You might also like
- Fármacos AntihipertensivosDocument15 pagesFármacos AntihipertensivosEricka SanchezNo ratings yet
- Slide HiperdiaDocument15 pagesSlide HiperdiaYannaFreire100% (1)
- DownloadDocument7 pagesDownloadjulyanne silvaNo ratings yet
- 150-Texto Artigo-309-1-10-20170620Document5 pages150-Texto Artigo-309-1-10-20170620cyprianoNo ratings yet
- Nefro 2Document9 pagesNefro 2Felix ApazaNo ratings yet
- Clínica Médica: Questão 1 Questão 2Document23 pagesClínica Médica: Questão 1 Questão 2Frank Camargo MartinsNo ratings yet
- TOP 10 Artigos de Clínica Médica - Final PDFDocument14 pagesTOP 10 Artigos de Clínica Médica - Final PDFBruno MeloNo ratings yet
- Terapêutica Diurética e Mecanismos de Resistência Diurética - HFF22MarDocument32 pagesTerapêutica Diurética e Mecanismos de Resistência Diurética - HFF22MarEmerson SchulzeNo ratings yet
- Intoxicação Por MedicamentosDocument2 pagesIntoxicação Por MedicamentosFrederico Gustavo de SouzaNo ratings yet
- A Influência Da Acupuntura e Auriculoterapia Nos Biomarcadores Ureia e CreatininaDocument5 pagesA Influência Da Acupuntura e Auriculoterapia Nos Biomarcadores Ureia e CreatininaHenrique Martins FilhoNo ratings yet
- Ponto de Vista ExistemDocument3 pagesPonto de Vista ExistemGustavo CarraroNo ratings yet
- Avaliacao Nutricional de Pacientes Com DRC (1938)Document12 pagesAvaliacao Nutricional de Pacientes Com DRC (1938)Filipe Taveira LeiteNo ratings yet
- Droga Vasoativa For DummiesDocument11 pagesDroga Vasoativa For DummieswagnabdNo ratings yet
- HAS Na APSDocument39 pagesHAS Na APSlaisa pinNo ratings yet
- Reposição VolêmicaDocument3 pagesReposição VolêmicaPedroPhilippoNo ratings yet
- Atividade de Atenção Farmacêutica.Document4 pagesAtividade de Atenção Farmacêutica.Karina NunesNo ratings yet
- JBN V21n4a05Document13 pagesJBN V21n4a05Eduarda MoraesNo ratings yet
- Exercicios Físicos Durante A HemodiáliseDocument11 pagesExercicios Físicos Durante A HemodiáliseVictor LauneNo ratings yet
- O Papel Da Enfermagem Na Assistência Ao Paciente em Tratamento Hemodialítico PDFDocument7 pagesO Papel Da Enfermagem Na Assistência Ao Paciente em Tratamento Hemodialítico PDFGeizibel CoserNo ratings yet
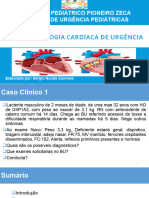
- Patologia Cardíaca de Urgencia. SérgioDocument25 pagesPatologia Cardíaca de Urgencia. Sérgiojorge rubenNo ratings yet
- Estudo de Caso 1Document12 pagesEstudo de Caso 1PaiNNo ratings yet
- Artigo Anestesie Liane Souza PDFDocument8 pagesArtigo Anestesie Liane Souza PDFThomson ChanaNo ratings yet
- DRC e Tto ConservadorDocument8 pagesDRC e Tto ConservadorGislane Sousa OliveiraNo ratings yet
- Healthy Eating and Reduced Risk of Cognitive DecliveDocument10 pagesHealthy Eating and Reduced Risk of Cognitive DecliveHugo Cesar da Silva SalgadoNo ratings yet
- Slide DialiseDocument48 pagesSlide Dialisemariana redivoNo ratings yet
- Sintomas e Complicações Agudas HemodiáliseDocument5 pagesSintomas e Complicações Agudas HemodiáliseAline SantosNo ratings yet
- Cleviprex BulaDocument4 pagesCleviprex BulaNatalia Leguisamo MeirellesNo ratings yet
- Farmacologia Aplicada A Cti Aula 1Document14 pagesFarmacologia Aplicada A Cti Aula 1Karina BarrosNo ratings yet
- Drogas VasoativasDocument30 pagesDrogas VasoativasLívia ChristineNo ratings yet
- Hu2015 en PTDocument7 pagesHu2015 en PTEduardoNo ratings yet
- ConcentradoHemaceas Indicações e Efeitos - En.ptDocument12 pagesConcentradoHemaceas Indicações e Efeitos - En.ptBreno Sousa AguiarNo ratings yet
- 13 Abreviscao Do JejumDocument5 pages13 Abreviscao Do Jejumnicolli munizNo ratings yet
