You might also like
- CosentyxDocument10 pagesCosentyxsamar RamadanNo ratings yet
- Ajcn 1013538Document11 pagesAjcn 1013538Tron TronNo ratings yet
- Clinical Nutrition: Emma Louise Metcalfe, Alison Avenell, Andrew FraserDocument8 pagesClinical Nutrition: Emma Louise Metcalfe, Alison Avenell, Andrew FraserHadi KuriryNo ratings yet
- Systematic Review: The Effects of Fibre in The Management of Chronic Idiopathic ConstipationDocument7 pagesSystematic Review: The Effects of Fibre in The Management of Chronic Idiopathic Constipationadinny julmizaNo ratings yet
- Imun 2Document12 pagesImun 2kadekapiklestariNo ratings yet
- Library 1555003975pdfDocument8 pagesLibrary 1555003975pdfAnghel MadalinaNo ratings yet
- 5 FullDocument13 pages5 FullVampaneZe ヴァンパネゼ ShuichiNo ratings yet
- 2016-Effectiveness of Aquatic Exercises in Women With.988491Document12 pages2016-Effectiveness of Aquatic Exercises in Women With.988491Deana Annisa AzizNo ratings yet
- 7051-Article Text-20588-1-10-20160303Document6 pages7051-Article Text-20588-1-10-20160303Mark JakoNo ratings yet
- Subjective Global Assessment in Chronic Kidney Disease - A ReviewDocument10 pagesSubjective Global Assessment in Chronic Kidney Disease - A ReviewDiana Laura MtzNo ratings yet
- Tratamiento N-ACETILCISTENIA FALLA HEPATICA AGUDA NO INTOX PARACETAMOLDocument12 pagesTratamiento N-ACETILCISTENIA FALLA HEPATICA AGUDA NO INTOX PARACETAMOLLauraQuiñonesNo ratings yet
- Effects of Probiotic Supplementation On Lipid Profile of Women With Rheumatoid Arthritis: A Randomized Placebo-Controlled Clinical TrialDocument7 pagesEffects of Probiotic Supplementation On Lipid Profile of Women With Rheumatoid Arthritis: A Randomized Placebo-Controlled Clinical Trialsufiah istthyNo ratings yet
- Efficacy and Safety of Avocado Soybean Unsaponifiables For The Treatment of Hip and Knee Osteoarthritis - A Systematic Review and Meta Analysis of Randomized Placebo Controlled TrialsDocument10 pagesEfficacy and Safety of Avocado Soybean Unsaponifiables For The Treatment of Hip and Knee Osteoarthritis - A Systematic Review and Meta Analysis of Randomized Placebo Controlled Trialsabo_youssof20047438No ratings yet
- Amonera 1Document7 pagesAmonera 1IstyNo ratings yet
- Jurnal 3Document6 pagesJurnal 3rifahNo ratings yet
- Zhu 2018Document10 pagesZhu 2018Luluil MunirohNo ratings yet
- Gluud 2016Document15 pagesGluud 2016FitriaNo ratings yet
- Ojsadmin, 7Document7 pagesOjsadmin, 7Veronika WijayaNo ratings yet
- Fphar 14 1186582Document18 pagesFphar 14 1186582yjbu0125No ratings yet
- Different Behaviour of Plasma Antioxidant Status After Red Wine Giammanco M, Et Al.Document8 pagesDifferent Behaviour of Plasma Antioxidant Status After Red Wine Giammanco M, Et Al.Marco GiammancoNo ratings yet
- Nicolau 2022Document6 pagesNicolau 2022Jefferson Souza SilvaNo ratings yet
- Chen 2021Document8 pagesChen 2021metha anandaNo ratings yet
- 250 Successful Management of Ankylosing SpondylitiDocument1 page250 Successful Management of Ankylosing SpondylitiAananda Raaj V MNo ratings yet
- Clinical Trial OA and Adverse EventsDocument15 pagesClinical Trial OA and Adverse Eventsdr_aasinNo ratings yet
- 326 PDFDocument13 pages326 PDFAnugrah Adi Santoso100% (1)
- Altman 2004Document8 pagesAltman 2004MeltemNo ratings yet
