written ExpressionDocument25 pagesTips and Strategies On Structure and Written ExpressionShantal PolitNo ratings yet
- Top 10 Pearls For The Recognition, Evaluation, And.246Document16 pagesTop 10 Pearls For The Recognition, Evaluation, And.246Vemuri SrinivasNo ratings yet
- Title, Byline, Abstract, KeywordsDocument11 pagesTitle, Byline, Abstract, KeywordsHappy WKNo ratings yet
- Neonatal SepsisDocument4 pagesNeonatal SepsisAudhrey BNo ratings yet
- Advance PathophysiologyDocument6 pagesAdvance PathophysiologyRhada M.No ratings yet
- Guidelines of Clinical & Public Health Management of Melioidosis in PahangDocument55 pagesGuidelines of Clinical & Public Health Management of Melioidosis in PahangSoon MuvenNo ratings yet
- Statement On Maternal SepsisDocument4 pagesStatement On Maternal SepsisIvonne Maritza TabaresNo ratings yet
- Nutritional Needs With SepsisDocument19 pagesNutritional Needs With Sepsisapi-319236078No ratings yet
- Nej Mo A 0810625Document15 pagesNej Mo A 0810625Catherine MorrisNo ratings yet
- Sepsis PathoDocument8 pagesSepsis PathoPatricia BringasNo ratings yet
- Antibiotic-Guideline-for-Neonatal SepsisDocument13 pagesAntibiotic-Guideline-for-Neonatal SepsisNada AhmedNo ratings yet
- ECG Changes During Septic Shock PDFDocument10 pagesECG Changes During Septic Shock PDFandikaisnaeniNo ratings yet
- Sepsis, Pathophysiology and Clinical Management (BMJ, 2016)Document20 pagesSepsis, Pathophysiology and Clinical Management (BMJ, 2016)Juan Luis Nuñez AravenaNo ratings yet
- Impact of Time To Antibiotic Therapy On Clinical Outcome I 2021 Clinical MicDocument7 pagesImpact of Time To Antibiotic Therapy On Clinical Outcome I 2021 Clinical MicSusanyi ErvinNo ratings yet
- A House Officer's Approach To DengueDocument9 pagesA House Officer's Approach To DengueBaihaqi SaharunNo ratings yet
- Aplication Progress of Modified Early Warning Score in General DepartmentsDocument10 pagesAplication Progress of Modified Early Warning Score in General DepartmentsFemyLealNo ratings yet
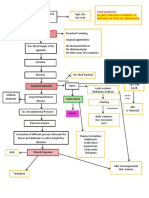
- CPC - Appendicitis (Flowchart)Document1 pageCPC - Appendicitis (Flowchart)Milet NacionalesNo ratings yet
- Trauma Pancreas ManagementDocument20 pagesTrauma Pancreas Managementazis aimaduddinNo ratings yet
- Bundles of Care at IcuDocument134 pagesBundles of Care at IcusamiNo ratings yet
- Management of The Urologic Sepsis SyndromeDocument10 pagesManagement of The Urologic Sepsis SyndromeNur Syamsiah MNo ratings yet
- Learning Guide 18: Animal Health Care Service NTQF Level-IVDocument105 pagesLearning Guide 18: Animal Health Care Service NTQF Level-IVRafez JoneNo ratings yet
- WHO 2019 nCoV Therapeutics 2022.4 EngDocument142 pagesWHO 2019 nCoV Therapeutics 2022.4 Engelsie versieNo ratings yet
- Evaluation and Management of Suspected Sepsis and Septic Shock in AdultsDocument62 pagesEvaluation and Management of Suspected Sepsis and Septic Shock in AdultsGiussepe Chirinos CalderonNo ratings yet
- Surviving Sepsis Campaign International Guidelines.20Document55 pagesSurviving Sepsis Campaign International Guidelines.20CynthiaNo ratings yet
- Shock PDFDocument15 pagesShock PDFWenny AgustinNo ratings yet
- Free 120 March 2021 Explanation 2Document62 pagesFree 120 March 2021 Explanation 2Enrique ParedesNo ratings yet
- Campbell 2006Document9 pagesCampbell 2006Sílvia TrindadeNo ratings yet
- Lepe Zuniga2019 PDFDocument6 pagesLepe Zuniga2019 PDFWening Dewi HapsariNo ratings yet