0% found this document useful (0 votes)
443 views9 pagesTuning Fork Tests
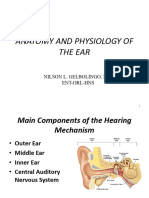
1. Tuning forks are acoustic resonators that emit a pure tone when struck. They are used in audiology tests to check hearing.
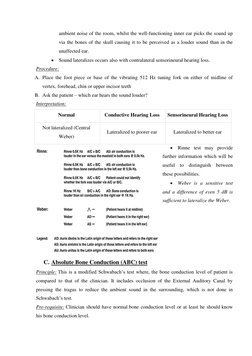
2. The Rinne test compares air conduction (sound through the ear canal) to bone conduction (sound through the skull). It detects conductive hearing loss. A negative Rinne indicates bone conduction is better, showing a problem transmitting sound through the ear.
3. Tuning forks are useful hearing tests because they produce a pure tone without overtones that could confuse results. Their frequency depends on material and temperature. Tests like the Rinne use them to check if sound is conducted properly through the ear.
Uploaded by
AndersonCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
443 views9 pagesTuning Fork Tests
1. Tuning forks are acoustic resonators that emit a pure tone when struck. They are used in audiology tests to check hearing.
2. The Rinne test compares air conduction (sound through the ear canal) to bone conduction (sound through the skull). It detects conductive hearing loss. A negative Rinne indicates bone conduction is better, showing a problem transmitting sound through the ear.
3. Tuning forks are useful hearing tests because they produce a pure tone without overtones that could confuse results. Their frequency depends on material and temperature. Tests like the Rinne use them to check if sound is conducted properly through the ear.
Uploaded by
AndersonCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
- Tuning Fork and Tuning Fork Tests
- Overtones and Sound Conduction
- Rinne Test