You might also like
- Oral Medicine & Pathology from A-ZFrom EverandOral Medicine & Pathology from A-ZRating: 5 out of 5 stars5/5 (9)
- The Dental Pulp: Biology, Pathology, and Regenerative TherapiesFrom EverandThe Dental Pulp: Biology, Pathology, and Regenerative TherapiesNo ratings yet
- Cyst of The JawsDocument13 pagesCyst of The Jawstthtn6c8pbNo ratings yet
- Cyst Final-1Document120 pagesCyst Final-1drjatinNo ratings yet
- Odontogenic and Non Odontogenic Cysts of The Oral CavityDocument115 pagesOdontogenic and Non Odontogenic Cysts of The Oral CavitySalwa AboelmagdNo ratings yet
- Odontogenic Cysts and TumorsDocument273 pagesOdontogenic Cysts and TumorsAliImadAlKhasaki82% (11)
- Odontogenic Cysts of The JAW: Seminar Presented byDocument31 pagesOdontogenic Cysts of The JAW: Seminar Presented byankita sethi100% (1)
- BDS10011 Cystic Lesions of Bone 2Document50 pagesBDS10011 Cystic Lesions of Bone 2habibahafez282No ratings yet
- Introduction Cysts of JawsDocument62 pagesIntroduction Cysts of JawsFatima Siddiqui100% (1)
- Introduction Cysts of JawsDocument62 pagesIntroduction Cysts of JawsEnass Alhadi50% (2)
- Oral & Maxillofacial Cysts GuideDocument43 pagesOral & Maxillofacial Cysts GuidemohmedNo ratings yet
- CYST - نسخةDocument71 pagesCYST - نسخةKHALED WALEEDNo ratings yet
- Cysts of The JawDocument7 pagesCysts of The Jawfadfadfad0No ratings yet
- Seminar On Radicular CystDocument7 pagesSeminar On Radicular CystKhalid Mahmud Arifin100% (2)
- Cysts of Odontogenic OriginDocument82 pagesCysts of Odontogenic OriginNamitha Mysore Hiriyanna100% (3)
- 3,3 - Cyst of Jaws and Oral Soft TissuesDocument19 pages3,3 - Cyst of Jaws and Oral Soft Tissuesحمزة تلاحمةNo ratings yet
- د.نجاة Cyst-7 (Muhadharaty) 1Document28 pagesد.نجاة Cyst-7 (Muhadharaty) 1بكر الدوريNo ratings yet
- Odontogenic Cysts of the Jaws: Classification, Clinical Features and TreatmentDocument63 pagesOdontogenic Cysts of the Jaws: Classification, Clinical Features and TreatmentFaraz MohammedNo ratings yet
- Odontogenic Cyst and Non Odontogenic CystDocument67 pagesOdontogenic Cyst and Non Odontogenic CystLuthfieHaq0% (1)
- Multiple Radiolucent or Mixed RadiolucentDocument17 pagesMultiple Radiolucent or Mixed RadiolucentMohamd ElbatannoyNo ratings yet
- Cysts of The JawDocument14 pagesCysts of The Jawluke swanepoelNo ratings yet
- Oral Mucosa CystsDocument180 pagesOral Mucosa CystsDinesh YadavNo ratings yet
- Odontogenic CystsDocument54 pagesOdontogenic CystssamsoomaustNo ratings yet
- CystDocument120 pagesCystAbood SamoudiNo ratings yet
- Odontogenic CystsDocument63 pagesOdontogenic CystsshabeelpnNo ratings yet
- Oral Pathology: Non-Epithelialized Primary Bone CystDocument4 pagesOral Pathology: Non-Epithelialized Primary Bone Cystعلي صادق جعفرNo ratings yet
- The Pathogenesis of Odontogenic Cysts: A ReviewDocument17 pagesThe Pathogenesis of Odontogenic Cysts: A ReviewClaudia AngNo ratings yet
- Cysts MainDocument43 pagesCysts MainharshiniNo ratings yet
- Radiographic features and treatment of periapical cystDocument40 pagesRadiographic features and treatment of periapical cystLojin HaddadNo ratings yet
- Cysts MainDocument43 pagesCysts MainharshiniNo ratings yet
- Cysts of The Oral Cavity-3Document33 pagesCysts of The Oral Cavity-3Mostafa El GendyNo ratings yet
- Odontogenic Cysts GuideDocument5 pagesOdontogenic Cysts GuideBH ASMRNo ratings yet
- ORAL RADIOLOGY SEMINAR CYSTS OF THE JAWDocument60 pagesORAL RADIOLOGY SEMINAR CYSTS OF THE JAWafzanwahab100% (1)
