You might also like
- Diagnosis and Treatment of Chronic CoughFrom EverandDiagnosis and Treatment of Chronic CoughSang Heon ChoNo ratings yet
- Comparing Nasal Irrigation Devices for Pediatric SinusitisDocument6 pagesComparing Nasal Irrigation Devices for Pediatric SinusitisrivanaNo ratings yet
- A Randomized-Controlled Study Comparing The EfficaDocument7 pagesA Randomized-Controlled Study Comparing The EfficaaisyahNo ratings yet
- A Double-Blind Randomized Controlled Trial of Normal Saline, Lactated Ringer's, and Hypertonic Saline Nasal Irrigation Solution After Endoscopic Sinus SurgeryDocument7 pagesA Double-Blind Randomized Controlled Trial of Normal Saline, Lactated Ringer's, and Hypertonic Saline Nasal Irrigation Solution After Endoscopic Sinus SurgeryYasdika ImamNo ratings yet
- Kjped 57 479Document5 pagesKjped 57 479Vincent LivandyNo ratings yet
- Vol. 5 No. 2 April 2021 Jurnal Ilmiah KohesiDocument7 pagesVol. 5 No. 2 April 2021 Jurnal Ilmiah KohesiadindaNo ratings yet
- Topicaldrugtherapiesfor Chronicrhinosinusitis: Lauren J. Luk,, John M. DelgaudioDocument11 pagesTopicaldrugtherapiesfor Chronicrhinosinusitis: Lauren J. Luk,, John M. DelgaudiomilaNo ratings yet
- A Randomized Controlled Study Comparing The Efficacy of Nasal Saline Irrigation Devices in Children With Acute RhinosinusitisDocument20 pagesA Randomized Controlled Study Comparing The Efficacy of Nasal Saline Irrigation Devices in Children With Acute RhinosinusitisRahma DinaNo ratings yet
- Xylitol Nasal Irrigation in The Management of ChronicDocument6 pagesXylitol Nasal Irrigation in The Management of ChronicFlor OMNo ratings yet
- American Journal of Otolaryngology - Head and Neck Medicine and SurgeryDocument4 pagesAmerican Journal of Otolaryngology - Head and Neck Medicine and SurgerySyalara FatharaniNo ratings yet
- EfficacyDocument8 pagesEfficacyNia DefinisiNo ratings yet
- Polyp-Nasal SprayDocument6 pagesPolyp-Nasal SprayAldy BimaNo ratings yet
- 10.1007@s12070 014 0766 7Document9 pages10.1007@s12070 014 0766 7girish_s777No ratings yet
- SepDocument7 pagesSepyuyuNo ratings yet
- Infectious DiseasesDocument7 pagesInfectious DiseasesIneke FaradilaNo ratings yet
- 1339310072.0-S1475491612000033-mainDocument8 pages1339310072.0-S1475491612000033-mainMili NichițeleaNo ratings yet
- Prospective Evaluation of ClarithromycinDocument7 pagesProspective Evaluation of ClarithromycingekwahyuNo ratings yet
- Isotonic Saline Nasal Irrigation in Clinical Practice: A Literature ReviewDocument11 pagesIsotonic Saline Nasal Irrigation in Clinical Practice: A Literature ReviewrivanaNo ratings yet
- Saline Irrigation For Allergic Rhinitis (Review) : CochraneDocument4 pagesSaline Irrigation For Allergic Rhinitis (Review) : CochranefiskaderishaNo ratings yet
- Dina Nurhayati JournalDocument49 pagesDina Nurhayati JournalnindyarpNo ratings yet
- Jurnal Nacl 1Document7 pagesJurnal Nacl 1samie.sahari.alkesNo ratings yet
- Nasal saline irrigation efficacy pediatric rhinosinusitisDocument19 pagesNasal saline irrigation efficacy pediatric rhinosinusitistopNo ratings yet
- Comparison of Different Biologics For Treating Chronic Rhinosinusitis With Nasal Polyps: A Network AnalysisDocument18 pagesComparison of Different Biologics For Treating Chronic Rhinosinusitis With Nasal Polyps: A Network AnalysisZha Zha Nurul ZahraNo ratings yet