- Conhecimentos e Práticas de Anestesiologistas Sobre Hidratação Perioperatória em PediatriaDocument28 pagesConhecimentos e Práticas de Anestesiologistas Sobre Hidratação Perioperatória em PediatriaPatrick MachadoNo ratings yet
- Roteiro Sobre DVADocument7 pagesRoteiro Sobre DVALarissa VasconcelosNo ratings yet
- Transfer I RDocument7 pagesTransfer I Rkatinhamatos123No ratings yet
- Síndrome Da Abstinência em UTI PediátricaDocument12 pagesSíndrome Da Abstinência em UTI Pediátricajose.neto5731No ratings yet
- FluidTherapyGLS en PTDocument11 pagesFluidTherapyGLS en PTIsabelle PassosNo ratings yet
- Eficacia DieteticaDocument9 pagesEficacia DieteticaMarco Aurélio RodriguesNo ratings yet
- Aula Ajustes Posologia AlunosDocument40 pagesAula Ajustes Posologia AlunosThomazNo ratings yet
- FARMACOLOGIA - QuestõesDocument26 pagesFARMACOLOGIA - QuestõesMariana Barreto Serra0% (1)
- Gouveia 2016Document10 pagesGouveia 2016Thaís MouraNo ratings yet
- 229 1358 1 PBDocument11 pages229 1358 1 PBGabriel AzeredoNo ratings yet
- Efeito Da Drenagem Linfatica Manual Sobre A Glicemia e A Glicose UrinariaDocument6 pagesEfeito Da Drenagem Linfatica Manual Sobre A Glicemia e A Glicose UrinariaGabriele CasonNo ratings yet
- Introdução:: Autor: Co-AutoresDocument3 pagesIntrodução:: Autor: Co-AutoresDimas PiresNo ratings yet
- Terapia Nutricional Na Doença Renal Crônica Transplante Renal - ApostilaDocument29 pagesTerapia Nutricional Na Doença Renal Crônica Transplante Renal - ApostilaLidiane SouzaNo ratings yet
- Aula 10 - Fármacos Anti-HipertensivosDocument40 pagesAula 10 - Fármacos Anti-HipertensivosWilliams MacedoNo ratings yet
- Unoprost 2mg Apsen 30 Capsulas v20Document10 pagesUnoprost 2mg Apsen 30 Capsulas v20Pablo JaborNo ratings yet
- Doenças Renais - Nutricionista Sophia NASF-AB PBH (Presencial)Document53 pagesDoenças Renais - Nutricionista Sophia NASF-AB PBH (Presencial)reinaldo bragança juniorNo ratings yet
- 3 Terapia Nutricional Na Doença Renal Crônica Hemodiálise e DiáliseDocument34 pages3 Terapia Nutricional Na Doença Renal Crônica Hemodiálise e DiáliseThaís VelosoNo ratings yet
- Manual Tecnicas Subs Funcao Renal DEFDocument92 pagesManual Tecnicas Subs Funcao Renal DEFeditwNo ratings yet
- 1 PBDocument13 pages1 PBclovis cechetNo ratings yet
- Aula 3-DiagnósticoDocument28 pagesAula 3-Diagnósticonilza PereiraNo ratings yet
- Avaliação Da Adesão À Dieta DASH Pelo Escore DASH em Paciente Hipertensos: Ensaio Clínico RandomizadoDocument55 pagesAvaliação Da Adesão À Dieta DASH Pelo Escore DASH em Paciente Hipertensos: Ensaio Clínico RandomizadoHipoko RistikoaNo ratings yet
- Rba 70 6 620 Trans1Document7 pagesRba 70 6 620 Trans1rickcosttNo ratings yet
- Pacientes Hipertensos e A Anestesia Na Odontologia PDFDocument7 pagesPacientes Hipertensos e A Anestesia Na Odontologia PDFOsvaldo Muniz CasarimNo ratings yet
- Complicações Nutricionais de Pacientes Com Doença Renal Crônica Submetidos A Hemodiálise: Uma Revisão de LiteraturaDocument3 pagesComplicações Nutricionais de Pacientes Com Doença Renal Crônica Submetidos A Hemodiálise: Uma Revisão de LiteraturaAle AraujoNo ratings yet
- FARA79 Farmacocinética 3Document11 pagesFARA79 Farmacocinética 3HenriqueNo ratings yet
- DIETA DASH PARA INICIANTES: Obtenha uma vida saudável perdendo peso de forma rápida, saudável e equilibrada. Reduzir a pressão arterial, inchaço abdominal e inflamação corporalFrom EverandDIETA DASH PARA INICIANTES: Obtenha uma vida saudável perdendo peso de forma rápida, saudável e equilibrada. Reduzir a pressão arterial, inchaço abdominal e inflamação corporalRating: 4 out of 5 stars4/5 (14)