0% found this document useful (0 votes)
1K views1 pageSedation Consent Forms.
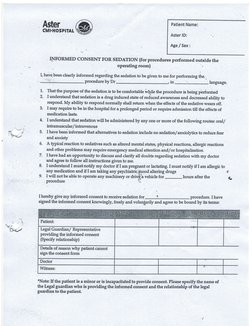
This document provides an informed consent form for sedation during a medical procedure outside the operating room. It outlines:
1) The patient's name, age, and sex.
2) That the purpose of sedation is to make the patient comfortable during the procedure and its effects are temporary.
3) Potential routes of sedative administration and alternatives to sedation.
4) Possible reactions to sedation and need for emergency care.
5) The patient's opportunity to discuss sedation and follow instructions.
6) Requirements to notify doctors of pregnancy, allergies, or other drug use.
7) Limitations on activities after the procedure.
The patient agrees to receive
Uploaded by
VishwaCrCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
1K views1 pageSedation Consent Forms.
This document provides an informed consent form for sedation during a medical procedure outside the operating room. It outlines:
1) The patient's name, age, and sex.
2) That the purpose of sedation is to make the patient comfortable during the procedure and its effects are temporary.
3) Potential routes of sedative administration and alternatives to sedation.
4) Possible reactions to sedation and need for emergency care.
5) The patient's opportunity to discuss sedation and follow instructions.
6) Requirements to notify doctors of pregnancy, allergies, or other drug use.
7) Limitations on activities after the procedure.
The patient agrees to receive
Uploaded by
VishwaCrCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
- Informed Consent for Sedation: Details the terms and conditions under which a patient consents to sedation during medical procedures, highlighting the importance of understanding risks and alternatives.