- Alcachofera en Sobrepeso PDFDocument9 pagesAlcachofera en Sobrepeso PDFIraidaCanudasHernandezNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 8: UrologyFrom EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyRating: 3 out of 5 stars3/5 (1)
- Anti-Inflammatory Diet in Rheumatoid Arthritis (ADIRA) - A Randomized, Controlled Crossover Trial Indicating Dieffects On Disease ActivityDocument11 pagesAnti-Inflammatory Diet in Rheumatoid Arthritis (ADIRA) - A Randomized, Controlled Crossover Trial Indicating Dieffects On Disease Activitysufiah istthyNo ratings yet
- Antonini Et Al-2016-Movement DisordersDocument8 pagesAntonini Et Al-2016-Movement DisordersMonika SarigNo ratings yet
- Zhu 2017Document9 pagesZhu 2017Hải TrầnNo ratings yet
- Nrgastro 2011Document2 pagesNrgastro 2011James LeungNo ratings yet
- Efficacy of Ursodeoxycholic Acid in Nonalcoholic Fatty Liver Disease: An Updated Meta-Analysis of Randomized Controlled TrialsDocument10 pagesEfficacy of Ursodeoxycholic Acid in Nonalcoholic Fatty Liver Disease: An Updated Meta-Analysis of Randomized Controlled Trialssteventanco1977No ratings yet
- Effects of LifePak Supplementation On Antioxidant Status and LDL-Oxidation in Healthy Non-SmokersDocument12 pagesEffects of LifePak Supplementation On Antioxidant Status and LDL-Oxidation in Healthy Non-SmokersCherry San DiegoNo ratings yet
- The Molar Ratio of Total Branched-Chain Amino Acids To Tyrosine Predicts A Digit Symbol Test Abnormality in Cirrhotic PatientsDocument11 pagesThe Molar Ratio of Total Branched-Chain Amino Acids To Tyrosine Predicts A Digit Symbol Test Abnormality in Cirrhotic PatientsThinh VinhNo ratings yet
- PIIS1063458410003584Document21 pagesPIIS1063458410003584abo_youssof20047438No ratings yet
- Jurnal Jaki Prof VeniDocument38 pagesJurnal Jaki Prof Veniiman prawiraNo ratings yet
- AlopurinolDocument10 pagesAlopurinoljoselyne carrascoNo ratings yet
- Nejm ArticleDocument10 pagesNejm ArticlePabloNo ratings yet
- JCSM 14 1199Document13 pagesJCSM 14 1199jamile oliveiraNo ratings yet
- Gastroparesis: A Comprehensive Approach to Evaluation and ManagementFrom EverandGastroparesis: A Comprehensive Approach to Evaluation and ManagementAnna IbeleNo ratings yet
- Curcumin LNDocument8 pagesCurcumin LNHend MahranNo ratings yet
- Efficacy and Tolerability of An Herbal Formulation For Weight ManagementDocument9 pagesEfficacy and Tolerability of An Herbal Formulation For Weight ManagementFaradina Zulaili Ifa EvendyNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 18: PsychiatryFrom EverandComplementary and Alternative Medical Lab Testing Part 18: PsychiatryRating: 5 out of 5 stars5/5 (1)
- Randomized, Double-Blind, Placebo-Controlled Glucosamine Discontinuation Trial in Knee OsteoarthritisDocument8 pagesRandomized, Double-Blind, Placebo-Controlled Glucosamine Discontinuation Trial in Knee OsteoarthritisFauzan AhmadNo ratings yet
- Effect and Interactions of Pueraria-Rehmannia and Aerobic Exercise On MetabolicDocument9 pagesEffect and Interactions of Pueraria-Rehmannia and Aerobic Exercise On Metabolicyhenti widjayantiNo ratings yet
- Pan. Metaanalisis of The Effects of Flaxseed On Blood LipidsDocument10 pagesPan. Metaanalisis of The Effects of Flaxseed On Blood LipidsJessica MoyaNo ratings yet
- SAMe For Liver DiseaseDocument15 pagesSAMe For Liver Diseasedivya tailorNo ratings yet
