You might also like
- Fetal Circulation: Dr. Khush BakhtDocument29 pagesFetal Circulation: Dr. Khush BakhtKhush BakhtNo ratings yet
- Fetal Cardiology: A Practical Approach to Diagnosis and ManagementFrom EverandFetal Cardiology: A Practical Approach to Diagnosis and ManagementNo ratings yet
- Fetal CirculationDocument39 pagesFetal CirculationjerlinNo ratings yet
- Human Body Book | Introduction to the Vascular System | Children's Anatomy & Physiology EditionFrom EverandHuman Body Book | Introduction to the Vascular System | Children's Anatomy & Physiology EditionNo ratings yet
- Embryology of The HeartDocument65 pagesEmbryology of The Heartnisha24No ratings yet
- Fetal CirculationDocument20 pagesFetal CirculationMuhyeeSalaIdjadNo ratings yet
- 4 EL Husseinys Essentials of Cardiovascular System @eduwaves360Document236 pages4 EL Husseinys Essentials of Cardiovascular System @eduwaves360ahmed_abu_alrobNo ratings yet
- FetalcirculationDocument32 pagesFetalcirculationannu panchalNo ratings yet
- Circulatory System - Part 2 4-8-14 For BBDocument23 pagesCirculatory System - Part 2 4-8-14 For BBroman7dbNo ratings yet
- Fetus Circulation LectureDocument28 pagesFetus Circulation LecturecandrastefannNo ratings yet
- Fetal CirculationDocument26 pagesFetal CirculationMuskan TiwariNo ratings yet
- مذكرة فرست الزمالة المجمعةDocument160 pagesمذكرة فرست الزمالة المجمعةmahi_elsemary7011100% (1)
- Fetalcirculation 181202080431 1Document27 pagesFetalcirculation 181202080431 1mukiza FestusNo ratings yet
- Fetal Circulation 4Document24 pagesFetal Circulation 4UmarNo ratings yet
- Development of The HeartDocument19 pagesDevelopment of The HeartYusuf UmarNo ratings yet
- Fetal CirculationDocument14 pagesFetal Circulationjoel david knda mj100% (3)
- Fetal CirculationDocument27 pagesFetal CirculationSureshChevagoniNo ratings yet
- Congenital Heart DIseasesDocument3 pagesCongenital Heart DIseasesAshan BopitiyaNo ratings yet
- Dr. Nia-Fisiologi Sirkulasi Fetus, Bayi, DewasaDocument21 pagesDr. Nia-Fisiologi Sirkulasi Fetus, Bayi, DewasaYuliasminde SofyanaNo ratings yet
- Fetal CirculationDocument16 pagesFetal CirculationArunashree ajayNo ratings yet
- Fetal CirculationDocument16 pagesFetal CirculationArunashree ajayNo ratings yet
- Embryonic Development of The HeartDocument11 pagesEmbryonic Development of The HeartMatthew RyanNo ratings yet
- Fetal CirculationDocument2 pagesFetal CirculationTracy88% (8)
- Embryology of CVSDocument63 pagesEmbryology of CVSAdan Iman100% (1)
- Foetal CirculationDocument39 pagesFoetal CirculationDr. Haricharan ANo ratings yet
- Fetal CirculationDocument17 pagesFetal Circulationjibson2354No ratings yet
- Fetal CirculationDocument3 pagesFetal Circulationyusrinastiti100% (1)
- Embryology of Cardiovascular SystemDocument51 pagesEmbryology of Cardiovascular SystemEniola abdullahi AduagbaNo ratings yet
- 1 Fetal CirculationDocument23 pages1 Fetal Circulationmohanad11No ratings yet
- Fetal Circulation in The WombDocument2 pagesFetal Circulation in The WombChristineAlaNo ratings yet
- Cardiovascular System Embryology Applied Aspects: Preceptor Prof S S KothariDocument109 pagesCardiovascular System Embryology Applied Aspects: Preceptor Prof S S KothariBir Singh100% (1)
- Fetal CirculationDocument19 pagesFetal Circulation3sshhhNo ratings yet