- S0301054620300264Document8 pagesS0301054620300264Niken KuncorowatiNo ratings yet
- Journal Reading: Nindya Riesmania P 30101206686Document50 pagesJournal Reading: Nindya Riesmania P 30101206686nindyarpNo ratings yet
- The Use of Inhaled NaceDocument7 pagesThe Use of Inhaled NaceYondi Piter PapulungNo ratings yet
- Lack of Efficacy of Long-Term, Low-Dose Azithromycin in Chronic Rhinosinusitis: A Randomized Controlled TrialDocument12 pagesLack of Efficacy of Long-Term, Low-Dose Azithromycin in Chronic Rhinosinusitis: A Randomized Controlled Trialpaijo09No ratings yet
- RCT (Randomized Control Trial)Document13 pagesRCT (Randomized Control Trial)yesicadeaNo ratings yet
- Jurnal THTDocument7 pagesJurnal THTFenti FatonahNo ratings yet
- jcm-12-03605-v2Document14 pagesjcm-12-03605-v2IgnacioCortésFuentesNo ratings yet
- Efectele IrigatieiDocument9 pagesEfectele IrigatieiKlaudynhooq JaudyNo ratings yet
- Medi 101 E29940Document5 pagesMedi 101 E29940Bella FebriantiNo ratings yet
- The Role of Doxycycline in The Management of CRSWPDocument6 pagesThe Role of Doxycycline in The Management of CRSWPLeonNo ratings yet
- Global Health Management JournalDocument7 pagesGlobal Health Management JournaldwiajaNo ratings yet
- Gargling Aloevera PDFDocument7 pagesGargling Aloevera PDFnalidaNo ratings yet
- Nasal IrrigationDocument16 pagesNasal IrrigationMaya AnggrainiNo ratings yet
- Significance of Nasal Polyps in Chronic Rhinosinusitis: Symptoms and Surgical OutcomesDocument5 pagesSignificance of Nasal Polyps in Chronic Rhinosinusitis: Symptoms and Surgical OutcomesbagasNo ratings yet
- Efficacy of Sinusitis UltrasoundDocument7 pagesEfficacy of Sinusitis UltrasoundYazid MultazamNo ratings yet
- Current Perspective On Nasal Delivery Systems For Chronic RhinosinusitisDocument20 pagesCurrent Perspective On Nasal Delivery Systems For Chronic RhinosinusitisiliyasNo ratings yet
- Effects of Surgical Treatment PDFDocument6 pagesEffects of Surgical Treatment PDFAssifa RidzkiNo ratings yet
- Kim 2012Document4 pagesKim 2012Aldi PutraNo ratings yet
- Trabajos Cientificos Sobre Agua de MarDocument10 pagesTrabajos Cientificos Sobre Agua de MarEnrique Climent SanchisNo ratings yet
- 834 3093 1 PB PDFDocument5 pages834 3093 1 PB PDFRegina Dwindarti DarostyNo ratings yet
- Cryotherapy For The Treatment of Chronic Rhinitis A Qualitative Systematic ReviewDocument11 pagesCryotherapy For The Treatment of Chronic Rhinitis A Qualitative Systematic ReviewAnneNo ratings yet
- Catgutpuntura Rinitis AlérgicaDocument11 pagesCatgutpuntura Rinitis AlérgicaDubichelNo ratings yet
- Weissman 2011Document5 pagesWeissman 2011gulararezendeNo ratings yet
- Ent-Hns Clinical Practice Guidelines: Acute Bacterial RhinosinusitisDocument11 pagesEnt-Hns Clinical Practice Guidelines: Acute Bacterial RhinosinusitisClarice VillanuevaNo ratings yet
- Comparative Study On The Efficacy of Non-Steroidal, Steroid and Non-Use Anti Inflammatory in The Treatment of Epidemic ConjungtivitisDocument6 pagesComparative Study On The Efficacy of Non-Steroidal, Steroid and Non-Use Anti Inflammatory in The Treatment of Epidemic ConjungtivitisVisakha VidyadeviNo ratings yet
- Efficacy of Dexamethasone Versus Fluticasone Nasal Sprays in Postoperative Patients With Chronic Rhinosinusitis With Nasal PolypsDocument5 pagesEfficacy of Dexamethasone Versus Fluticasone Nasal Sprays in Postoperative Patients With Chronic Rhinosinusitis With Nasal PolypsandiniNo ratings yet
