You might also like
- Unani Medicine in India WebDocument122 pagesUnani Medicine in India WebHiramandalam Patanjali100% (2)
- Non Invasive VentilationDocument442 pagesNon Invasive Ventilationagnese valentiniNo ratings yet
- Week 7 - Nail Disorder and DiseasesDocument46 pagesWeek 7 - Nail Disorder and DiseasesGinalynRapirapHuitNo ratings yet
- COCOLIFE Heathcare Reimbursement FormDocument2 pagesCOCOLIFE Heathcare Reimbursement FormMJVP0% (1)
- The Association of Blood Pressure and Primary Open-Angle Glaucoma: A Meta-AnalysisDocument23 pagesThe Association of Blood Pressure and Primary Open-Angle Glaucoma: A Meta-AnalysisSarah Martinauli HarahapNo ratings yet
- Korean COMPASS-31Document11 pagesKorean COMPASS-31Margareth HildariaNo ratings yet
- Korean SCOPA AUTDocument6 pagesKorean SCOPA AUTMargareth HildariaNo ratings yet
- CSF ParkinsonDocument4 pagesCSF ParkinsonYunita Christiani BiyangNo ratings yet
- Pharmacotherapy For Diabetic Peripheral Neuropathy Pain and Quality of LifeDocument11 pagesPharmacotherapy For Diabetic Peripheral Neuropathy Pain and Quality of LifeAF KoasNo ratings yet
- Panda 2021Document9 pagesPanda 2021rayan1996.officialNo ratings yet
- 60 - Minocycline Combination Therapy Withfluvoxaminein Moderate-To-Severe Obsessive-Compulsive Disorder, A Placebo-Controlled, Double-Blind, Randomized TrialDocument10 pages60 - Minocycline Combination Therapy Withfluvoxaminein Moderate-To-Severe Obsessive-Compulsive Disorder, A Placebo-Controlled, Double-Blind, Randomized TrialPaula CantalapiedraNo ratings yet
- Efficacy and Acceptability of Pharmacological Treat-Ments For Depressive Disorders in Primary Care: Systematic Review and Network Meta-AnalysisDocument11 pagesEfficacy and Acceptability of Pharmacological Treat-Ments For Depressive Disorders in Primary Care: Systematic Review and Network Meta-AnalysisPutri YingNo ratings yet
- Greek SCOPA-AUTDocument6 pagesGreek SCOPA-AUTMargareth HildariaNo ratings yet
- Autonomic Function and Motor Subtypes in Parkinson's DiseaseDocument11 pagesAutonomic Function and Motor Subtypes in Parkinson's DiseaseCarla AlmeidaNo ratings yet
- Equilibrio y Movilidad en Pacientes Con Enfermedad de Parkinson Recién Diagnosticada Seguimiento de Cinco Años de Una Cohorte en El Norte de SueciaDocument10 pagesEquilibrio y Movilidad en Pacientes Con Enfermedad de Parkinson Recién Diagnosticada Seguimiento de Cinco Años de Una Cohorte en El Norte de SueciacamilaNo ratings yet
- RamachandranDocument9 pagesRamachandranjojobaggins100% (1)
- Second Generation Antipsychotic-Induced Obsessive-Compulsive Symptoms in Schizophrenia: A Review of The Experimental LiteratureDocument17 pagesSecond Generation Antipsychotic-Induced Obsessive-Compulsive Symptoms in Schizophrenia: A Review of The Experimental LiteratureDerek TantaleánNo ratings yet
- UA ParkinsonDocument6 pagesUA ParkinsonNgọc LamNo ratings yet
- Journal Pone 0276012Document15 pagesJournal Pone 0276012hardi adiyatmaNo ratings yet
- Autonomic Dysregulation Cognition and Fatigue in People With Depression and in Active and Healthy Controls Observational Cohort StudyDocument11 pagesAutonomic Dysregulation Cognition and Fatigue in People With Depression and in Active and Healthy Controls Observational Cohort StudyValentina De La PazNo ratings yet
- tmp1329 TMPDocument11 pagestmp1329 TMPFrontiersNo ratings yet
- Pone 0159966Document16 pagesPone 0159966JESICA PAOLA RODRIGUEZ PEREZNo ratings yet
- Slide Jurnal Efusi PleuraDocument8 pagesSlide Jurnal Efusi PleuraolakasturiNo ratings yet
- Effects of Risperidone and Olanzapine Dose Reduction On Cognitive Function in Stable Patients With SchizophreniaDocument6 pagesEffects of Risperidone and Olanzapine Dose Reduction On Cognitive Function in Stable Patients With Schizophreniawen zhangNo ratings yet
- Panss 78Document24 pagesPanss 78ijmalNo ratings yet
- Neu 2015 4192Document14 pagesNeu 2015 4192Dea RitungNo ratings yet