- Branched-Chain Amino Acids For People With Hepatic Encephalopathy (Review)Document4 pagesBranched-Chain Amino Acids For People With Hepatic Encephalopathy (Review)SupermanNo ratings yet
- Bislev 2018Document11 pagesBislev 2018Mahida El shafiNo ratings yet
- Efficacy and Safety of MerivaRDocument8 pagesEfficacy and Safety of MerivaRmazsamNo ratings yet
- Significance of Garlic and Its Constituents in Cancer and Cardiovascular DiseaseDocument3 pagesSignificance of Garlic and Its Constituents in Cancer and Cardiovascular DiseaseMaged Al-BadanyNo ratings yet
- Rehab September 2023Document8 pagesRehab September 2023Faeyz OrabiNo ratings yet
- The Liver & Neem: AntioxidantsDocument24 pagesThe Liver & Neem: AntioxidantsedyyantoNo ratings yet
- Arginine For HealthDocument6 pagesArginine For Healthmerry christiantiNo ratings yet
- Antioxidants and Physical Performance in Elderly Persons: The Invecchiare in Chianti (Inchianti) StudyDocument8 pagesAntioxidants and Physical Performance in Elderly Persons: The Invecchiare in Chianti (Inchianti) StudyRubí Gutierrez LopezNo ratings yet
- Alkaline IBSDocument9 pagesAlkaline IBSAnh LevanNo ratings yet
- Khannasharma 2017Document7 pagesKhannasharma 2017Imam IskandarNo ratings yet
- Evaluation of Handgrip Strength As A Nutritional Marker and Prognostic Indicator in Peritoneal Dialysis PatientsDocument9 pagesEvaluation of Handgrip Strength As A Nutritional Marker and Prognostic Indicator in Peritoneal Dialysis PatientsSalwiyadiNo ratings yet
- Zorov Et Al 2014 Mitochondrial Reactive Oxygen Species (Ros) and Ros Induced Ros ReleaseDocument42 pagesZorov Et Al 2014 Mitochondrial Reactive Oxygen Species (Ros) and Ros Induced Ros Release1766636545No ratings yet
- Zinkevich Gutterman 2011 Ros Induced Ros Release in Vascular Biology Redox 4444signalingDocument7 pagesZinkevich Gutterman 2011 Ros Induced Ros Release in Vascular Biology Redox 4444signaling1766636545No ratings yet
- Kal Ko601 - Anti Cd44icd Pab - DatasheetDocument1 pageKal Ko601 - Anti Cd44icd Pab - Datasheet1766636545No ratings yet
- Zorov 2006Document9 pagesZorov 20061766636545No ratings yet
- Ahn Et Al 2010 Electrophilic Tuning of The Chemoprotective Natural Product SulforaphaneDocument6 pagesAhn Et Al 2010 Electrophilic Tuning of The Chemoprotective Natural Product Sulforaphane1766636545No ratings yet
- Keap1 Recruits Neh2 Through Binding To ETGE and DLG Motifs: Characterization of The Two-Site Molecular Recognition ModelDocument14 pagesKeap1 Recruits Neh2 Through Binding To ETGE and DLG Motifs: Characterization of The Two-Site Molecular Recognition Model1766636545No ratings yet
- Research ArticleDocument12 pagesResearch Article1766636545No ratings yet
- 1 s2.0 S0891584914010120 MainDocument10 pages1 s2.0 S0891584914010120 Main1766636545No ratings yet
- 1 s2.0 S2213231723000356 MainDocument18 pages1 s2.0 S2213231723000356 Main1766636545No ratings yet
- 1 s2.0 S221323171500110X MainDocument28 pages1 s2.0 S221323171500110X Main1766636545No ratings yet
- 1 s2.0 S0167527302001894 MainDocument19 pages1 s2.0 S0167527302001894 Main1766636545No ratings yet
- Department of Education: Catherine B. Operaña, EddDocument5 pagesDepartment of Education: Catherine B. Operaña, EddMarica PangilinanNo ratings yet