- Treatment of Chronic Rhinosinusitis and Its Effects On AsthmaDocument7 pagesTreatment of Chronic Rhinosinusitis and Its Effects On AsthmaHalilGutajNo ratings yet
- 2010 - Zhang - EAP For AR Review PDFDocument8 pages2010 - Zhang - EAP For AR Review PDFmonday125No ratings yet
- CT Ratio Predicts Chronic Rhinosinusitis RecurrenceDocument8 pagesCT Ratio Predicts Chronic Rhinosinusitis RecurrenceyohanasmjtNo ratings yet
- Respirador BucalDocument8 pagesRespirador Bucalyessenia armijosNo ratings yet
- Articulos BronquiolitisDocument18 pagesArticulos BronquiolitisLaura López Del Castillo LalydelcaNo ratings yet
- Quality of Life After Functional Endoscopic Sinus Surgery in Patients With Chronic RhinosinusitisDocument15 pagesQuality of Life After Functional Endoscopic Sinus Surgery in Patients With Chronic RhinosinusitisNarendraNo ratings yet
- BJMP 2012 5 1 A512Document5 pagesBJMP 2012 5 1 A512maslikanNo ratings yet
- Ciclesonide Nasal Spray Effective for Seasonal Allergic RhinitisDocument1 pageCiclesonide Nasal Spray Effective for Seasonal Allergic RhinitisTata TataraNo ratings yet
- Efficacy of 25% Glucose in Glycerin and Honey in The Management of Primary Atrophic Rhinitis: A Comparative Prospective StudyDocument4 pagesEfficacy of 25% Glucose in Glycerin and Honey in The Management of Primary Atrophic Rhinitis: A Comparative Prospective StudySathiyamoorthy KarunakaranNo ratings yet
- The Besmart (Best Supportive Management For Adults Referred With Tonsillopharyngitis) Multicentre Observational StudyDocument6 pagesThe Besmart (Best Supportive Management For Adults Referred With Tonsillopharyngitis) Multicentre Observational StudyArizkamhNo ratings yet
- 23.06.24 - 2021-Chin J Integr Med.27 (2) .83 - Allergic Rhinitis - Acu GuidelineDocument8 pages23.06.24 - 2021-Chin J Integr Med.27 (2) .83 - Allergic Rhinitis - Acu Guidelinehj4gpphdysNo ratings yet
- SpaceX ProposalDocument6 pagesSpaceX ProposalTexas WatchdogNo ratings yet
- Conplast SP430Document2 pagesConplast SP430Tori Small100% (1)
- Basic Principles of Growth DevelopmentDocument19 pagesBasic Principles of Growth DevelopmentMikz Chua100% (1)
- HN E-Catalog CableDocument36 pagesHN E-Catalog CableMin Min AungNo ratings yet
- Nitrogen BlanketingDocument21 pagesNitrogen Blanketingrvkumar61No ratings yet
- TDI - Full Cave Diver Course: TDI Instructor Manual Part 2 - Diver Standards Date: 12/31/2009 Revision: 10.0Document5 pagesTDI - Full Cave Diver Course: TDI Instructor Manual Part 2 - Diver Standards Date: 12/31/2009 Revision: 10.0BraulioNo ratings yet
- Recommended Abma & Asme Boiler Water Limits Drum Operating Pressure (Psig) SteamDocument9 pagesRecommended Abma & Asme Boiler Water Limits Drum Operating Pressure (Psig) Steammaoc4vnNo ratings yet
- School and CentreDocument24 pagesSchool and CentreThrilling PrinceNo ratings yet
- Candidate 1 (Reservoir Engineering Panel) : ONGC SAMPLE INTERVIEW QUESTIONS (Based Upon Memory of Appeared Candidates)Document3 pagesCandidate 1 (Reservoir Engineering Panel) : ONGC SAMPLE INTERVIEW QUESTIONS (Based Upon Memory of Appeared Candidates)Neha AhiraoNo ratings yet
- Examination of Power Electronics (Pel) : AnswerDocument10 pagesExamination of Power Electronics (Pel) : Answerves vegasNo ratings yet
- Veterinarian Careers Projected Strong GrowthDocument6 pagesVeterinarian Careers Projected Strong Growthnmann7100% (1)
