You might also like
- Child TCLDocument28 pagesChild TCLNandie JoyNo ratings yet
- ChildDocument17 pagesChildReyna Glorian HilarioNo ratings yet
- Child TCLDocument12 pagesChild TCLlaliejhessNo ratings yet
- TCL BHS 14Document38 pagesTCL BHS 14maroseg21No ratings yet
- Immunization Outreach Form 2023Document1 pageImmunization Outreach Form 2023Ignatius KashumeNo ratings yet
- Target Client List For Nutrition and Expanded Program For ImmunizationDocument7 pagesTarget Client List For Nutrition and Expanded Program For ImmunizationEden Vblagasy0% (1)
- Immunization & Child Follow-UpDocument1 pageImmunization & Child Follow-UpRoseNo ratings yet
- Maternal Care and ServicesDocument35 pagesMaternal Care and ServicesAaron ConstantinoNo ratings yet
- NICU Register - A3 29008Document5 pagesNICU Register - A3 29008MesfinNo ratings yet
- 21Document12 pages21Dr-Sanjay SinghaniaNo ratings yet
- FHSIS Form TCL Pre NatalDocument11 pagesFHSIS Form TCL Pre NatalEden Vblagasy100% (5)
- For 20 Weeks AOG and AboveDocument6 pagesFor 20 Weeks AOG and AboveShannen AndradeNo ratings yet
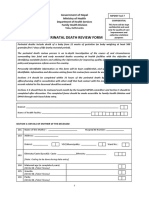
- Form Kematian Bayi & A BLTDocument6 pagesForm Kematian Bayi & A BLTpuskesmasNo ratings yet
- C-MAMI Enrolment and Management CardDocument3 pagesC-MAMI Enrolment and Management CardAbebe TilahunNo ratings yet
- Indicators Calculation Formula Achieveme NT Weightag e Acheieved Score (Out of 100)Document8 pagesIndicators Calculation Formula Achieveme NT Weightag e Acheieved Score (Out of 100)Mahadeb MukhopadhyayNo ratings yet
- Annexure 1.3: Reporting Format For Newborn Facility: Section A To Be Filled From Labor Room & OT Records (As Applicable)Document6 pagesAnnexure 1.3: Reporting Format For Newborn Facility: Section A To Be Filled From Labor Room & OT Records (As Applicable)Nodal Officer NHM AAAGHNo ratings yet
- India EPI Factsheet 2023Document6 pagesIndia EPI Factsheet 2023Chetan SharmaNo ratings yet
- Overview, OB Scoring, AOG, and EDDDocument1 pageOverview, OB Scoring, AOG, and EDDelmer.platiljrNo ratings yet
- Handout PrenatalDocument5 pagesHandout PrenatalCiella Dela Cruz100% (2)
- NCM 209 Lec - TransesDocument122 pagesNCM 209 Lec - TransesAlianna RoseeNo ratings yet
- Mncah Presentation (For Jan-April-7Document30 pagesMncah Presentation (For Jan-April-7lunyolo oliverNo ratings yet
- DR Skills LabDocument14 pagesDR Skills LabHameda MangulamasNo ratings yet
- Table 2: Summary of WHO Position Papers - Recommended Routine Immunizations For ChildrenDocument11 pagesTable 2: Summary of WHO Position Papers - Recommended Routine Immunizations For ChildrenNehaNo ratings yet
- 1-Introduction To NeonatologyDocument7 pages1-Introduction To NeonatologyMhmNo ratings yet
- FNCPDocument5 pagesFNCPCarina QuibinitNo ratings yet
- Immunization Scedule WhoDocument1 pageImmunization Scedule Whokg7976No ratings yet
- History TakingDocument3 pagesHistory Takingmkct111100% (1)
- Immunization Routine Table2Document11 pagesImmunization Routine Table2Rafika IkaNo ratings yet
- OB Notes 101 2Document1 pageOB Notes 101 2rose.petalsssrme01No ratings yet
- FP TCLDocument2 pagesFP TCLlaliejhessNo ratings yet
- Tool For Data CollectionDocument5 pagesTool For Data CollectionAbishaNo ratings yet
- SC 96032864Document8 pagesSC 96032864Anonymous TESWhmTgNo ratings yet
- SC 96032864Document8 pagesSC 96032864Anonymous TESWhmTgNo ratings yet
- OG Notes EditedDocument10 pagesOG Notes EditedAnonymous w4lLoMd7No ratings yet
