You might also like
- Eating Disorders in Boys and MenFrom EverandEating Disorders in Boys and MenJason M. NagataNo ratings yet
- Associations of Per Uoroalkyl and Poly Uoroalkyl Substances With Incident Diabetes and Microvascular DiseaseDocument9 pagesAssociations of Per Uoroalkyl and Poly Uoroalkyl Substances With Incident Diabetes and Microvascular Diseasespadini putriNo ratings yet
- Surviving Cancer, COVID-19, and Disease: The Repurposed Drug RevolutionFrom EverandSurviving Cancer, COVID-19, and Disease: The Repurposed Drug RevolutionNo ratings yet
- The Impact of Physical Activity OnDocument7 pagesThe Impact of Physical Activity OnJudith Huarancca MariñoNo ratings yet
- Clinical Precision Medicine: A PrimerFrom EverandClinical Precision Medicine: A PrimerJudy S. CrabtreeNo ratings yet
- RRL3 RLRLDocument18 pagesRRL3 RLRLRowena BayalanNo ratings yet
- Health Care Transition in Young Adults With Type 1 Diabetes: Perspectives of Adult Endocrinologists in The U.SDocument8 pagesHealth Care Transition in Young Adults With Type 1 Diabetes: Perspectives of Adult Endocrinologists in The U.SfransNo ratings yet
- A Randomized, Controlled Trial of Liraglutide For Adolescents With ObesityDocument12 pagesA Randomized, Controlled Trial of Liraglutide For Adolescents With ObesityWarun KumarNo ratings yet
- Dis Arfid PDFDocument10 pagesDis Arfid PDFDalilaNo ratings yet
- Nutrición Hospitalaria: Trabajo OriginalDocument8 pagesNutrición Hospitalaria: Trabajo OriginalSarai OsegueraNo ratings yet
- Evaluating The Quality of Life of Adult Patients oDocument1 pageEvaluating The Quality of Life of Adult Patients opspd anakNo ratings yet
- A Randomized, Controlled Trial of Liraglutide For Adolescents With ObesityDocument12 pagesA Randomized, Controlled Trial of Liraglutide For Adolescents With ObesityJosé Luis ChavesNo ratings yet
- Homa B Homa IrDocument12 pagesHoma B Homa IrMaria Marcella RusliNo ratings yet
- Yogurt Presión ArterialDocument9 pagesYogurt Presión ArterialCarlos MendozaNo ratings yet
- Dieta y CancerDocument11 pagesDieta y CancerJose Angel AbadíaNo ratings yet
- Diabetes-Specific Nutrition Algorithm: A Transcultural Program To Optimize Diabetes and Prediabetes CareDocument15 pagesDiabetes-Specific Nutrition Algorithm: A Transcultural Program To Optimize Diabetes and Prediabetes CareMoechanis HidayatNo ratings yet
- Armodafinil in Binge Eating Disorder A RandomizedDocument7 pagesArmodafinil in Binge Eating Disorder A RandomizedQuel PaivaNo ratings yet
- Antocinaninas Reduzem Risco de DM2 Am J Clin Nutr-2012Document9 pagesAntocinaninas Reduzem Risco de DM2 Am J Clin Nutr-2012Elenice Peltz NutricionistaNo ratings yet
- 10 1002@eat 23236Document12 pages10 1002@eat 23236LucíaNo ratings yet
- Dietary Intake DMDocument9 pagesDietary Intake DMQia BummNo ratings yet
- Health Related Quality of Life and Health Insurance Coverage Among - 2017 - BloDocument3 pagesHealth Related Quality of Life and Health Insurance Coverage Among - 2017 - BloMichael John AguilarNo ratings yet
- ايرانDocument6 pagesايرانsadiq. aljabha.2014No ratings yet
- Nutrition Therapy For Adults With Diabetes or Prediabetes A Consensus Report - 2019 PDFDocument24 pagesNutrition Therapy For Adults With Diabetes or Prediabetes A Consensus Report - 2019 PDFNicolás Di SantoroNo ratings yet
- Polycystic Ovary SyndromeDocument13 pagesPolycystic Ovary SyndromeNAYSHA YANET CHAVEZ RONDINELNo ratings yet