- Wolf Gone Wild - Juliette CrossDocument312 pagesWolf Gone Wild - Juliette CrossAbdelhediNo ratings yet
- Group 3Document11 pagesGroup 3Sharp MIER TVNo ratings yet
- Midterm Exam Reviewer: Surgical Handwashing QuizDocument9 pagesMidterm Exam Reviewer: Surgical Handwashing QuizOfficially RandomNo ratings yet
- CHEMDocument20 pagesCHEMValli RamalingamNo ratings yet
- How Yeast Growth is AffectedDocument9 pagesHow Yeast Growth is AffectedMisika AlamNo ratings yet
- Continuous Renal Replacement TherapyDocument9 pagesContinuous Renal Replacement Therapydoc_next_doorNo ratings yet
- VR-ForM-F06.10 (Hot Work Permit Request Form)Document1 pageVR-ForM-F06.10 (Hot Work Permit Request Form)imtz2013No ratings yet
- Project: M/S Cae-Gondia at Nagpur Cable Schedule For Proposed ProjectDocument26 pagesProject: M/S Cae-Gondia at Nagpur Cable Schedule For Proposed ProjectMurali MohanNo ratings yet
- Concrete Pump Hose TDSDocument2 pagesConcrete Pump Hose TDSAlaa Abu KhurjNo ratings yet
- Counter Argument Against Euthanasia (40Document4 pagesCounter Argument Against Euthanasia (40Daphniee PosingNo ratings yet
- The Four Common Types of Parenting StylesDocument11 pagesThe Four Common Types of Parenting StylesIka_Dyah_Purwa_1972100% (3)
- 20090716FoxReiki PDFDocument40 pages20090716FoxReiki PDFAgustina RomeroNo ratings yet
- Rear Derailleur: Important Notice Names of PartsDocument1 pageRear Derailleur: Important Notice Names of PartsRyan MulyanaNo ratings yet
- Product Brochure-Electronically Controlled Air Dryer-ECA PDFDocument4 pagesProduct Brochure-Electronically Controlled Air Dryer-ECA PDFAnonymous O0T8aZZNo ratings yet
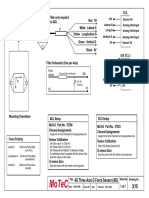
- Filter and wiring schematic for 3-axis ADL G-force sensorDocument1 pageFilter and wiring schematic for 3-axis ADL G-force sensorJuan Ramón Pérez LorenzoNo ratings yet
- Labrel 104-195Document1,014 pagesLabrel 104-195Maria Seleena HipolitoNo ratings yet
- CardiovascularDocument155 pagesCardiovascularEric VeranoNo ratings yet
- Aftercooler - Test: Shutdown SIS Previous ScreenDocument7 pagesAftercooler - Test: Shutdown SIS Previous ScreenKeron Trotz100% (1)
- Flame Amplifier HoneywellDocument8 pagesFlame Amplifier Honeywellgavo vargoNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (16)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- CBT Strategies: CBT Strategies for Overcoming Panic, Fear, Depression, Anxiety, Worry, and AngerFrom EverandCBT Strategies: CBT Strategies for Overcoming Panic, Fear, Depression, Anxiety, Worry, and AngerNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- How To Understand Your Anger For Better Mental Health: How To Control Emotions And Eliminate Stress In Your LifeFrom EverandHow To Understand Your Anger For Better Mental Health: How To Control Emotions And Eliminate Stress In Your LifeNo ratings yet
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Inmersion Into The Shadown Effective Method Of Dark Psychology: How To Use The Best Persuasion Techniques To Achieve Your Best Goals And How To Protect Yourself From Being ManipulatedFrom EverandInmersion Into The Shadown Effective Method Of Dark Psychology: How To Use The Best Persuasion Techniques To Achieve Your Best Goals And How To Protect Yourself From Being ManipulatedRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)