You might also like
- IIA - Altered Tissue PerfusionDocument14 pagesIIA - Altered Tissue PerfusionDharylle CariñoNo ratings yet
- Angina PectorisDocument8 pagesAngina PectorisJoanne LagusadNo ratings yet
- Chest Pain ProtocolDocument7 pagesChest Pain Protocolomar kmr97No ratings yet
- Angina Pectoris, SeminarDocument18 pagesAngina Pectoris, SeminarMuslim GrdkhiwatyNo ratings yet
- Coronary Artherosclerosis - ACS and MIDocument5 pagesCoronary Artherosclerosis - ACS and MIAila HinlogNo ratings yet
- Assignment No.1 OB High Risk Grp.1Document15 pagesAssignment No.1 OB High Risk Grp.1YongNo ratings yet
- Cardiovascular System Diseases Part 1Document22 pagesCardiovascular System Diseases Part 1Prince Rener Velasco PeraNo ratings yet
- Medurg MidtermDocument4 pagesMedurg Midtermmark OrpillaNo ratings yet
- Scenario NCPDocument3 pagesScenario NCPZanie CruzNo ratings yet
- Module 2 ABC-CardioDocument7 pagesModule 2 ABC-Cardiomelba040510No ratings yet
- Care of Clients With Myocardial InfarctionDocument7 pagesCare of Clients With Myocardial InfarctionaryshamyleeNo ratings yet
- NCM 112 MidtermDocument25 pagesNCM 112 MidtermJan Charlie Sophia100% (1)
- Acute Coronary, Angina Pectoris and Myocardial InfractionDocument26 pagesAcute Coronary, Angina Pectoris and Myocardial Infractionabeer alzhoorNo ratings yet
- Coronary Circulation Disorder: Henri Setiawan, S.Kep.,Ners.,M.Si - MedDocument31 pagesCoronary Circulation Disorder: Henri Setiawan, S.Kep.,Ners.,M.Si - MedannisafithrianiNo ratings yet
- Acute Coronary Syndromes GAPDocument25 pagesAcute Coronary Syndromes GAPhhgangurde9323No ratings yet
- Peripheral Arterial Occlusive DiseaseDocument6 pagesPeripheral Arterial Occlusive DiseaseAila HinlogNo ratings yet
- Cardiac Disease NotesDocument4 pagesCardiac Disease NotesKyla Mae JumaritoNo ratings yet
- Chapter 14: Nursing Management: Patients With Coronary Vascular DisordersDocument13 pagesChapter 14: Nursing Management: Patients With Coronary Vascular DisorderskingNo ratings yet
- Nurul Ilmi Hajar (PO.71.3.201.14.1.130) Nurul Khabliana (PO.71.3.201.14.1.131)Document27 pagesNurul Ilmi Hajar (PO.71.3.201.14.1.130) Nurul Khabliana (PO.71.3.201.14.1.131)Nurulilmi hajarNo ratings yet
- MINI CP Angina PectorisDocument11 pagesMINI CP Angina Pectorisyasira100% (1)
- Angina PectorisDocument19 pagesAngina PectorisRenas SalayNo ratings yet
- Problem Based Learning Cardiovascular System: 2nd GroupDocument47 pagesProblem Based Learning Cardiovascular System: 2nd GroupClaudia Narinda R. PNo ratings yet
- Cardiac PPT SeminarDocument129 pagesCardiac PPT SeminarjoashannNo ratings yet
- Riyadh Ali 4/9/12 MDSC3311Document6 pagesRiyadh Ali 4/9/12 MDSC3311Hugh JacobsNo ratings yet
- Angina Pectoris: Prepared byDocument30 pagesAngina Pectoris: Prepared byjyothiNo ratings yet
- Angina Pectoris (Stable Angina) Nursing Care Management - Study GuideDocument8 pagesAngina Pectoris (Stable Angina) Nursing Care Management - Study GuideSachin Singh100% (1)
- Angina Pectoris: Stable Angina Unstable AnginaDocument3 pagesAngina Pectoris: Stable Angina Unstable AnginaDanesa MadoNo ratings yet
- Hematologic Acute or Chronic Problems: ScenarioDocument36 pagesHematologic Acute or Chronic Problems: ScenariobhavanaNo ratings yet
- Second Problem Emergency Medicine Block: "Give Your Heart A Break"Document59 pagesSecond Problem Emergency Medicine Block: "Give Your Heart A Break"waraney palitNo ratings yet
- Guidelines Applied To Practice (GAP) : American College of Cardiology, Puerto Rico ChapterDocument27 pagesGuidelines Applied To Practice (GAP) : American College of Cardiology, Puerto Rico ChapterYenza FaheraNo ratings yet