- Revised CSSM Monthly Reporting Format For ANMsDocument3 pagesRevised CSSM Monthly Reporting Format For ANMsphc kallumarri0% (1)
- Routine Immunization Schedule For InfantsDocument2 pagesRoutine Immunization Schedule For InfantsShing Mae MarieNo ratings yet
- 7 Tools Hospital PDR FormDocument5 pages7 Tools Hospital PDR FormprabeshNo ratings yet
- Ban Epi Factsheet 2020 EngDocument6 pagesBan Epi Factsheet 2020 EngAL HayatNo ratings yet
- Maternal Rle ReviewerDocument4 pagesMaternal Rle ReviewerPrincess Dela CruzNo ratings yet
- Expanded Program of Immunization (Source: DOH)Document12 pagesExpanded Program of Immunization (Source: DOH)Jefferson Dungca94% (35)
- Paediatrics Case History Format by S.P.Kamthankar PDFDocument10 pagesPaediatrics Case History Format by S.P.Kamthankar PDFManisha PatelNo ratings yet
- OB 1.01 Philippine Obstetrics and Anatomy of The Female Reproductive SystemDocument8 pagesOB 1.01 Philippine Obstetrics and Anatomy of The Female Reproductive SystemCandice SongcoNo ratings yet
- Enhanced Surveillance FormDocument2 pagesEnhanced Surveillance FormhelfiNo ratings yet
- Expanded Program On Immunization With Pics - RHUBY ABENOJADocument8 pagesExpanded Program On Immunization With Pics - RHUBY ABENOJARHUBY ABENOJANo ratings yet
- SicckKids - PRD - 070 - EFGH - Neyama AlladinDocument1 pageSicckKids - PRD - 070 - EFGH - Neyama AlladinNeyama AlladinNo ratings yet
- Notification of Vaccination Letter Template: Vaccines AdministeredDocument1 pageNotification of Vaccination Letter Template: Vaccines AdministeredJacob BuckNo ratings yet
- Kindergarten UsirDocument2 pagesKindergarten UsirsoloskojNo ratings yet
- NBZ Qobgy V01 092020Document3 pagesNBZ Qobgy V01 092020chong xue erNo ratings yet
- Part 2Document15 pagesPart 2Rod Reynon BorceNo ratings yet
- Who Immunization-Routine-Table2Document11 pagesWho Immunization-Routine-Table2Frances Jean T. DoblasNo ratings yet
- BCCDC Adult Record CardDocument2 pagesBCCDC Adult Record CardYoj SaraNo ratings yet
- 8 PEDIA Dr. Gallardo Pediatric Immunizations April 7Document7 pages8 PEDIA Dr. Gallardo Pediatric Immunizations April 7qsd clinicNo ratings yet
- Attending Gynaecologist's StatementDocument3 pagesAttending Gynaecologist's Statementaiqianlim97No ratings yet
- Laporan Dashboard Poned JUNI NoviaDocument1 pageLaporan Dashboard Poned JUNI Noviaastri syadiahNo ratings yet
- Route and Site of Administration: Age of The ChildDocument2 pagesRoute and Site of Administration: Age of The ChildJoshua VillarbaNo ratings yet
- Camca Prelim Reviewer 2Document11 pagesCamca Prelim Reviewer 2Danna MedranaNo ratings yet
- Obstetrics - 3rd EdDocument102 pagesObstetrics - 3rd EdAbdelazizSeliemNo ratings yet
- VaccinesDocument2 pagesVaccinesMa. Christina Jane OmambacNo ratings yet
- 7 Postpartum CareDocument20 pages7 Postpartum CareVirgie GigiNo ratings yet
- KELOMPOK 2 - Psikologi Dalam Praktik Kebidanan - Referensi Makalah - B1 - S1 KebidananDocument102 pagesKELOMPOK 2 - Psikologi Dalam Praktik Kebidanan - Referensi Makalah - B1 - S1 KebidananAsyifa SetiawanNo ratings yet
- Backgrounder Pearl Gamblers Experience at Misericordia Community Hospital in EdmontonDocument2 pagesBackgrounder Pearl Gamblers Experience at Misericordia Community Hospital in EdmontonCityNewsTorontoNo ratings yet
- Mick Final ppt-1Document8 pagesMick Final ppt-1SAMMYNo ratings yet