- Possible Effect of Acupuncture in Autism Spectrum DisorderDocument3 pagesPossible Effect of Acupuncture in Autism Spectrum DisorderPaul NguyenNo ratings yet
- Age at Onset and Parkinson Disease PhenotypeDocument9 pagesAge at Onset and Parkinson Disease Phenotypemariel gonzalezNo ratings yet
- Z Al-Roubaie - 2020Document12 pagesZ Al-Roubaie - 2020Kossay ZaouiNo ratings yet
- Atrofia Multiples Sitemas 2009Document7 pagesAtrofia Multiples Sitemas 2009Miztli CervantesNo ratings yet
- Tratamiento en APP 2013Document34 pagesTratamiento en APP 2013Mauricio EtchegarayNo ratings yet
- Journal Pone 0070571Document8 pagesJournal Pone 0070571Basil AlsaadiNo ratings yet
- A Systematic Review and Network Meta-Analysis To AssessDocument13 pagesA Systematic Review and Network Meta-Analysis To AssessastrogliaNo ratings yet
- Sepede G, 2016Document21 pagesSepede G, 2016Bianca PerezNo ratings yet
- Mortality in Pediatric Acute Respiratory Distress Syndrome: A Systematic Review and Meta-AnalysisDocument9 pagesMortality in Pediatric Acute Respiratory Distress Syndrome: A Systematic Review and Meta-Analysisesya putrri oktareginaNo ratings yet
- Heterogenitate BPDocument8 pagesHeterogenitate BPCarmen CiursaşNo ratings yet
- Lurasidone For Adolescent SchizophreniaDocument11 pagesLurasidone For Adolescent Schizophreniaromany hosnyNo ratings yet
- (1479683X - European Journal of Endocrinology) THERAPY OF ENDOCRINE DISEASE - A systematic review and meta-analysis of α-lipoic acid in the treatment of diabetic peripheral neuropathyDocument7 pages(1479683X - European Journal of Endocrinology) THERAPY OF ENDOCRINE DISEASE - A systematic review and meta-analysis of α-lipoic acid in the treatment of diabetic peripheral neuropathyHendri YantoNo ratings yet
- 2014 KimDocument6 pages2014 Kimnermal93No ratings yet
- Barrionuevo 2018Document7 pagesBarrionuevo 2018hlwNo ratings yet
- Leukotriene Antagonists in Nasal Polyposis: A Meta-Analysis and Systematic ReviewDocument8 pagesLeukotriene Antagonists in Nasal Polyposis: A Meta-Analysis and Systematic ReviewRezaNo ratings yet
- Cognitive Impairment in Patients With Parkinsons Disease A 30month Followup StudyDocument11 pagesCognitive Impairment in Patients With Parkinsons Disease A 30month Followup StudyAisyahImasSetiawatiNo ratings yet
- PTJ 1620Document18 pagesPTJ 1620Martina SimangunsongNo ratings yet
- Dysautonomia Is Associated With Structural and Functional Alterations in Parkinson DiseaseDocument13 pagesDysautonomia Is Associated With Structural and Functional Alterations in Parkinson DiseaseolgaguerreroNo ratings yet
- Lian 2021Document11 pagesLian 2021RickyconsuegraNo ratings yet
- Acta Psychiatr Scand - 2013 - Bourne - Neuropsychological Testing of Cognitive Impairment in Euthymic Bipolar Disorder AnDocument14 pagesActa Psychiatr Scand - 2013 - Bourne - Neuropsychological Testing of Cognitive Impairment in Euthymic Bipolar Disorder AnJeriesnal GamingNo ratings yet
- Duailibi 2017Document7 pagesDuailibi 2017Iván Tonatiuh Jiménez MolinaNo ratings yet
- Factors Associated With Patellofemoral Pain Syndrome: A Systematic ReviewDocument17 pagesFactors Associated With Patellofemoral Pain Syndrome: A Systematic Reviewנתנאל מושקוביץNo ratings yet
- Dexlansoprazole Vs Esomeprazole ERGEDocument12 pagesDexlansoprazole Vs Esomeprazole ERGELuis Felipe Gomez AndradeNo ratings yet
- Parkinson Subtypes Progress Differently PDFDocument8 pagesParkinson Subtypes Progress Differently PDFParisNo ratings yet
- RMD Open-2016-KalyoncuDocument9 pagesRMD Open-2016-KalyoncuneoslaveNo ratings yet
- Evaluation and Comparison of Three Assays For Molecular Detection of Spinal Muscular AtrophyDocument11 pagesEvaluation and Comparison of Three Assays For Molecular Detection of Spinal Muscular AtrophyRainie PhamNo ratings yet
- Meta-Analysis of Randomized Controlled Trials On TDocument18 pagesMeta-Analysis of Randomized Controlled Trials On TIbrahim SabraNo ratings yet