- Fetal CirculationDocument62 pagesFetal CirculationRed Williams100% (4)
- Lecture 3 NCM 107Document7 pagesLecture 3 NCM 107Anna YepisNo ratings yet
- Update Fetal Circulation - MDM AmyDocument10 pagesUpdate Fetal Circulation - MDM AmyNana Yunus100% (1)
- Fetal CirculationDocument2 pagesFetal CirculationCJ PorrasNo ratings yet
- Formation of Blood and ArteriesDocument7 pagesFormation of Blood and ArteriesAlyssa VillanoNo ratings yet
- Jantung (The Heart)Document24 pagesJantung (The Heart)JoePutraNo ratings yet
- Semeiology of CvsDocument64 pagesSemeiology of CvsIris BakerNo ratings yet
- Cardiovascular SystemDocument37 pagesCardiovascular Systemrazoon haroonNo ratings yet
- Development of The Heart and Blood VesselsDocument10 pagesDevelopment of The Heart and Blood VesselsAbigail ChristisnNo ratings yet
- Embryology of Cardiovascular System 1: DR - Navajyothi, Mbbs MDDocument59 pagesEmbryology of Cardiovascular System 1: DR - Navajyothi, Mbbs MDcheckmateNo ratings yet
- RJI - Fetal CirculationDocument10 pagesRJI - Fetal CirculationgalaetiNo ratings yet
- Fetal CirculationDocument22 pagesFetal CirculationJSeasharkNo ratings yet
- Development of The HeartDocument4 pagesDevelopment of The HeartMatthew GiscombeNo ratings yet
- Embryology of Heart and LungDocument7 pagesEmbryology of Heart and Lungavinash dhameriyaNo ratings yet
- Development Cardio 1Document39 pagesDevelopment Cardio 1Deniz asmazNo ratings yet
- Neonatal Physiology: Teka Siebenaler RRT Cardiopulmonary Services University of Minnesota Amplatz Children's HospitalDocument29 pagesNeonatal Physiology: Teka Siebenaler RRT Cardiopulmonary Services University of Minnesota Amplatz Children's HospitalStrept PneumoniaNo ratings yet
- AsdaDocument42 pagesAsdaratchagarajaNo ratings yet
- Fetal CirculationDocument19 pagesFetal CirculationAlozie PrestigeNo ratings yet
- Cardiovascular System Heart ModuleDocument19 pagesCardiovascular System Heart Modulebadodong700No ratings yet
- Fetal Circulation...Document2 pagesFetal Circulation...Ezra Dizon Manzano100% (1)
- Blood Circulation-DmDocument32 pagesBlood Circulation-DmMathews showsNo ratings yet
- 1 Fetal CirculationDocument21 pages1 Fetal Circulationdr_mohanad100% (1)
- Development of HeartDocument18 pagesDevelopment of HeartBishal BelbaseNo ratings yet
- Tetralogy of Fallot FinaleDocument8 pagesTetralogy of Fallot FinaledawnieciousNo ratings yet
- Pregnancy Induced Hypertension (PIH) Is ADocument14 pagesPregnancy Induced Hypertension (PIH) Is APaul John HipolitoNo ratings yet
- Atria and SeptumDocument29 pagesAtria and SeptumAarushi JainNo ratings yet
- Basic of Clinical Examination For OSCEDocument109 pagesBasic of Clinical Examination For OSCESualeha SohailNo ratings yet
- Physical Fitness AssessmentDocument30 pagesPhysical Fitness AssessmentJingle BellsNo ratings yet
- PALS Precourse Self 2023Document9 pagesPALS Precourse Self 2023Airene SibleNo ratings yet
- Vital Signs RationaleDocument3 pagesVital Signs RationalePhil Pasaol100% (2)
- 5C Assessing Apical - Radial Pulse-3Document2 pages5C Assessing Apical - Radial Pulse-3Marky RoqueNo ratings yet
- Almaghrabi Cardio ExaminationDocument22 pagesAlmaghrabi Cardio ExaminationSagit Nauman81No ratings yet