- Advanced Mixed Methods Designs SlidesDocument15 pagesAdvanced Mixed Methods Designs Slideslisa brathwaite grahamNo ratings yet
- Nature NS Genetics Nbiol Tca 2022Document12 pagesNature NS Genetics Nbiol Tca 2022Adriyo00No ratings yet
- Antibiotics As Part of The Management of Severe Acute MalnutritionDocument13 pagesAntibiotics As Part of The Management of Severe Acute Malnutritionmarisa armyNo ratings yet
- Shan. Association of Low-Carbohydrate and Low-Fat Diets With MortalityDocument20 pagesShan. Association of Low-Carbohydrate and Low-Fat Diets With MortalityMaria Julia Ogna EgeaNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive Biology 273 (2022) E1-E62Document1 pageEuropean Journal of Obstetrics & Gynecology and Reproductive Biology 273 (2022) E1-E62LiaNo ratings yet
- Pregnancy-Induced Hypertension and Neonatal Outcomes: A Systematic Review and Meta-AnalysisDocument8 pagesPregnancy-Induced Hypertension and Neonatal Outcomes: A Systematic Review and Meta-AnalysissilvanaNo ratings yet
- Bandini 2010Document6 pagesBandini 2010Monalisa CostaNo ratings yet
- Differentiation of Diabetes by Pathophysiology, Natural History, and Prognosis PDFDocument15 pagesDifferentiation of Diabetes by Pathophysiology, Natural History, and Prognosis PDFHadi PrasetyoNo ratings yet
- Nip Et Al (2019)Document8 pagesNip Et Al (2019)paulabagnaroliNo ratings yet
- Tdah 2Document11 pagesTdah 2Roberto Alexis Molina CampuzanoNo ratings yet
- Articles: BackgroundDocument14 pagesArticles: BackgroundhudaNo ratings yet
- Neonatal Abstinence Syndrome Advances in Diagnosis and TreatmentDocument14 pagesNeonatal Abstinence Syndrome Advances in Diagnosis and TreatmentdzratsoNo ratings yet
- ProteinasDocument9 pagesProteinaspauly 111No ratings yet
- Vitamin D and Telomerase 5Document5 pagesVitamin D and Telomerase 5Muhammad AL Farisi SutrisnoNo ratings yet
- Nip 2019Document8 pagesNip 2019psihologdiabetclujNo ratings yet
- Healthy Diet Reduces Markers of Cardiac Injury and Inflammation Regardless of Macronutrientes Results From de Omniheart TrialDocument19 pagesHealthy Diet Reduces Markers of Cardiac Injury and Inflammation Regardless of Macronutrientes Results From de Omniheart TrialBruno CavicchioNo ratings yet
- Preparing For The NASH Epidemic A Call To ActioDocument11 pagesPreparing For The NASH Epidemic A Call To ActioDaniNo ratings yet
- Homocysteine As A Biomarker For Predicting Disease-Free Survival in Breast Cancer PDFDocument8 pagesHomocysteine As A Biomarker For Predicting Disease-Free Survival in Breast Cancer PDFNelson Carvas JrNo ratings yet
- Wolf Et Al MultivitaminsDocument30 pagesWolf Et Al MultivitaminsAnonymous 2GBzrE3XNo ratings yet
- E20151662 FullDocument11 pagesE20151662 FullMichael OlaleyeNo ratings yet
- Administracion Una Perspectiva Global y Empresarial KoontzDocument11 pagesAdministracion Una Perspectiva Global y Empresarial Koontzandres vallejo cNo ratings yet
- Prospective Study of Major Dietary Patterns and Risk of CoronaryDocument10 pagesProspective Study of Major Dietary Patterns and Risk of CoronaryJohn SammutNo ratings yet
- Ada ModyDocument12 pagesAda ModyMikeyNo ratings yet
- Ni Hms 633733Document15 pagesNi Hms 633733Mirna Liliana Carmona GarciaNo ratings yet
- Food Neophobia Is Related To Factors Associated With Functional Food Consumption in Older AdultsDocument8 pagesFood Neophobia Is Related To Factors Associated With Functional Food Consumption in Older AdultsrodrigoromoNo ratings yet