- Drug StudyDocument7 pagesDrug StudyCassie ValderramaNo ratings yet
- PY6030 Term 1Document13 pagesPY6030 Term 1AlexaJoiceJumao-AsNo ratings yet
- NCM 118 - Lesson 8 (Acute Ischemic Heart Diseases)Document9 pagesNCM 118 - Lesson 8 (Acute Ischemic Heart Diseases)Bobby Christian DuronNo ratings yet
- Acute Coronary SyndromeDocument27 pagesAcute Coronary SyndromeSahr Anne Pilar B. ParreñoNo ratings yet
- Coronary AtherosclerosisDocument3 pagesCoronary AtherosclerosisGwyn Oona Florence ForroNo ratings yet
- Oxy Nov 9Document4 pagesOxy Nov 9Sofronio OmboyNo ratings yet
- Atherosclerosis Angina Pectoris Myocardial InfarctionDocument2 pagesAtherosclerosis Angina Pectoris Myocardial InfarctionKaren Mae AlcantaraNo ratings yet
- Anginapectoris ClassDocument45 pagesAnginapectoris Classjyothi lekshmi sNo ratings yet
- Mari Zita Spa OnDocument57 pagesMari Zita Spa OnMarty BrownNo ratings yet
- Myocardial InfarctionDocument28 pagesMyocardial Infarctionshaitabligan100% (1)
- Angina PectorisDocument7 pagesAngina PectorisTruptilata SahooNo ratings yet
- Acute Coronary SyndromeDocument42 pagesAcute Coronary SyndromeGorgieNo ratings yet
- Myocardial Infarction Handout 1Document3 pagesMyocardial Infarction Handout 1Alekxandra Erl ManansalaNo ratings yet
- Week 2 Individual AssignmentDocument1 pageWeek 2 Individual AssignmentPaul SahagunNo ratings yet
- Cardio DiseasesDocument77 pagesCardio Diseasesrea bentayaoNo ratings yet
- Cardiac EmergencyDocument34 pagesCardiac EmergencyRima HannaniNo ratings yet
- Reason For Needing Health Care: Key Problem / ND: Noncompliance Key Problem / NDDocument6 pagesReason For Needing Health Care: Key Problem / ND: Noncompliance Key Problem / NDnursing concept mapsNo ratings yet
- السمنار الجديد PDFDocument17 pagesالسمنار الجديد PDFعمار ياسرNo ratings yet
- Algorithms of Care (Myocardial Infarction)Document3 pagesAlgorithms of Care (Myocardial Infarction)Julius Delos SantosNo ratings yet
- Old CartsDocument3 pagesOld CartsinggitluthfiazahraNo ratings yet
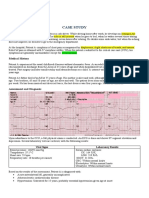
- Case Study With ECG Reading OcañaDocument3 pagesCase Study With ECG Reading OcañaNicole Chloe OcanaNo ratings yet
- WK1 - Inflammatory Heart Failure Infectious DiseaseDocument4 pagesWK1 - Inflammatory Heart Failure Infectious DiseaseJhaji Mei Margarete CasiNo ratings yet
- General Medicine and Surgery For Dental Practition PDFDocument7 pagesGeneral Medicine and Surgery For Dental Practition PDFAnnanyaNo ratings yet
- Angina PectorisDocument8 pagesAngina PectorisPrince DuNo ratings yet
- Ardhendu Sinha Ray - Essentials of Internal Medicine-Jp Medical LTD (2017) - 92-105Document14 pagesArdhendu Sinha Ray - Essentials of Internal Medicine-Jp Medical LTD (2017) - 92-105Noveno CNo ratings yet
- NCP: Acute Coronary Syndrome: Nursing DiagnosisDocument17 pagesNCP: Acute Coronary Syndrome: Nursing DiagnosisICa MarlinaNo ratings yet
- Cardio InternetDocument46 pagesCardio InternetnaimNo ratings yet
- (NCM 410-M) Trans 1 - Altered Tissue PerfusionDocument6 pages(NCM 410-M) Trans 1 - Altered Tissue PerfusionANDREA JUSTINE CARDEÑONo ratings yet
- Transoesophageal Echocardiography in Anaesthesia and Intensive Care MedicineFrom EverandTransoesophageal Echocardiography in Anaesthesia and Intensive Care MedicineJan PoelaertNo ratings yet
- Pericarditis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPericarditis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (3)
- Cambridge - Science Skills Builder 6 BookDocument15 pagesCambridge - Science Skills Builder 6 BookRasha Ali100% (2)