- Physical Education & Health: Quarter 1 - Module 4&5 Physical Fitness Physiological Indicators (Week 4 & 5)Document28 pagesPhysical Education & Health: Quarter 1 - Module 4&5 Physical Fitness Physiological Indicators (Week 4 & 5)I Love You 3000100% (1)
- My Lecture13 - Cardiovascular PhysiologyDocument16 pagesMy Lecture13 - Cardiovascular PhysiologyVivek ChaudharyNo ratings yet
- Medico Legal Aspects of DeathDocument129 pagesMedico Legal Aspects of Deathkenneth marronNo ratings yet
- Vital SignsDocument6 pagesVital SignsJan Jamison ZuluetaNo ratings yet
- Updated Physiology and Pathophysiology of CSF Circulation - The Pulsatile Vector TheoryDocument18 pagesUpdated Physiology and Pathophysiology of CSF Circulation - The Pulsatile Vector TheorysavitageraNo ratings yet
- Funda (Course Audit)Document16 pagesFunda (Course Audit)Kath-Kath Cubillan RanayNo ratings yet
- Funda Rle Reviewer - (Prelims)Document8 pagesFunda Rle Reviewer - (Prelims)Jhaztene Mae BaniquedNo ratings yet
- FUNDAMENTALS OF NURSING (100 Items)Document10 pagesFUNDAMENTALS OF NURSING (100 Items)Arcon AlvarNo ratings yet
- Handy Guide: We'Ve Also Put Together This - Pulsesensor Starter Project Code FeaturesDocument5 pagesHandy Guide: We'Ve Also Put Together This - Pulsesensor Starter Project Code FeaturesRonaldMartinezNo ratings yet
- Blood Flow Restriction Training Manual: (Type The Company Name) - Error! No Text of Specified Style in Document. 0Document24 pagesBlood Flow Restriction Training Manual: (Type The Company Name) - Error! No Text of Specified Style in Document. 0Dany FernandezNo ratings yet
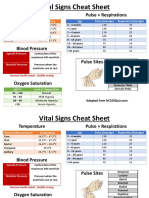
- Temperature Pulse + RespirationsDocument2 pagesTemperature Pulse + RespirationsMarshin Thea Celocia100% (1)
- Physical Assessment of Preeclamptic PatientDocument3 pagesPhysical Assessment of Preeclamptic PatientAndreiNo ratings yet
- F3 Chapter 3 TransportationDocument19 pagesF3 Chapter 3 TransportationJue Hazea GoldshopNo ratings yet
- Latihan Soal Pat K.11Document5 pagesLatihan Soal Pat K.11yeol parkNo ratings yet
- Davidson's McqsDocument145 pagesDavidson's McqsSekhons Akademy100% (3)
- Circulatory System ActivityDocument7 pagesCirculatory System ActivityReginald MalibiranNo ratings yet
- Test Bank For Foundations and Adult Health Nursing 5th Edition Barbara ChristensenDocument6 pagesTest Bank For Foundations and Adult Health Nursing 5th Edition Barbara ChristensenBrianHarrellednyf100% (29)
- Functional Hemodynamic Monitoring PDFDocument10 pagesFunctional Hemodynamic Monitoring PDFPGI AnaesthesiaNo ratings yet
- The 29 Pulses in Chinese MedicineDocument7 pagesThe 29 Pulses in Chinese MedicineJasmine Wild50% (2)
- How 20to 20perform 20a 20physical 20exam 20in 20your 20horseDocument50 pagesHow 20to 20perform 20a 20physical 20exam 20in 20your 20horseThamil ArasanNo ratings yet
- Anamneza I Status InternaDocument12 pagesAnamneza I Status Internatajana91No ratings yet
- Vital SignsDocument10 pagesVital SignsBiway RegalaNo ratings yet
- Techniques of Physical Assessment: Observation /inspection Palpation Percussion AuscultationDocument56 pagesTechniques of Physical Assessment: Observation /inspection Palpation Percussion AuscultationAnna Fayeziah YussophNo ratings yet
- UntitledDocument48 pagesUntitledSamad MaqsoodNo ratings yet