- Relative Reinforcing Value of FoodDocument11 pagesRelative Reinforcing Value of FoodEnrique AlarconNo ratings yet
- Breakfast Frequency and Development of Metabolic RiskDocument7 pagesBreakfast Frequency and Development of Metabolic Riskpriyanka sharmaNo ratings yet
- ReviewDocument13 pagesReviewNelly ElizabethNo ratings yet
- Leslie Et Al-2018-European Eating Disorders ReviewDocument10 pagesLeslie Et Al-2018-European Eating Disorders ReviewGNo ratings yet
- 303 FullDocument8 pages303 FullpelinNo ratings yet
- The Prevalence, Risk Factors and Clinical Correlates of Obesity in Chinese Patients WithDocument20 pagesThe Prevalence, Risk Factors and Clinical Correlates of Obesity in Chinese Patients WithjhuNo ratings yet
- Clusters Provide A Better Holistic View of Type 2Document1 pageClusters Provide A Better Holistic View of Type 2Ramón Alberto MoroyoquiNo ratings yet
- Fast FoodDocument8 pagesFast Foodkangna_sharma20No ratings yet
- Research Clinical 1 1Document18 pagesResearch Clinical 1 1api-459656816No ratings yet
- Lynch, Et Al ('17) - Sulforaphane From Broccoli Reduces Symptoms of Autism - A Follow-Up Case Series From A Randomized Double-Blind Study (GAHM) PDFDocument7 pagesLynch, Et Al ('17) - Sulforaphane From Broccoli Reduces Symptoms of Autism - A Follow-Up Case Series From A Randomized Double-Blind Study (GAHM) PDFaida-69No ratings yet
- Kuczmarski 2010Document7 pagesKuczmarski 2010Alejandra LópezNo ratings yet
- 2021 Fibroid Uterus Surgical Challenges inDocument200 pages2021 Fibroid Uterus Surgical Challenges inHAVIZ YUADNo ratings yet
- MCU 2021 Uterine Fibroids 1st EditionDocument165 pagesMCU 2021 Uterine Fibroids 1st EditionHAVIZ YUADNo ratings yet
- 2021 Clinical Practice Guidelines On The Diagnosis and Management of Polycystic OvaryDocument11 pages2021 Clinical Practice Guidelines On The Diagnosis and Management of Polycystic OvarySalma Yuri KhairunnisaNo ratings yet
- Genetic Construction Between Polycystic Ovarian SyndromeDocument5 pagesGenetic Construction Between Polycystic Ovarian SyndromeHAVIZ YUADNo ratings yet
- Weight Management in Adolescents With Polycystic Ovary SyndromeDocument11 pagesWeight Management in Adolescents With Polycystic Ovary SyndromeHAVIZ YUADNo ratings yet
- MCU 2019 Essentials in Gynecology For Undergraduate Medical StudentsDocument414 pagesMCU 2019 Essentials in Gynecology For Undergraduate Medical StudentsHAVIZ YUAD100% (1)
- Vaginal Microbiota Transplantation:: The Next FrontierDocument13 pagesVaginal Microbiota Transplantation:: The Next FrontierHAVIZ YUADNo ratings yet
- MCU 2018 Workbook For Diagnostic Medical Sonography A Guide To ClinicalDocument496 pagesMCU 2018 Workbook For Diagnostic Medical Sonography A Guide To ClinicalHAVIZ YUADNo ratings yet
- Paulson 2020 Add-Ons Seminar PGTA IntroDocument18 pagesPaulson 2020 Add-Ons Seminar PGTA IntroHAVIZ YUADNo ratings yet
- The Role of Gut and Genital Microbiota and The Estrobolome in Endometriosis, Infertility and Chronic Pelvic PainDocument40 pagesThe Role of Gut and Genital Microbiota and The Estrobolome in Endometriosis, Infertility and Chronic Pelvic PainsefzanimeriaNo ratings yet
- Weight Management in Adolescents With Polycystic Ovary SyndromeDocument11 pagesWeight Management in Adolescents With Polycystic Ovary SyndromeHAVIZ YUADNo ratings yet
- Andropause Current ConceptsDocument9 pagesAndropause Current ConceptsHAVIZ YUADNo ratings yet