- ANP Human Behavior and Life ProcessDocument15 pagesANP Human Behavior and Life ProcessRinal BaradNo ratings yet
- Heart Sounds: Presented by Group 2A & 3ADocument13 pagesHeart Sounds: Presented by Group 2A & 3AMeow Catto100% (1)
- 9700 BIOLOGY: MARK SCHEME For The May/June 2010 Question Paper For The Guidance of TeachersDocument6 pages9700 BIOLOGY: MARK SCHEME For The May/June 2010 Question Paper For The Guidance of TeachersLuis YamnelNo ratings yet
- Cardiac PhysiologDocument30 pagesCardiac PhysiologKannan GNo ratings yet
- Drug StudyDocument5 pagesDrug StudyAshley Jane MacapayadNo ratings yet
- PhDthesisAASL PDFDocument168 pagesPhDthesisAASL PDFmuhammad alamNo ratings yet
- QuizbowlDocument23 pagesQuizbowlOlive NNo ratings yet
- Career Probationary Firefighter Dies During SCBA ConfidenceDocument43 pagesCareer Probationary Firefighter Dies During SCBA ConfidenceScott AtkinsonNo ratings yet
- Department of Education Division of Leyte Taberna National High SchoolDocument3 pagesDepartment of Education Division of Leyte Taberna National High SchoolSheila May Tapales TabonNo ratings yet
- Assignment 1 Health AssessmentDocument8 pagesAssignment 1 Health AssessmentHung PhanNo ratings yet
- Adempas Epar Public Assessment Report enDocument118 pagesAdempas Epar Public Assessment Report enANA MARIA ORTEGON BUITRAGONo ratings yet
- ?1 - Chest X-Ray Interpretation - A Structured Approach - Radiology - OSCEDocument55 pages?1 - Chest X-Ray Interpretation - A Structured Approach - Radiology - OSCESupaluk Mod ChuencheepNo ratings yet
- DR Kupe - ECGDocument14 pagesDR Kupe - ECGIrfan ZiadNo ratings yet
- Year End Test in Science 9: Republic of The Philippines Region III Guzmanville, Sto. Cristo, City of San Jose Del MonteDocument5 pagesYear End Test in Science 9: Republic of The Philippines Region III Guzmanville, Sto. Cristo, City of San Jose Del Monteberith grace magcalasNo ratings yet
- Introduction To The CvsDocument43 pagesIntroduction To The CvsParmesh PandeyNo ratings yet
- Chapter 31 - Assessment and Management of Patients With Vascular DisordersDocument7 pagesChapter 31 - Assessment and Management of Patients With Vascular DisordersMichael Boado100% (1)
- Ecg Level 3 Precise Calculation of Cardiac AxisDocument44 pagesEcg Level 3 Precise Calculation of Cardiac Axismoneer chanceNo ratings yet
- Concept Map Chap7 General Survey Vital SignsDocument1 pageConcept Map Chap7 General Survey Vital SignsEvelyn MoatsNo ratings yet
- CH 04 DDocument34 pagesCH 04 DVijayRajNo ratings yet
- 3j Cuci - The Circulatory System WorksheetDocument6 pages3j Cuci - The Circulatory System Worksheetcharmaine nwankwoNo ratings yet
- The Study of Operation Theatre Utilization Amri Hospital BhubaneswarDocument46 pagesThe Study of Operation Theatre Utilization Amri Hospital BhubaneswarRakesh Kumar AcharjyaNo ratings yet
- Medicina 58 01115 v2Document21 pagesMedicina 58 01115 v2silmanuryanzila2705No ratings yet
- Drug StudyDocument4 pagesDrug StudyTeanu Jose Gabrillo TamayoNo ratings yet
- Circulatory SystemDocument2 pagesCirculatory SystemDearly Niña OsinsaoNo ratings yet
- Postnatal AssessmentDocument8 pagesPostnatal Assessmentsaritha OrugantiNo ratings yet
- 11 The Pericardium and The HeartDocument39 pages11 The Pericardium and The HeartJeff D'erique Ozil TettehNo ratings yet
- 3doodler Case StudyDocument8 pages3doodler Case StudyShakeel RehmanNo ratings yet
- MODULE I Elec 102 PDFDocument23 pagesMODULE I Elec 102 PDFEsmareldah Henry SirueNo ratings yet
- Abstract BookDocument170 pagesAbstract BookausterkoolNo ratings yet