- The Effect of A Training Program During Pregnancy On The Attitude and Intention of NulliparousDocument8 pagesThe Effect of A Training Program During Pregnancy On The Attitude and Intention of NulliparousNoraNo ratings yet
- Adorio Partograph ScenarioDocument2 pagesAdorio Partograph Scenariojonathan liboonNo ratings yet
- Discharge PlanDocument5 pagesDischarge PlanYoshimi Salazar Sasaki100% (1)
- Presentation 1Document11 pagesPresentation 1Leo PrabhuNo ratings yet
- FAQ False or True LaborDocument2 pagesFAQ False or True LaborArifGusaseanoNo ratings yet
- PROPOSAL WRITING To Sir JaucianDocument21 pagesPROPOSAL WRITING To Sir JaucianKirby C. CatulinNo ratings yet
- Jurnal PICOS VK Zainudin HalidDocument11 pagesJurnal PICOS VK Zainudin HalidCahayastore CahayastoreNo ratings yet
- Intrapartum Fetal Monitoring Guideline - Physiological-CTG PDFDocument33 pagesIntrapartum Fetal Monitoring Guideline - Physiological-CTG PDFKovacs TiborNo ratings yet
- Northern Mindanao Medical Center Department of Obstetrics and Gynecology Schedule For November 2019Document8 pagesNorthern Mindanao Medical Center Department of Obstetrics and Gynecology Schedule For November 2019Janellah BatuaanNo ratings yet
- LaborDocument94 pagesLaborLany Cardente PascuaNo ratings yet
- Hydramnios and Premature Rupture of MembranesDocument5 pagesHydramnios and Premature Rupture of Membranessarguss14No ratings yet
- Emergency DeliveryDocument61 pagesEmergency DeliveryRam Kirubakar ThangarajNo ratings yet
- Early Initiation of BreastfeedingDocument2 pagesEarly Initiation of BreastfeedingMutia Salindri Putri100% (1)
- Effect of Antenatal Dietary Interventions in Maternal Obesity On Pregnancy Weight Gain and Birthweight Healthy Mums and Babies (HUMBA) Randomized TrialDocument13 pagesEffect of Antenatal Dietary Interventions in Maternal Obesity On Pregnancy Weight Gain and Birthweight Healthy Mums and Babies (HUMBA) Randomized TrialAripin Ari AripinNo ratings yet
- The Development of The Unborn Child.: Life Before BirthDocument3 pagesThe Development of The Unborn Child.: Life Before BirthRicson DrewNo ratings yet
- Healthy Mothers, Healthy Babies:: Taking Stock of Maternal HealthDocument12 pagesHealthy Mothers, Healthy Babies:: Taking Stock of Maternal HealthYurika Elizabeth SusantiNo ratings yet
- Complication of Labor-Dysfunctional LaborDocument25 pagesComplication of Labor-Dysfunctional Laborcn351073No ratings yet
- Copar-RU Maternal and Child HealthDocument16 pagesCopar-RU Maternal and Child HealthMichelle ThereseNo ratings yet
- Model Asuhan Kebidanan Berbasis Teori Helen Varney Dalam Deteksi Dini Preeklampsia Kehamilan Di RSIA Citra Keluarga Kota KediriDocument12 pagesModel Asuhan Kebidanan Berbasis Teori Helen Varney Dalam Deteksi Dini Preeklampsia Kehamilan Di RSIA Citra Keluarga Kota Kedirirosha yuliantiNo ratings yet
- DOLE Pushes For BreastDocument4 pagesDOLE Pushes For BreastCriselda Cabangon DavidNo ratings yet
- Acog Vbac PDFDocument14 pagesAcog Vbac PDFFrancyn Rossi YangsonNo ratings yet
- Roles and Duties of Bhws in Postpartum CareDocument18 pagesRoles and Duties of Bhws in Postpartum CareFret Ramirez Coronia RNNo ratings yet
- LHV 2022 TestDocument1 pageLHV 2022 TestMuhammad AliNo ratings yet
- Complications During Labor and BirthDocument4 pagesComplications During Labor and BirthAudree Bustamante100% (2)
- Vasa PraeviaDocument14 pagesVasa Praeviakhadzx100% (2)
- April ResumeDocument1 pageApril ResumeChristian jade QuijanoNo ratings yet