- Fcimb 12 1069557Document8 pagesFcimb 12 1069557HAVIZ YUADNo ratings yet
- Acog Committee Opinion: Infertility Workup For The Women 'S Health SpecialistDocument8 pagesAcog Committee Opinion: Infertility Workup For The Women 'S Health SpecialistLissa SabrinaNo ratings yet
- Molecular Detection of Microbial Colonization in Cervical MucusDocument9 pagesMolecular Detection of Microbial Colonization in Cervical MucusHAVIZ YUADNo ratings yet
- Detection of The Selective Androgen Receptor Modulator GSK2881078 andDocument16 pagesDetection of The Selective Androgen Receptor Modulator GSK2881078 andHAVIZ YUADNo ratings yet
- Role of Anti-Müllerian Hormone in The Pathogenesis of Polycystic Ovary SyndromeDocument9 pagesRole of Anti-Müllerian Hormone in The Pathogenesis of Polycystic Ovary SyndromeHAVIZ YUADNo ratings yet
- Pcos May Be AutoimmunDocument9 pagesPcos May Be AutoimmunHAVIZ YUADNo ratings yet
- Androgen Receptor Gene Mutations in 258 Han ChineseDocument8 pagesAndrogen Receptor Gene Mutations in 258 Han ChineseHAVIZ YUADNo ratings yet
- Ijerph 18 10074Document20 pagesIjerph 18 10074HAVIZ YUADNo ratings yet
- Double StimulationDocument13 pagesDouble StimulationHAVIZ YUADNo ratings yet
- Raja EA-2022Document12 pagesRaja EA-2022HAVIZ YUADNo ratings yet
- Genetic Basis of Polycystic Ovary Syndrome (PCOS)Document12 pagesGenetic Basis of Polycystic Ovary Syndrome (PCOS)HAVIZ YUADNo ratings yet
- The Metabolic Syndrome in Polycystic Ovary SyndromeDocument21 pagesThe Metabolic Syndrome in Polycystic Ovary SyndromeHAVIZ YUADNo ratings yet
- What Is The Best Regimen For Ovarian Stimulation of Poor Responders in ARTIVFDocument10 pagesWhat Is The Best Regimen For Ovarian Stimulation of Poor Responders in ARTIVFHAVIZ YUADNo ratings yet
- The Metabolic Syndrome in Polycystic Ovary SyndromeDocument21 pagesThe Metabolic Syndrome in Polycystic Ovary SyndromeHAVIZ YUADNo ratings yet
- Androgen Receptor Splice Variants and PolycysticDocument2 pagesAndrogen Receptor Splice Variants and PolycysticHAVIZ YUADNo ratings yet
- Androgen Receptor Gene Polymorphism and Polycystic Ovary SyndromeDocument4 pagesAndrogen Receptor Gene Polymorphism and Polycystic Ovary SyndromeHAVIZ YUADNo ratings yet
- What Is The Best Regimen For Ovarian Stimulation of Poor Responders in ARTIVFDocument10 pagesWhat Is The Best Regimen For Ovarian Stimulation of Poor Responders in ARTIVFHAVIZ YUADNo ratings yet
- Insulin Guidelines For Type2 DiabetesDocument6 pagesInsulin Guidelines For Type2 DiabetestcsariNo ratings yet
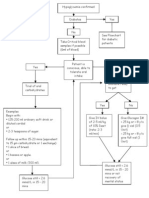
- Hypoglycaemia FlowchartDocument1 pageHypoglycaemia FlowchartMohammad SultanNo ratings yet
- Nutra Puding Buah NagaDocument2 pagesNutra Puding Buah NagaUun RochmawatiNo ratings yet
- AF (CHADSVASC-HASbled)Document1 pageAF (CHADSVASC-HASbled)Giorgi NanetashviliNo ratings yet
- What Is A Blood Glucose TestDocument8 pagesWhat Is A Blood Glucose TestRatnaPrasadNalamNo ratings yet
- Diabetes ManagementDocument11 pagesDiabetes ManagementNirav SharmaNo ratings yet
- Anik Widijanti: Clinical Pathology Department Saiful Anwar Hospital / Medical Faculty Brawijaya University MALANGDocument40 pagesAnik Widijanti: Clinical Pathology Department Saiful Anwar Hospital / Medical Faculty Brawijaya University MALANGTutde SedanaNo ratings yet
- Bayer Contour GlucometruDocument25 pagesBayer Contour Glucometruantic2007No ratings yet
- Quantifying The Health Economic Value AsDocument1 pageQuantifying The Health Economic Value AsMatiasNo ratings yet