- Nuevas Patologias Cie 10Document281 pagesNuevas Patologias Cie 10Ana guely santivañez mitmaNo ratings yet
- PERDEV DLL Unit 1 - M3 (Developmental Stages Handout)Document4 pagesPERDEV DLL Unit 1 - M3 (Developmental Stages Handout)Leonila MirandaNo ratings yet
- BioassayDocument38 pagesBioassayMuhammad Masoom AkhtarNo ratings yet
- Dental Informatics PlusDocument1 pageDental Informatics PlusNagendra TyagiNo ratings yet
- Assessment of PersonalityDocument3 pagesAssessment of PersonalityRahman ButtNo ratings yet
- Nepal New Emerging Pharma MarketDocument5 pagesNepal New Emerging Pharma MarketDeep_HeartNo ratings yet
- Moth Balls: Safety Data SheetDocument9 pagesMoth Balls: Safety Data SheethafilrediandikaNo ratings yet
- Smith Slides CH 4Document26 pagesSmith Slides CH 4USHA RANI SONOWALNo ratings yet
- Good Practice Review - 8 - Revised2 PDFDocument323 pagesGood Practice Review - 8 - Revised2 PDFsteppevosNo ratings yet
- Chapter 01Document22 pagesChapter 01kita5437100% (1)
- Cannabis-Infused Food and Canadian Consumers' Willingness To Consider "Recreational" Cannabis As A Food IngredientDocument7 pagesCannabis-Infused Food and Canadian Consumers' Willingness To Consider "Recreational" Cannabis As A Food IngredientCTV CalgaryNo ratings yet
- Short StoryDocument5 pagesShort Storyapi-376081909No ratings yet
- Notes On Critical Areas in Labor Law Part IiDocument66 pagesNotes On Critical Areas in Labor Law Part IipaulNo ratings yet
- 61Document11 pages61Mohammed Issa SalehNo ratings yet
- Hematoma: HaematomaDocument3 pagesHematoma: HaematomaBeeBeeSethNo ratings yet
- Cleft Lip and PalateDocument18 pagesCleft Lip and Palateicywitch100% (1)
- Intercostal Chest DrainageDocument6 pagesIntercostal Chest DrainageNovalis CrazyNo ratings yet
- Feline Injection-Site Sarcoma - Todays Veterinary PracticeDocument12 pagesFeline Injection-Site Sarcoma - Todays Veterinary PracticeBla bla BlaNo ratings yet
- WCLC2017 Abstract Book WebDocument700 pagesWCLC2017 Abstract Book Webdavid.yb.wangNo ratings yet
- Rhomboid Flap For Pilonidal Sinus - Our ExperienceDocument5 pagesRhomboid Flap For Pilonidal Sinus - Our ExperienceKhalidHussainNo ratings yet
- Primary Eye Care-A Manual For Health WorkersDocument76 pagesPrimary Eye Care-A Manual For Health WorkersRHU LOOCNo ratings yet
- Understanding Violence-Does Psychoanalytic Thinking matter-J.Yakeley&J.R.Meloy PDFDocument11 pagesUnderstanding Violence-Does Psychoanalytic Thinking matter-J.Yakeley&J.R.Meloy PDFMihaela BalionNo ratings yet
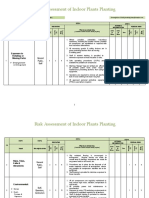
- Risk Assessment of Indoor Plants PlantingDocument5 pagesRisk Assessment of Indoor Plants Plantingطارق رضوانNo ratings yet
- Definitions of Human SecurityDocument10 pagesDefinitions of Human SecurityClandestain Zee100% (2)
- Readers Digest Asia Feburary 2021Document134 pagesReaders Digest Asia Feburary 2021FURY FURIONNo ratings yet
- Hyoscine ButylbromideDocument2 pagesHyoscine ButylbromideKenneth ColeNo ratings yet
- Isu Dan Etika Pada Perawatan Paliatif PDFDocument17 pagesIsu Dan Etika Pada Perawatan Paliatif PDFNatasya ChieCaem FunforeverNo ratings yet
- Responsible Tourism in Myanmar Current Situation and Challenges Red - 2 PDFDocument64 pagesResponsible Tourism in Myanmar Current Situation and Challenges Red - 2 PDFPyae PyaeNo ratings yet