- Cysts of The JawsDocument75 pagesCysts of The JawsSwetha KaripineniNo ratings yet
- Review Article: Bone Diseases of The JawsDocument7 pagesReview Article: Bone Diseases of The Jawsh20pologtNo ratings yet
- Odontogenic Keratocyst: - Jayalakshmi Preetha Meyyanathan CRIDocument48 pagesOdontogenic Keratocyst: - Jayalakshmi Preetha Meyyanathan CRIJayalakshmi PreethaNo ratings yet
- Cysts of Maxillofacial Region: Presnter: Dr. Siyum M. (Omfs-Rii) Moderator: Dr. Jorge (Omfs Consultant)Document115 pagesCysts of Maxillofacial Region: Presnter: Dr. Siyum M. (Omfs-Rii) Moderator: Dr. Jorge (Omfs Consultant)Siyum MathewosNo ratings yet
- l17 Management of CystsDocument55 pagesl17 Management of CystsJu JuNo ratings yet
- Fissural CystsDocument17 pagesFissural CystssailalithaNo ratings yet
- Cysts of the Jaws Treatment GuideDocument24 pagesCysts of the Jaws Treatment GuidedoctorniravNo ratings yet
- Cysts of The Oral CavityDocument270 pagesCysts of The Oral CavitySally Mahfouz100% (6)
- Odontogenic CystsDocument106 pagesOdontogenic Cystsريام الموسويNo ratings yet
- Cyst Theory ClassDocument310 pagesCyst Theory ClasswakoNo ratings yet
- CystDocument59 pagesCystHarshini DonepudiNo ratings yet
- Oral Cavity Cysts: Types, Causes and TreatmentsDocument65 pagesOral Cavity Cysts: Types, Causes and TreatmentsDr. Hasna ArshadNo ratings yet
- Odontogenic Tumor Ameloblastoma: Presented By: Ankita Singh Bds Final Year Roll No 37Document73 pagesOdontogenic Tumor Ameloblastoma: Presented By: Ankita Singh Bds Final Year Roll No 37ankita sethiNo ratings yet
- Summary For Cysts of JawsDocument10 pagesSummary For Cysts of JawsVihang Naphade100% (2)
- Odontogenic Cysts and Tumor of The JawsDocument149 pagesOdontogenic Cysts and Tumor of The JawsAnooda MazenNo ratings yet
- Cysts - DR SpoorthiDocument206 pagesCysts - DR Spoorthiohc sem8No ratings yet
- Differential Diagnosis of Pericoronal RadiolucenciesDocument30 pagesDifferential Diagnosis of Pericoronal RadiolucenciesakNo ratings yet
- Orofacial CystsDocument84 pagesOrofacial CystsWorku KifleNo ratings yet
- William L. Chung Kurt Summersgill Mark Ochs: OdontogenicDocument18 pagesWilliam L. Chung Kurt Summersgill Mark Ochs: OdontogenicyosephineninaNo ratings yet
- 3-Cysts of JawsDocument61 pages3-Cysts of JawsMedo AshrafNo ratings yet
- Cysts of The JawsDocument28 pagesCysts of The JawsMladen PazinNo ratings yet
- Radicular Cyst Guide: Causes, Symptoms & TreatmentDocument45 pagesRadicular Cyst Guide: Causes, Symptoms & TreatmentPriyanka GanesanNo ratings yet
- Odontogenic Keratocyst (Keratocystic Odontogenic Tumor, WHO 2005)Document10 pagesOdontogenic Keratocyst (Keratocystic Odontogenic Tumor, WHO 2005)Atef Mahmoud AhmedNo ratings yet
- Klasifikasi KistaDocument31 pagesKlasifikasi KistaIbnuNo ratings yet
- Complications in UveitisFrom EverandComplications in UveitisFrancesco PichiNo ratings yet
- 1-Pain 1Document30 pages1-Pain 1Sadek MohamedNo ratings yet
- Colour Science and Shade Selection For PDFDocument75 pagesColour Science and Shade Selection For PDFSadek MohamedNo ratings yet
- Level 1,2,3 Dentistry-Spring 2024 Timetable-RamadanDocument14 pagesLevel 1,2,3 Dentistry-Spring 2024 Timetable-RamadanSadek MohamedNo ratings yet
- 4 5809670530357265615 PDFDocument420 pages4 5809670530357265615 PDFOmar SiddigNo ratings yet
- Abnormal Female Puberty 2016Document281 pagesAbnormal Female Puberty 2016MustafaAwaad100% (1)