- 17-Article Text-72-1-10-20191213Document8 pages17-Article Text-72-1-10-20191213Zahratul HayatiNo ratings yet
- Classification of DiabetesDocument94 pagesClassification of DiabetesTHAO DANGNo ratings yet
- REFRENSCESDocument3 pagesREFRENSCESArief AndriyantoNo ratings yet
- HbA1C, RBS AND FBS DATADocument2 pagesHbA1C, RBS AND FBS DATASamwel GachokaNo ratings yet
- ZP194021 PDFDocument1 pageZP194021 PDFNeel VermaNo ratings yet
- Diabeties in PregnancyDocument15 pagesDiabeties in PregnancyBhawna JoshiNo ratings yet
- Carbohydrates - Part - 2 - MazenDocument28 pagesCarbohydrates - Part - 2 - MazenAhmed GaberNo ratings yet
- Oral Diabetic MedicationDocument26 pagesOral Diabetic MedicationTaimoor BaigNo ratings yet
- 2 June 2023Document5 pages2 June 2023harronNo ratings yet
- The Role of Insulin in Maintaining Blood Glucose HomeostasisDocument2 pagesThe Role of Insulin in Maintaining Blood Glucose HomeostasisyaniqueNo ratings yet
- A Case Presentation On Diabetic KetoacidosisDocument13 pagesA Case Presentation On Diabetic Ketoacidosisrenie3245No ratings yet
- Jurnal PKMDocument12 pagesJurnal PKMfidyaangraeni 61No ratings yet
- Insulin ManagementDocument38 pagesInsulin ManagementMelinda Rose FernandezNo ratings yet
- User Guide: Blood Glucose Monitoring SystemDocument30 pagesUser Guide: Blood Glucose Monitoring SystemVince CentenoNo ratings yet
- DC 221622Document6 pagesDC 221622juanraNo ratings yet
- Diabetes 2023Document15 pagesDiabetes 2023Hira ijazNo ratings yet
- DM Pamphlet FinalDocument3 pagesDM Pamphlet FinalLouresa Mae TNo ratings yet
- ADA Management Patients DKA UpToDate AlgoritmoDocument3 pagesADA Management Patients DKA UpToDate AlgoritmoEMELYN YASMIN FIGUEROA HUANCANo ratings yet
- Task 9 Glucose EstimationDocument2 pagesTask 9 Glucose EstimationJhenard John Lansangan BeltranNo ratings yet
- Risk For Unstable Blood Glucose (DM)Document4 pagesRisk For Unstable Blood Glucose (DM)Ace Khiel Peralta50% (2)
- Ijcmr 3211 v1 PDFDocument5 pagesIjcmr 3211 v1 PDFAtul DwivediNo ratings yet
- Boundless: Upgrade Your Brain, Optimize Your Body & Defy AgingFrom EverandBoundless: Upgrade Your Brain, Optimize Your Body & Defy AgingRating: 4.5 out of 5 stars4.5/5 (66)
- Relentless: From Good to Great to UnstoppableFrom EverandRelentless: From Good to Great to UnstoppableRating: 5 out of 5 stars5/5 (783)
- Weight Lifting Is a Waste of Time: So Is Cardio, and There’s a Better Way to Have the Body You WantFrom EverandWeight Lifting Is a Waste of Time: So Is Cardio, and There’s a Better Way to Have the Body You WantRating: 4.5 out of 5 stars4.5/5 (38)
- Peak: The New Science of Athletic Performance That is Revolutionizing SportsFrom EverandPeak: The New Science of Athletic Performance That is Revolutionizing SportsRating: 5 out of 5 stars5/5 (96)
- Muscle for Life: Get Lean, Strong, and Healthy at Any Age!From EverandMuscle for Life: Get Lean, Strong, and Healthy at Any Age!Rating: 4.5 out of 5 stars4.5/5 (22)
- Power of 10: The Once-A-Week Slow Motion Fitness RevolutionFrom EverandPower of 10: The Once-A-Week Slow Motion Fitness RevolutionRating: 3.5 out of 5 stars3.5/5 (11)
- Aging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayFrom EverandAging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayNo ratings yet
- Chair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouFrom EverandChair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouRating: 3.5 out of 5 stars3.5/5 (5)