- A Systematic Review of Neuropsychiatric and Cognitive AssessmentsDocument12 pagesA Systematic Review of Neuropsychiatric and Cognitive Assessmentskarenina10No ratings yet
- Fnins 13 00472Document18 pagesFnins 13 00472Infinity PsychiatryNo ratings yet
- Texte 9Document12 pagesTexte 9Clara ScemamaNo ratings yet
- Congantive Metobolic Symdrome Case StudyDocument6 pagesCongantive Metobolic Symdrome Case StudyPrachiti ChavanNo ratings yet
- Development and Validation of The FSIQ-RMS A New PDocument14 pagesDevelopment and Validation of The FSIQ-RMS A New Psda asfNo ratings yet
- Skripsi Full Teks Tanpa Bab Pembahasan PDFDocument68 pagesSkripsi Full Teks Tanpa Bab Pembahasan PDFahmad faisalNo ratings yet
- Skripsi Full Teks Tanpa Bab Pembahasan PDFDocument68 pagesSkripsi Full Teks Tanpa Bab Pembahasan PDFahmad faisalNo ratings yet
- BJP 2011 Thase 501 7Document8 pagesBJP 2011 Thase 501 7Joanne Suguitan- GarciaNo ratings yet
- BD 3Document14 pagesBD 3aboharaNo ratings yet
- Review Dysphagia Tto PoststrokeDocument7 pagesReview Dysphagia Tto PoststrokeTrinidad OdaeNo ratings yet
- C4T Pulmonary Stenosis - WebDocument2 pagesC4T Pulmonary Stenosis - WebraosudhNo ratings yet
- The Top 15 Best Selling Cancer Drugs in 2022Document16 pagesThe Top 15 Best Selling Cancer Drugs in 2022Soma YasaswiNo ratings yet
- Unit 4 Reading (Lisnawatie)Document2 pagesUnit 4 Reading (Lisnawatie)Lisna WatieNo ratings yet
- ProjDocument37 pagesProjM LubisNo ratings yet
- Nurs362 Professional Development PlanDocument4 pagesNurs362 Professional Development Planapi-272566401No ratings yet
- Feline Anaplasmosis 2020Document14 pagesFeline Anaplasmosis 2020Birdella GwenNo ratings yet
- Agenda Zoonotic Influenza Webinar - 8-9 May 2023Document2 pagesAgenda Zoonotic Influenza Webinar - 8-9 May 2023haniefahmadNo ratings yet
- DR René KABERA :this Situation Was AlarmingDocument2 pagesDR René KABERA :this Situation Was AlarmingKABERA RENENo ratings yet
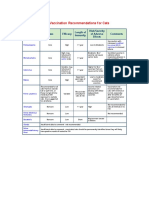
- AVMA Vaccination Recommendations F or CatsDocument2 pagesAVMA Vaccination Recommendations F or CatsHazim Azmi Al-QadryNo ratings yet
- Medical Problems in The 19th CenturyDocument9 pagesMedical Problems in The 19th CenturyWill TeeceNo ratings yet
- BOPTDocument7 pagesBOPThelmuth0207No ratings yet
- Bronchopneumonia TreatmentDocument2 pagesBronchopneumonia TreatmentJam RapaconNo ratings yet
- Breast ScreeningDocument76 pagesBreast ScreeningBenny KurniawanNo ratings yet
- Us ObDocument16 pagesUs ObWahyu RianiNo ratings yet
- Malaria ProtocolDocument8 pagesMalaria ProtocolPERFECT CLASSESNo ratings yet
- 3rd Year-Community Medicine Study GuideDocument78 pages3rd Year-Community Medicine Study GuideNasir HussainNo ratings yet
- School Health Examination Form EDITEDDocument2 pagesSchool Health Examination Form EDITEDjustine mae villaruelNo ratings yet
- 1 Running Head: Cauti Bundle EffectivenessDocument9 pages1 Running Head: Cauti Bundle Effectivenessapi-544117547No ratings yet
- CSS Perio ObieDocument11 pagesCSS Perio ObieRobbyRamadhonieNo ratings yet
- Safety ProgramDocument24 pagesSafety ProgramJuan CruzNo ratings yet
- Informed Consent For Nursing ProceduresDocument2 pagesInformed Consent For Nursing ProceduresZNo ratings yet
- Report of Medical Examination and Vaccination RecordDocument14 pagesReport of Medical Examination and Vaccination RecordHrishi WaghNo ratings yet
- Issues Paper Kim Werschler and Becky WerschlerDocument12 pagesIssues Paper Kim Werschler and Becky WerschlerKimberly WerschlerNo ratings yet
- Role of Statistics in HealthcareDocument4 pagesRole of Statistics in HealthcareSumita ChatterjeeNo ratings yet
- Reviewing Harm Reduction For People Who Inject Drugs in Asia - The Necessity For GrowthDocument5 pagesReviewing Harm Reduction For People Who Inject Drugs in Asia - The Necessity For GrowthAura NirwanaNo ratings yet
- PulpotecDocument2 pagesPulpotecFeras Al-ZbounNo ratings yet