- C Difficile SporesDocument3 pagesC Difficile SporesEda SopNo ratings yet
- Unit 10Document7 pagesUnit 10Minh Đức NghiêmNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakaYuli ErmaNo ratings yet
- Step 1 Checklist for Biochemistry, Genetics and DevelopmentDocument11 pagesStep 1 Checklist for Biochemistry, Genetics and DevelopmentHasan Khan RoudbaryNo ratings yet
- 2018-09-01 Men's Fitness UK PDFDocument116 pages2018-09-01 Men's Fitness UK PDFsalik salmanNo ratings yet
- Vomiting in ChildrenDocument41 pagesVomiting in ChildrenWiresa RenaltaNo ratings yet
- Conscious Sedation Guidelines for DentistsDocument18 pagesConscious Sedation Guidelines for DentistsAnna NgNo ratings yet
- CoronarografieDocument72 pagesCoronarografieLaurentiu AndreiNo ratings yet
- Insulin MinDocument23 pagesInsulin MinLukasNo ratings yet
- Principles of GeneticsDocument161 pagesPrinciples of GeneticsSomeone100% (3)
- Intl Journal of Cancer - 2014 - Lakritz - Beneficial Bacteria Stimulate Host Immune Cells To Counteract Dietary and GeneticDocument12 pagesIntl Journal of Cancer - 2014 - Lakritz - Beneficial Bacteria Stimulate Host Immune Cells To Counteract Dietary and GeneticTrang MốcNo ratings yet
- Segamat District Muet Final Year Lower 6 Exam-Govin2Document20 pagesSegamat District Muet Final Year Lower 6 Exam-Govin2govinjementah100% (1)
- Bacteria - Definition, Shapes, Characteristics, Types & ExamplesDocument2 pagesBacteria - Definition, Shapes, Characteristics, Types & ExamplesBaikuntha SabarNo ratings yet
- Analysis of Survival Data - LN - D Zhang - 05Document264 pagesAnalysis of Survival Data - LN - D Zhang - 05mirceacomanro2740100% (1)
- Antihistamine: I. HistoryDocument6 pagesAntihistamine: I. HistoryAnaliza Kitongan LantayanNo ratings yet
- IeltsDocument65 pagesIeltskitten_alina92% (13)
- Genital ProlapseDocument20 pagesGenital ProlapseMehreen MaqboolNo ratings yet
- MLS & IMT Reading List 3-13Document2 pagesMLS & IMT Reading List 3-13Joseph SabidoNo ratings yet
- AAO - External Disease and CorneaDocument19 pagesAAO - External Disease and CorneaJohn Paul VillaflorNo ratings yet
- Diverticular DiseaseDocument15 pagesDiverticular DiseaseRogie SaludoNo ratings yet
- Mrunal Emotional Intelligence:Meaning, Benefits, Models, Case StudiesDocument8 pagesMrunal Emotional Intelligence:Meaning, Benefits, Models, Case StudiesPrateek BayalNo ratings yet
- Uterin InversionDocument8 pagesUterin InversionZahra AlSaif100% (1)
- Liu2011 PDFDocument6 pagesLiu2011 PDFAnonymous cUzAJWocPCNo ratings yet
- Group 8Document14 pagesGroup 8HrishavNo ratings yet
- Maintaining Homeostasis: The Coordinated Functions of the Nervous and Endocrine SystemsDocument15 pagesMaintaining Homeostasis: The Coordinated Functions of the Nervous and Endocrine SystemsZahra Alexä DavidsonNo ratings yet
- Vital SignsDocument2 pagesVital SignsstaciadokNo ratings yet
- Illustrated Synopsis of Dermatology and Sexually Transmitted DiseasesDocument1 pageIllustrated Synopsis of Dermatology and Sexually Transmitted DiseasesManoj PavanNo ratings yet
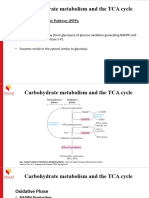
- Carbohydrate Metabolism TCA Cycle - (PPP and Glycogen Metabolism)Document17 pagesCarbohydrate Metabolism TCA Cycle - (PPP and Glycogen Metabolism)Frolian MichaelNo ratings yet
- THE ANTIFUNGAL PROPERTY OF RADISH EXTRACT (RaphanusDocument35 pagesTHE ANTIFUNGAL PROPERTY OF RADISH EXTRACT (RaphanusJaroq Aljon HipolitoNo ratings yet