- Functional Training and Beyond: Building the Ultimate Superfunctional Body and MindFrom EverandFunctional Training and Beyond: Building the Ultimate Superfunctional Body and MindRating: 4.5 out of 5 stars4.5/5 (1)
- Music For Healing: With Nature Sounds For Natural Healing Powers: Sounds Of Nature, Deep Sleep Music, Meditation, Relaxation, Healing MusicFrom EverandMusic For Healing: With Nature Sounds For Natural Healing Powers: Sounds Of Nature, Deep Sleep Music, Meditation, Relaxation, Healing MusicRating: 5 out of 5 stars5/5 (1)
- Strong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerFrom EverandStrong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerRating: 4 out of 5 stars4/5 (5)
- Wall Pilates: Quick-and-Simple to Lose Weight and Stay Healthy. A 30-Day Journey with + 100 ExercisesFrom EverandWall Pilates: Quick-and-Simple to Lose Weight and Stay Healthy. A 30-Day Journey with + 100 ExercisesNo ratings yet
- Yamas & Niyamas: Exploring Yoga's Ethical PracticeFrom EverandYamas & Niyamas: Exploring Yoga's Ethical PracticeRating: 4.5 out of 5 stars4.5/5 (111)
- The Yogi Code: Seven Universal Laws of Infinite SuccessFrom EverandThe Yogi Code: Seven Universal Laws of Infinite SuccessRating: 4.5 out of 5 stars4.5/5 (104)
- Whole Body Barefoot: Transitioning Well to Minimal FootwearFrom EverandWhole Body Barefoot: Transitioning Well to Minimal FootwearRating: 4 out of 5 stars4/5 (16)
- SAS Training Manual: How to get fit enough to pass a special forces selection courseFrom EverandSAS Training Manual: How to get fit enough to pass a special forces selection courseRating: 4 out of 5 stars4/5 (3)
- Roxane Gay & Everand Originals: Built for This: The Quiet Strength of PowerliftingFrom EverandRoxane Gay & Everand Originals: Built for This: The Quiet Strength of PowerliftingRating: 4.5 out of 5 stars4.5/5 (132)
- Body by Science: A Research Based Program for Strength Training, Body building, and Complete Fitness in 12 Minutes a WeekFrom EverandBody by Science: A Research Based Program for Strength Training, Body building, and Complete Fitness in 12 Minutes a WeekRating: 4.5 out of 5 stars4.5/5 (84)
- Endure: Mind, Body, and the Curiously Elastic Limits of Human PerformanceFrom EverandEndure: Mind, Body, and the Curiously Elastic Limits of Human PerformanceRating: 4.5 out of 5 stars4.5/5 (237)
- The Power of Now by Eckhart Tolle: Summary and AnalysisFrom EverandThe Power of Now by Eckhart Tolle: Summary and AnalysisRating: 4.5 out of 5 stars4.5/5 (12)
- How To Walk Yourself Healthy And Happy: Discover the physical and mental benefits of regular walking.From EverandHow To Walk Yourself Healthy And Happy: Discover the physical and mental benefits of regular walking.Rating: 4.5 out of 5 stars4.5/5 (11)
- Not a Diet Book: Take Control. Gain Confidence. Change Your Life.From EverandNot a Diet Book: Take Control. Gain Confidence. Change Your Life.Rating: 4.5 out of 5 stars4.5/5 (124)
- You: Breathing Easy: Meditation and Breathing Techniques to Relax, Refresh and RevitalizeFrom EverandYou: Breathing Easy: Meditation and Breathing Techniques to Relax, Refresh and RevitalizeRating: 3 out of 5 stars3/5 (5)
- Body by Science: A Research Based Program to Get the Results You Want in 12 Minutes a WeekFrom EverandBody by Science: A Research Based Program to Get the Results You Want in 12 Minutes a WeekRating: 4 out of 5 stars4/5 (38)